The area where the pelvis connects to the spine experiences significant stress when moving and changing body positions. Therefore, the inflammatory process of the sacroiliac joint, or sacroiliitis, occurs quite often. Its designation in the International Classification of Diseases ICD-10 is M46.1. The disease can be independent or a side effect of tumor processes, infectious or autoimmune problems. A significant number of cases of lumbar sacroiliitis are observed in patients who were previously diagnosed with tuberculosis or syphilis. Depending on the cause that caused the appearance of painful symptoms, the nature and severity of the inflammatory process are distinguished.
General information
What is sacroiliitis?
This is an inflammatory process of the sacroiliac (ileosacral) joint, which can be unilateral or bilateral. The paired sacroiliac joints connect the sacrum (a section of the spine made up of five vertebrae fused into one bone) and the ilium, forming the pelvic ring. This is a synovial joint, the articular surface of the sacrum has hyaline cartilage, and the surface of the ilium has fibrocartilage. The articular surface of the sacrum is uneven and it connects with the same irregularities of the ilium. The joint is held in place by strong interosseous sacrolumbar ligaments, which are attached to the sacrum and ilium.
The joint is physiologically adapted to the load, since its main function is support. It supports the body, reducing the strain when walking. The range of motion in the joint when walking is limited due to ligaments.
Most often, sacroiliitis is a symptom of various diseases of an infectious or autoimmune nature.
In this regard, the classification of diseases indicates the underlying disease ( Bechterew's disease , psoriatic arthritis , rheumatoid arthritis , various spondylopathies and dorsopathies ), in which unilateral or bilateral inflammation of the joint occurs. Sacroiliitis , which is not classified elsewhere, has an ICD-10 code of M46.1.
The anatomical structure of the joint contributes to low-symptomatic manifestations in the initial stages of the disease. Over time, the pain in the joint area intensifies, radiating to the buttock and groin. Subsequently, changes occur in the joint in the form of arthrosis and ankylosis , and the joint becomes a source of constant pain. Pain in the sacrum in women or men is most often associated with neurological manifestations of degenerative changes in this part of the spine, and patients do not receive the necessary treatment for a long time if there is a specific inflammation (tuberculosis, syphilitic, brucellosis) or autoimmune ( Bechterew's disease , Reiter's , psoriasis ). In this regard, you need to know how to make a diagnosis, signs of sacroiliitis of the iliosacral joint. In this short review we will look at all these questions. And also, which doctor treats sacroiliitis? Depending on the cause, this may be a rheumatologist or a traumatologist. However, initially you need to see a therapist and undergo a minimum of examinations, based on the results of which the doctor will give a referral to a specialist.
How to make an appointment with a rheumatologist at JSC "Medicine" (clinic of academician Roitberg)
To be examined by a qualified rheumatologist or traumatologist and receive recommendations for the treatment of sacroiliitis in our clinic, you can call +7 (495) 775-73-60. You can apply for an appointment online using the contact form on the website. Be sure to include your current phone number so that a call center employee can contact you and confirm your appointment time.
The clinic is located at the address: Central Administrative District, 2nd Tverskoy-Yamskaya Lane, 10. For those who travel by public transport, it is more convenient to get to the medical center from the Mayakovskaya, Belorusskaya, Novoslobodskaya, Tverskaya, Chekhovskaya metro stations.
Pathogenesis
The sacroiliac joint is complex, partly a synovial joint and partly a fixed synostosis. Considering the presence of powerful ligaments that support it, it is more correct to speak of a complex. There are pain receptors in the joint capsule, ligaments, and even in the subchondral bone, but there are fewer of them. Damage to any of the structures becomes a source of pain. The most common causes are spondyloarthropathy and arthrosis-arthritis , which develop against the background of specific factors - autoimmune, infectious or septic inflammation. Damage to the joint develops from a combination of two factors - pronounced axial load and rotation.
Physiotherapy for sacroiliitis
Today, there are many studies that confirm the effectiveness and benefits of physiotherapy for sacroiliitis. This is especially true for the rheumatological nature of the disease.
- Infrared radiation to the affected area. Infrared radiation has a warming and locally stimulating effect. As a result, healing processes are accelerated, immunity is stimulated, and infiltrates and other traces of chronic inflammation are reabsorbed.
- Laser radiation to the spine and the area of the sacroiliac joint. Under the influence of laser radiation, special sensitive molecules are activated in tissues and organs, which, interacting with surrounding cells, change the activity of metabolic reactions and increase oxygen consumption. As a result, cell division is stimulated, glucose production and fat breakdown are activated. All this increases the ability of tissues to regenerate (recovery).
- Ultraphonophoresis of anti-inflammatory drugs and local anesthetics. Under the influence of ultrasonic vibrations, the absorption of drugs is enhanced, the area of their distribution increases, and their therapeutic effect is enhanced.
- High-intensity pulsed magnetic therapy. Under the influence of a magnetic field, metabolic processes between cells change, metabolism increases, and the removal of decay products accelerates, which helps reduce the inflammatory reaction.
In addition to the listed methods of influence using physical factors, it is important to carry out correct gymnastics, which allows you to effectively combat morning stiffness of the joints, and also allows you to maintain adequate functional potential of the joint and limb.
Classification
Depending on the prevalence of the process in the joint, the following are distinguished:
- synovitis (only the synovial membrane is affected);
- panarthritis (all joint tissues);
- osteoarthritis (degenerative changes in joint surfaces).
According to the nature of inflammation and changes in the joint:
- specific (syphilitic, tuberculosis, brucellosis, yersinia);
- nonspecific (purulent) arises from a focus of osteomyelitis ;
- autoimmune (aseptic),
- degenerative-dystrophic.
Purulent damage to the joint is always one-sided - right-sided sacroiliitis or left-sided sacroiliitis develops. The onset is acute, there is a rapid course with high fever and chills, sharp pain in the back on the right (if right-sided sacroiliitis occurs) or on the left (left-sided). The patient's condition quickly deteriorates, and severe intoxication develops. The causes of purulent inflammation are osteomyelitis , a breakthrough of the abscess in the surrounding tissues, or infection of the joint due to an open injury to the pelvis and back.
Unilateral damage is also caused by:
- bone tumors;
- metastases of tumors of various localizations;
- infections ( tuberculosis , brucellosis , chlamydia , gonorrhea , syphilis );
- septic arthritis.
Bilateral sacroiliitis accompanies systemic diseases that occur with arthritis. What it is? Bilateral means damage to the joints on both sides, which can be symmetrical (on both sides in the same places) or asymmetrical (on both sides, but in different places of the joint).
Bilateral and symmetrical lesions are observed when:
- inflammatory bowel disease ( ulcerative colitis , Crohn's disease );
- ankylosing spondylitis ( ankylosing );
- condensing osteitis ( osteosclerosis ) of the ilium;
- multicentric reticulohistiocytosis (systemic disease with infiltration of organs by giant cells and histiocytes);
- Whipple's disease.
Bilateral lesions are of particular diagnostic importance in ankylosing spondylitis - sometimes this is an early sign of an incipient disease.
Bilateral but asymmetrical lesions are observed when:
- psoriatic arthritis;
- Reiter's disease;
- rheumatoid arthritis;
- osteoarthritis;
- relapsing polychondritis (systemic immune-inflammatory with gradual destruction of cartilaginous structures);
- Behçet's disease (systemic vasculitis).
Clinically Relevant Anatomy
The sacrum articulates with the ilia, which helps distribute the body's weight onto the pelvis. The SIJ joint capsule is relatively thin and often develops defects that allow fluid, such as joint effusion or pus, to leak into the surrounding structures.
Sacroiliac joint
- This is a true diarthrodial joint, the articular surfaces of which are separated by an articular space containing synovial fluid; the joint is surrounded by a fibrous capsule.
- The SIJ has unique characteristics that are not typically found in other diarthrodial joints.
- Composed of fibrocartilage in addition to hyaline cartilage, it is characterized by a discontinuous posterior capsule, with ridges and troughs that minimize movement and enhance stability.
- This joint is abundantly supplied with nociceptors and proprioceptors. Receives its innervation from the ventral rami of L4 and L5, the superior gluteal nerve and the dorsal rami of L5, S1 and S2.
Causes of pain in the sacrum
Primary inflammation of the sacroiliac joint can be caused by:
- traumatic injuries to bones, ligaments and muscles in this area;
- repeated excessive loads;
- local infection of the joint in open injuries;
- tumors and metastases (most often from the genital organs, intestines and lungs);
- pregnancy and childbirth.
Secondary inflammation occurs in the following diseases:
- Ankylosing spondylitis . Ankylosing spondylitis is a chronic inflammatory disease of the spine. The main symptom is damage to the sacroiliac joints. In the peripheral form of ankylosing spondylitis, damage to the sacroiliac joints occurs without significant pain, and therefore can only be detected by x-ray. The X-ray picture makes it possible to make an early diagnosis. In the initial stages, foci of subchondral osteoporosis appear, the contours of the joints become unclear and a false impression appears that the joint space is widened. Then erosion of the subchondral bone appears - the edges of the joint become uneven. Gradually, the joint space narrows and even disappears (ankylosis). The diagnosis of ankylosing spondylitis is considered reliable in the presence of a unilateral lesion of stage III-IV or bilateral lesion of stage II-IV, as well as one clinical manifestation. A potential causative agent of ankylosing spondylitis is Klebsiella pneumoniae.
- Inflammatory bowel diseases ( ulcerative colitis and Crohn's disease ). Sacroiliitis, usually symmetrical, is found in 25% of patients with ulcerative colitis and 15% with Crohn's disease. It may be a precursor to these diseases and the only localization on the joint side, but in 90% of patients it is asymptomatic. Its presence does not correlate with the severity of the inflammatory process in the intestine. Treatment of intestinal syndrome does not improve the clinical course of sacroiliitis. In parallel with inflammation of the sacroiliac joint, eye damage ( episcleritis , corneal ulcer ) is detected. Some patients experience transient sacroiliitis.
- Whipple's disease . Signs of this disease are articular syndrome, gastrointestinal damage ( diarrhea and steatorrhea ), paroxysmal abdominal pain, malabsorption and progressive weight loss. Unilateral or bilateral damage to the sacrococcygeal joint is found in 14% of patients.
- Psoriasis . With this disease, damage to the joints, including the sacroiliac joints, is common. Characterized by asymmetric arthritis , damage to the fingers and toes, distal interphalangeal joints, as well as asymmetric bilateral sacroiliitis. X-ray examination reveals periarticular osteoporosis , bone erosion, narrowing of the gap, bone ankylosis, and destruction of the vertebrae.
Infectious lesions of the sacroiliac joint are not so common; they are caused by:
- Tuberculosis . Tuberculosis of the joint is observed in 1-4% of patients. The primary focus is located in the ilium or sacrum. The defeat is one-sided. X-ray shows massive destruction of the sacrum and ilium. Sequestra occupy one third of the bone, the contours of the joint are not clear, and the edges are corroded. Sometimes there is a disappearance of the joint space (partial or complete).
- Yersiniosis . With this infectious disease there is an enteral phase, and then the disease passes into the generalized, allergic and secondary focal stages, which occur with exacerbations.
- Brucellosis . Brucellosis lesions are bilateral in nature and mask dystrophic diseases of the joint. Patients experience pain in the lumbosacral region when walking, stiffness of movement, and pain when going down stairs. An epidemiological history helps to establish a diagnosis.
- Syphilis . Syphilitic lesion occurs at the tertiary stage of the disease. It manifests itself as night pain, which is diffuse in nature. X-rays reveal minor changes that become pronounced over time.
If we consider this pathology in men, then it occurs with Reiter's disease , which affects mainly men. This is an autoimmune disease that affects the eyes ( conjunctivitis ), joints ( arthritis , including the sacroiliac joint) and the genitourinary system ( urethritis ). Ankylosing spondylitis is also more common (2-3 times) in men. Considering that men are more susceptible to significant physical activity and intense sports activities, this factor plays a big role in the occurrence of sacroiliitis .
The causes of pain in the sacrum in women, in general, do not differ from those in men. But there are still specific reasons, one of which is pregnancy . This is due to the fact that weight increases during pregnancy, and changes in hormonal levels cause stretching and weakening of ligaments and increased lordosis (excessive curvature of the lumbar spine with a convexity forward). The pelvis becomes “less rigid”, and this is favorable for childbirth. About 50% of women experience pain in the lower back and their source is the sacroiliac joints.
Pain in the sacrum in women can provoke difficult childbirth, during which pelvic tissues are damaged, ligaments, muscles and the pelvis are further stretched. In such cases, a course of nonsteroidal anti-inflammatory drugs and wearing a sacroiliac belt are recommended. It fixes tissue, stabilizes joints, and helps reduce inflammation. The recovery process can be lengthy and take from several months to a year. Complaints often recur during subsequent pregnancies and after childbirth.
Pain in the sacral region in women can cause malformations of the pelvis, disturbances in the formation of the sacroiliac joints, injuries to the pelvic bones, and pelvic distortion due to shortening of the leg. A difference in leg length of more than 5 mm already causes pain due to the increased load on the joint. It should be taken into account that in case of gynecological diseases, the sacroiliac joint is an area of referred pain. Also, pain in the sacral spine in women can be associated with a sedentary lifestyle, carrying heavy objects, prolonged static loads, running and jumping. Thus, if pain appears in the sacral spine in women, then this condition requires further examination to clarify the cause.
Treatment
The course of drug treatment for sacroiliitis includes taking antibiotics, anti-inflammatory drugs and corticosteroids. When choosing appropriate medications, the doctor takes into account the age and general condition of the patient’s body, the degree of damage to the joint and the characteristics of the course of the disease. When diagnosing complex purulent inflammation, surgical intervention is indicated.
If sacroiliitis is detected at the initial stage, the patient is guaranteed a complete cure while maintaining mobility and integrity of the joint. If the chronic stage develops, the likelihood of eliminating symptoms directly depends on the extent of inflammation and destruction of the articular joint.
Symptoms of sacroiliitis
The main symptoms of sacroiliitis are pain in the sacrum at night, after waking up, and when moving. The pain radiates to the buttocks and back of the thighs. All these symptoms resemble lumbosacral radiculitis. In addition, patients complain of morning stiffness.
For systemic diseases, the following are characteristic:
- bilateral lesion;
- widespread pain, covering the entire lumbosacral region and spreading to the thigh and buttocks;
- the pain intensifies at night and with prolonged stay in one position;
- reduction of pain when moving;
- stiffness in the morning.
In the chronic course of the disease, the pain is moderate and intensifies with prolonged stay in one position (sitting or standing).
Symptoms for injuries, infections and tumors:
- predominantly unilateral lesion;
- pain in the lower back and spreading to the leg;
- intensifies with abduction of the leg, pressure and movements;
- subsides at rest.
The most pronounced symptoms are observed with purulent lesions of the joint. With the infectious nature of the disease, the temperature rises, severe pain develops, which is why the patient takes a forced position (legs bent at the knee and hip joints). The pain intensifies when straightening the legs, turning, and when pressing on the wing of the ilium. On examination, sharp pain is noted in the sacroiliac joint. A positive test for the presence of sacroiliitis is painful extension of the hip while simultaneously fixing the pelvis in the prone position. Due to pain, patients require pain relief and assistance.
As we have found out, pain in the sacrum in men is often associated with ankylosing spondylitis. It is characterized by intensification at rest and in one position. The pain is especially disturbing in the second half of the night. Patients feel better when they move or exercise regularly. With this disease, planned activity is important, which prevents irreversible changes in the joint in the form of ankylosis .
Causes
Doctors usually distinguish two large groups of causes that provoke the inflammatory process.
The first is formed by autoimmune diseases, which are characterized by asymmetric inflammation. This group of causes is isolated separately because no additional symptoms are found in these joints. By inflammation you can simply diagnose the onset of a systemic process.
The second group of causes consists of diseases that are caused by ordinary arthritis, as well as other pathological processes. If the patient is right-handed, then sacroiliitis is usually found on the right side. Accordingly, left-sided sacroiliitis is detected in left-handed people.
In this group of reasons, it is customary to highlight the following:
- Incorrect biomechanics of the joint;
- Pregnancy status;
- Infectious diseases;
- Osteoporosis diagnosed in women at the postmenopausal stage;
- Developmental defects caused by complications during childbirth;
- A tumor condition developing in the bones of the pelvis, retroperitoneum and pelvic cavity;
- Features of work associated with prolonged sitting, causing weakening of the pelvic ring.
Tests and diagnostics
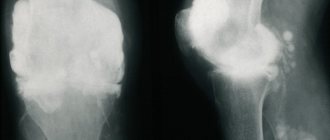
Radiography. True sacroiliitis in ankylosing spondylitis has characteristic radiological signs: unevenness of the joint space, subchondral sclerosis, widening of the joint space, and at a later date - narrowing. Radiologically there are 4 stages:
- Stage I - areas of erosion and changes in the joint space are absent;
- Stage II - narrowing of the joint space;
- Stage III - erosion, narrowing of the gap, severe sclerosis , bone “bridges” between the two surfaces of the joint and partial ankylosis ;
- Stage IV—overgrowth of the gap and complete ankylosis .
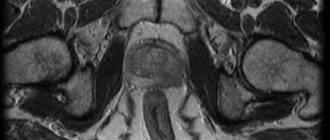
MRI is the most informative method that allows you to detect changes very early, when they are not yet detected radiographically. In the early stages, swelling of the articular surfaces is detected, there are still no changes in the surface of the cartilage, and the joint space is not changed.
CT scan. Detects changes in the second stage - narrowing or widening of the gap, cartilage defects in the form of small points. Later, foci of destruction are detected in the ilium.
For rheumatic diseases, additional tests are prescribed to identify specific antibodies (rheumatoid factor class IgA and IgM, antibodies to cyclic citrullinated peptide), HLA-B27 antigen in ankylosing spondylitis .
To diagnose sacroiliitis, special tests are used (Kushelevsky’s symptoms), which are performed by the doctor when examining the patient:
- When sharp pressure is applied to the crests of the iliac bones while the patient is lying on his back on a hard surface, pain occurs in the sacral area.
- Sharp pressure on the area of the ilium with the patient lying on his side also causes pain in the sacrum. The symptom is checked on both sides.
- The patient is positioned on his back, the leg is bent at the knee and laid to the side. The doctor rests his hand on the bent knee joint, while with the other hand he presses on the ilium on the opposite side. When performing a test in the presence of sacroiliitis, pain appears. The symptom is checked on both sides.
Reviews
Almost all patients who have encountered sacroyelitis claim that this pathology needs to be treated for a long time and with high quality. Only complex therapy will help overcome the disease.
Elena, 38 years old: “I had pain in the lower back that radiated to my hip, which appeared 6 years ago. I went to the doctor, who diagnosed me with sacroyelitis due to arthritis. I was prescribed anti-inflammatory drugs, electrophoresis, and magnetic therapy. In addition, I started visiting an osteopath, who turned out to be an excellent specialist, doing exercise therapy (first under the supervision of an instructor, and then on my own at home), and going to the pool. All these procedures together helped get rid of lower back pain.”
Anna, 35 years old: “I was diagnosed with left-sided sacroyelitis after childbirth. The pain was severe, treatment took place in a hospital. For about a month I went to physiotherapy, received NSAID injections, as well as vitamins. A therapeutic blockade helped with severe pain. Then I wore a corset for about 6 months and did gymnastics. After the course of therapy, the pain went away and didn’t bother me anymore.”
Andrey, 39 years old: “My sacroiliac joint became inflamed on the right, and then on the left. Pain appears on one side, then on the other, then on both sides. The pain gradually became stronger and stronger. I went to doctors for a long time, they prescribed a bunch of tests, but they couldn’t find the reason. Then I found a good specialist on the advice of friends, who found out that I have bilateral sacroyelitis of an autoimmune nature. I prescribed a bunch of medications and physical therapy, I hope it gets better. Although the doctor immediately warned that the treatment would be long.”
In children
Pathology of the sacroiliac joint occurs in adults, but in children it is an insufficiently studied pathology. Due to the complex anatomical structure of the joint, children rarely localize pain in this particular area, and this makes diagnosis difficult. The inflammatory process in the joint is preceded by injuries, hypothermia and acute respiratory viral infections.
During X-ray examination, in case of primary sacroiliitis, the process is localized in the middle and lower third of the joint (which corresponds to the synovial part of the joint), and in case of secondary sacroiliitis, it is localized in the upper third (this is the fibrous part). Most often, children experience purulent sacroiliitis , the clinical picture of which is dominated by abdominal, infectious-toxic and ischioradicular syndrome.
Infectious-toxic syndrome includes fever and intoxication (weakness, headache, nausea, disturbances in appetite and sleep, disturbance of consciousness, lethargy). With abdominal syndrome, abdominal pain, loose stools, intestinal paresis, tension in the muscles of the anterior abdominal wall and its soreness appear.
Ischioradicular syndrome is manifested by a forced position (lying on the back with straight legs). Minor movements of the body and legs cause severe pain. Due to the pelvic distortion, the leg is shortened by 1-1.5 cm on the affected side, and a curvature of the spine towards the inflamed joint is also detected. Children cannot lift their leg - only slight bending of the leg at the knee and hip joint.
In newborns and infants, inflammation of the iliosacral joint occurs with a severe general condition and a predominance of infectious-toxic syndrome with high fever.
In children 1-3 years old with this pathology, the condition is moderate or also severe. There is an infectious-toxic syndrome, and the abdominal syndrome occurs with periodic abdominal pain, muscle tension in the abdomen on the affected side. If the children still walk for the first two days, leaning on the front of the foot, and then refuse to walk. They experience minor paresis of the foot. In older children, ischioradicular syndrome predominates, and they can clearly localize pain.
If there is a purulent focus (phlegmon), surgical treatment is performed and antibiotics are prescribed (taking into account sensitivity to antibiotics). The duration of antibiotic treatment is 4-6 weeks. Sometimes after surgery, special immobilization or adhesive traction of the leg on the affected side is performed. Bed rest is observed for 1-3 weeks (depending on the severity and volume of the operation). After this, children begin to stand up and walk with crutches, protecting the leg on the affected side. Wearing the leg is allowed after 3-4 weeks, but it must be dosed.
If we consider ankylosing spondylitis, then 20% of all cases of the disease occur under the age of 15-16 years. 25% of sick children have a family history of seronegative spondyloarthritis . The disease usually begins at age 10, and patients begin to be examined at age 15, when the diagnosis of ankylosing spondylitis is made.
It is eligible in the presence of three syndromes:
- arthritis of peripheral joints;
- enthesopathies;
- spinal damage.
Enthesopathy is a pathological process at the sites of attachment of tendons, ligaments or joint capsules to the bone. The ends of tendons ( tendinitis ) and adjacent joint capsules may also be affected. In adolescents, the peripheral form of ankylosing spondylitis mostly occurs - initial damage to the sacroiliac joints, and then the addition of lesions to the knee and ankle joints, in which deforming arthrosis .
Thus, the first symptom is pain in the sacrum. Pain in the lumbosacral spine is accompanied by changes in posture and even swelling in the sacroiliac area. Involvement of the sacroiliac joints is observed at the age of 11-14 years, and then the large and medium joints of the legs are affected. Particularly characteristic of the juvenile form of ankylosing spondylitis is the involvement of the hip (in the first place), knee, ankle and tarsal joints. It is very important to suspect and identify the disease at an early age in order to carry out timely treatment and prevent the progression of the disease.
Prevention
Sacroiliitis is not classified as a rare phenomenon. First of all, this is due to a considerable number of professions that require a sitting position. Therefore, you should not neglect preventive measures to avoid health problems.
In order to prevent sacroiliitis from developing, infectious diseases should be treated in a timely manner, the immune system should be strengthened, and exercise should be performed. If possible, the sitting position at work should be varied by walking and warming up. If you have a diseased joint, the load on it should be minimized.
Following these simple recommendations will allow you to avoid unpleasant and even severe consequences of sacroiliitis, such as limited mobility of the spine in the lumbosacral region, up to complete loss of the ability to move.
List of sources
- Bunchuk N.V., Badokin V.V., Korotaeva T.V. Psoriatic arthritis. In the book: Rheumatology. National leadership. Ed. Nasonova E. L., Nasonova V. A. M.: GEOTAR-Media, 2008. 720 p.
- Silantieva T.S. Seronegative spondyloarthritis and ankylosing spondylitis: how to establish a diagnosis and not be late with treatment / Health of Ukraine. — 2021.— No. 7, pp. 37-38.
- Ostanina T.G., Evstigneev I.V., Cherny V.I., M.A. Beresten. Tuberculous sacroiliitis / Clinical immunology. Allergology. Infectology. — 2021.— No. 5, pp. 39-43.
- Slobodin T.N. Damage to the sacroiliac joint: diagnostic difficulties / Health of Ukraine. - 2021. - No. 5, p. 25.
- Badokin V.V. Psoriatic sacroiliitis and psoriatic ankylosing spondylitis // Consilium Medicum. 2008. No. 2.
Physical therapy
At an early stage we can use the pelvic girdle (during exercise and daily activities). This provides compression of the SIJ and reduces their mobility in “hypermobile” patients. The belt should be positioned posteriorly across the base of the sacrum and anteriorly under the anterior superior iliac spines. The belt can also be used in chronic cases.
At this stage, the patient should avoid movements such as bending, twisting and lateral bending to extreme positions. Maintaining correct posture is essential, so it is recommended to use lumbar support for your office chair and vehicle.
Once acute symptoms have subsided, the patient can move on to mobility and specific stabilization exercises. Stretching exercises can be used to maintain mobility of the SIJ and lower back. These exercises include side bends, knee tucks, and pelvic tilts to stretch the paraspinal muscles, glutes, and SIJ.
Patients with SIJ dysfunction may benefit from specific pelvic stabilization exercises, postural training, and core and lower extremity muscle training. The transverse abdominis, multifidus, and pelvic floor muscles are the muscles that need training the most. Training the transverse abdominis muscle independently of the other abdominal muscles is effective in providing greater SIJ stabilization and preventing weakness that can cause lower back pain. Therefore, it is necessary to teach the patient to contract the transverse abdominal muscles and multifidus muscles. In addition, the training program should include exercises for the specific joint contraction of the transverse abdominis and multifidus muscles. The best position for teaching the patient to contract these muscles together is on all fours. Once the patient can perform the muscles correctly in this position, they can move on to more intense training options.
Other examples of exercises may include: modified squats, weighted side bends, and gentle stretches. Strengthening the pelvic floor muscles is also important because these muscles counteract the lateral movement of the pelvic bones, which stabilizes the position of the sacrum. Activation of the transverse abdominis and pelvic diaphragm muscles will reduce vertical shear forces on the SIJ and increase its stability. After rehabilitation, aerobic exercises such as light jogging and water aerobics are prescribed to prevent recurrence of the disease.
If a patient has a leg length discrepancy or an altered gait pattern, the most reliable treatment is to correct the underlying defect.
Who diagnoses and treats sacroiliitis
If symptoms characteristic of the described disease are detected, you should contact an orthopedic traumatologist. In order to identify the nature of inflammation, the following diagnostic studies are prescribed:
- general tests;
- X-ray;
- radiography;
- MRI;
- laboratory tests for bacterial pathogens.
Treatment consists of eliminating the main cause of inflammation (bacterial infection, autoimmune reaction, etc.), relieving pain and increasing the body's resistance. For rheumatological forms, physiotherapy and physical therapy are relevant.
Pain in the sacral region is a good reason to see a doctor as soon as possible. Self-medication and folk remedies are ineffective in treating purulent forms and diseases caused by bacterial infections. At the same time, the lack of adequate treatment almost always leads to disability.
Consultations with a doctor online Taking care of your health is a life priority for everyone. Communicate with doctors online and receive qualified assistance without leaving your home. Try it Please note! The information on this page is provided for informational purposes only. To prescribe treatment, you must consult a doctor.
Preparing for MRI of the sacroiliac joints
Before examining the sacroiliac joints, you can adhere to your usual diet and physical activity, and lead your usual lifestyle. There is a small exception to this rule if a study involves the use of a contrast agent.
Sometimes the administration of the drug is accompanied by autonomic reactions (nausea, vomiting) that occur with a full stomach or on an empty stomach. On the day of the procedure, you should not overeat, and 30-40 minutes before the examination it is recommended to have a snack of fruit or a sandwich.
Extremely rarely, gadolinium (the substance on which the contrast agent is made) can cause allergic reactions. You need to tell your radiologist in detail about any drug intolerances you have. According to indications, an allergy test for gadolinium is prescribed. In people with underlying severe renal failure, the drug may worsen the course of the disease.
Therefore, in the presence of this pathology, preparation for MRI of the sacroiliac joints using amplification includes a study of blood creatinine levels.
Contraindications to performing MRI with a contrast agent are:
- enhancement study performed less than 36 hours ago;
- allergic reactions to gadolinium;
- chronic renal failure stage IV-V;
- severe bronchial asthma
- history of polyvalent drug intolerance.
It is necessary to bring medical documentation related to the disease of the sacroiliac joints to the examination:
- referral from the attending physician;
- discharge from hospital;
- data from previous studies, such as MRI, CT, if they were performed in another medical institution.
This will help the doctor make the right conclusions. If metal structures or artificial joints are installed in the body, you must submit a certificate from the hospital where the surgery was performed indicating the material from which the structure was made or stating that there are no contraindications for MRI. The restriction does not apply to dental braces and implants.
It is strictly forbidden to bring into the room where tomography is performed:
- watch;
- Hearing Aids;
- credit cards (they are damaged by magnetic fields), etc.
The MRI machine makes loud noises when operating, so don't be alarmed. You should use headphones to reduce the noise level. At the end of the procedure, you can immediately return to normal life if sedatives were not used due to claustrophobia. Do not drive while using sedatives. To find out how long you need to refrain from driving, consult your doctor.
A modern high-field tomograph is the key to high-quality research results.