Why does the infringement occur?
The causes of strangulated hernia are associated with a sharp or persistent increase in intra-abdominal pressure. This condition develops under the influence of external or internal factors:
- excessive physical activity;
- lifting heavy loads;
- chronic constipation;
- hacking cough;
- intestinal atony;
- weakened abdominal wall muscles;
- abdominal injuries;
- sudden weight loss;
- abdominal surgeries.
Internal organs caught in the hernial orifice are unable to correct themselves. Due to the overly stimulated tone of the muscles that form the hernial orifice, their size decreases, the organs become pinched, and signs of strangulation of the hernia appear.
With a hernia of the Spigelian line and other elastic strangulations, necrosis develops in the strangulated tissues within a few hours, and the risks of peritonitis and intestinal obstruction increase.
Complications
If parents delay visiting a doctor, then after 12 hours the child’s general condition becomes serious.
This is associated with the development of complications - intoxication syndrome with a rise in body temperature, intestinal obstruction or inflammatory damage to the peritoneum in the event of strangulation of intestinal loops. Due to compression, the blood supply is disrupted, the strangulated organ becomes necrotic, and diffuse purulent inflammation of the hernial protrusion may develop. In girls, the ovary may be strangulated, which, if assistance is not provided in a timely manner, becomes necrotic. In adulthood, this is fraught with the development of infertility and premature menopause.
Inguinal hernia strangulation can lead to sepsis and multiple organ failure.
Types of pathology
According to pathogenesis in surgery, the following types of strangulated hernias :
- elastic – associated with persistent spasm of the muscles of the anterior abdominal wall;
- fecal - develops as a result of a sharp overflow of the adductor part of the intestine located in the hernial sac.
Depending on which organ is pinched in the hernial orifice, there are pathologies with: pinching of the mesentery, parts of the intestine, omentum or stomach. With an inguinal hernia, the bladder, uterine appendages (in women), and spermatic cords (in men) may be compressed.
Special types of infringement include:
- Retrograde - at least three intestinal loops enter the hernial sac, two of which are in good condition, and necrosis develops in the third.
- Parietal - partial compression of the intestine in the area opposite the mesenteric edge.
Primary infringement is most often provoked by a single spasm of the abdominal wall muscles. Secondary develops as a complication of a previously diagnosed hernial formation.
External abdominal hernia
April 30, 2021
Abdominal hernia is a protrusion or protrusion of abdominal organs through defects or “weak spots” of the abdominal wall while the outer integument is intact. The weakest points of the abdominal wall, which are clinically important, include: the inguinal canal, the umbilical ring, the area of the white line of the abdomen, most often above the navel, the Spigelian line.
Abdominal hernias are among the most common surgical diseases; therefore, the treatment of such patients is not only a medical problem, but also a socio-economic one. The name “hernia” in Russian comes from the word “gnaw”, which indicates the unpleasant sensations that occur during the formation of hernias, and are manifested in the violation of “gnawing” the integrity of the abdominal wall and the release of its contents under the skin.
In the 5th century AD Celsus introduced the term “Hernia” (hernia), and therefore the science of studying hernias became known as herniology.
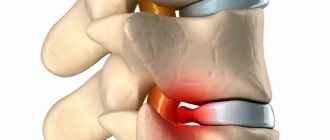
To understand the problem of the disease, let's take a little look at the anatomical features of this pathology. As can be seen in the diagram, the hernia consists of several parts: the hernial orifice, the hernial sac, the hernial contents and the external hernial membranes.
The hernial contents can be the abdominal organs or parts thereof (most often these are loops of the small intestine, omentum, wall of the colon or bladder). Thus, a hernia is like a sac with a small hole that allows the internal organ to come out.
The classification of external abdominal hernias is based on two basic principles:
- the name of the hernia corresponds to the anatomical areas where they form (inguinal, femoral, umbilical, postoperative or ventral hernias, as well as hernias of the white line of the abdomen and internal hernias);
- according to the ability of the contents of the hernial sac to be reduced into the abdominal cavity - reducible and irreducible.
An example of an internal hernia is a hiatal hernia. They can be of two types: sliding or paraesophageal. Hiatal hernia occurs more often in women than in men.
What are the causes of hernias?
The causes of hernias include:
- obesity;
- pregnancy: during pregnancy, the mother's abdomen stretches, which increases the likelihood of hernias;
- heavy lifting, severe cough, constipation: cause tension in the muscles of the anterior abdominal wall, which leads to increased intra-abdominal pressure;
- sudden weight loss: People who suddenly lose weight are at increased risk of developing a hernia;
- genetic predisposition: if one of your parents had hernias, then there is a chance that you will also have one;
- age: the older we get, the higher our chance of “earning” a hernia;
Other causes of hiatal hernia include obesity, pregnancy, very tight, tight clothing, sudden physical exertion, muscle tension, and coughing.
How to check if you have a hernia?
As a rule, the disease is characterized by the following features:
- the disease develops gradually and most often begins with discomfort during physical activity;
- hernial protrusion appears later, manifesting itself during exercise and disappearing at rest;
- Over time, the visible formation increases and ceases to be reduced or disappears at rest.
Pay attention to:
- the appearance of a protrusion (swelling, formation) in the area of the navel, groin, abdomen, which increases in a vertical position, during physical activity, when straining, and disappears or decreases in size in a horizontal position. The protrusion increases in size over time and takes on a round or oval shape. With indirect inguinal hernias, the contents of the abdominal cavity in men can descend into the scrotum.
- the appearance or intensification of pain in the protrusion area when doing physical exercise, lifting heavy objects, when coughing or sneezing, at the end of the day, or after a prolonged vertical position (standing still).
- The severity of the pain syndrome can vary: from discomfort to severe pain (the presence of pain syndrome more often indicates the occurrence of a complication - pinching).
Please note that if any symptom characteristic of a hernia appears, such as protrusion, discomfort, pain during physical activity, this is a reason to consult a doctor. A timely diagnosis will help avoid life-threatening conditions and serious complications.
What is the danger of a hernia?
A hernia of any location has a risk of developing complications.
Complications of hernias include:
- infringement;
- irreducibility;
- inflammation;
- coprostasis.
A strangulated hernia is the most common and dangerous complication, requiring immediate surgical treatment . In this case, the organs that have entered the hernial sac are subjected to compression in the area of the neck of the hernial sac in the hernial orifice.
Any organ located in the abdominal cavity can be pinched. More often, the loops of the small intestine and the greater omentum are pinched; the vessels supplying the intestine are compressed, which can result in necrosis (death of a section of the intestine), followed by the development of peritonitis. In such situations, in no case should you try to reduce the hernial protrusion into the abdominal cavity; you need to call and wait for doctors. A strangulated hernia always requires emergency surgical treatment, unlike non-strangulated hernias.
To avoid such complications, the presence of a hernia (i.e. hernia defect) is an indication for surgical treatment.
Treatment
Unfortunately, there are no conservative treatment methods. There are no pills or exercises to treat hernias. To eliminate a hernia, it is necessary to reduce the entire contents of the hernial sac, and the hernial orifice (the hole through which the hernia emerges) must be sutured to such a size that subsequently the hernia will not be able to exit through them again.
Currently, there are several methods of surgical treatment of hernias. The choice of technique depends on the type of hernia, the age of the patient, anatomical features, gender and the qualifications of the surgeon. The sooner an unstrangulated hernia is operated on, the better the prognosis for the patient’s health!
We treat inguinal hernias, umbilical hernias, femoral hernias, postoperative hernias, and hernias of the white line of the abdomen.
Our Outpatient Surgery Center actively uses hospital-replacing technologies, which have a number of advantages over hospitals:
The use of modern minimally invasive surgical techniques allows us to minimize pain in the postoperative period and ensure high cosmetic efficiency. We use only modern equipment, suture materials and mesh grafts from leading companies such as B|Braun, Johnson & Johnson, etc.
Modern methods of anesthesia allow surgical interventions to be performed without deep sedation of patients and intubation anesthesia, which significantly increases the safety of operations and reduces the time of the early postoperative period.
Surgical operations do not require hospitalization of the patient in a hospital and are performed in more comfortable conditions, and the ability to return to a familiar environment on the same day after the operation does not create psychological discomfort and saves time.
The low risk of postoperative infectious complications is ensured by the absence of hospital-acquired infection.
What to do if you have a hernia or suspect one?
Recommendations
- Contact a surgeon: only a qualified doctor can make the correct diagnosis. Whether you want to have surgery or not is up to each individual, but you need to know your diagnosis. And once the diagnosis is made, there are two options: either live with the hernia, or agree to surgery. Remember that a hernia tends to increase over time, it limits physical capabilities, introduces a cosmetic defect and can be strangulated at any time.
- Try not to lift weights: this will strain the muscles and create a lot of pressure in the abdominal cavity. It is necessary to lift weights correctly: when lifting something heavy, bend your legs at the knee joints, while your back should remain straight. The main work should be done by the leg muscles, not the stomach or back.
- Wearing various hernia bandages : indicated only for those people who are not able to withstand surgery. Surgery for such people for a hernia is contraindicated for health reasons. On the one hand, the bandage prevents the hernia from coming out; on the other hand, when worn for a long time, it contributes to a strong weakening and thinning of the connective tissues of the anterior abdominal wall - the so-called atrophy from inactivity.
- In case of hiatal hernia: do not eat foods that may irritate the stomach lining. Elevate the head of your bed a few centimeters to prevent stomach contents from refluxing into the esophagus. You should not lie down or go to bed immediately after eating.
What preventative measures are there?
If you are overweight: you need to watch your diet. This does not mean that you need to sharply limit yourself in food. Rapid weight change is very bad for health. After all, the body got used to its weight, it accumulated it gradually. If you suddenly go on a strict diet and force the body to lose more than 10% of its previous weight in a short period of time, this can lead to various diseases, including the development of a hernia. The body's regulatory systems do not have time to respond to such changes. It is considered normal to lose 1-2 kg per month. If you manage to lose a couple of kilograms, do not try to lose weight further. It’s better to try to keep your weight at this level for some time.
Prevent and treat constipation: Eat more fluids, fruits, vegetables and whole grains every day. Avoid "fixing" products, i.e. those that cause hard stools.
Reduce the amount of carbonated drinks and coffee in your diet. Exercise regularly. Follow a routine and eat at about the same time 3-4 times a day. If you feel the urge to defecate, do not delay it.
If the hernia suddenly hurts:
Take a horizontal position, relax your stomach and gently stroke it until it straightens and stops hurting. If the pain does not go away within an hour, call an ambulance; most likely, a strangulated hernia has occurred. In this case, immediate surgery is indicated, since the strangulated intestine may die and peritonitis may develop.
Strangulated hernia: symptoms of the disease
❗ What signs can be used to judge a developing pathology:
- sharp pain at the location of the hernial formation;
- muscle tension in the protrusion area;
- inability to straighten a pinched organ;
- absence of cough impulse transmission.
The clinic of a strangulated hernia is characterized by a general deterioration in the patient’s well-being. The skin becomes pale, the heartbeat quickens, and vomiting occurs. With the development of intestinal obstruction, vomiting becomes fecal in nature and becomes constant.
With prolonged strangulation, signs of painful shock appear - decreased blood pressure and tachycardia. At the site of the hernial protrusion, phlegmon forms - a purulent inflammatory process without clear boundaries of the lesion. If a strangulated umbilical hernia or other protrusion is not eliminated in time, the outcome is diffuse peritonitis.
Diagnosis of femoral hernias
In general, this hernia disorder is characterized by a rather unpredictable development, which is capable of sudden exacerbation, unlike, for example, inguinal hernias, which are easier to diagnose. The primary and mandatory diagnostic measure, when symptoms of a disorder are identified, is an immediate visit to the surgeon, who will prescribe further studies after a detailed examination and interview of the patient. For specialized and accurate diagnosis of the disease, a number of X-ray studies are used, in particular irrigoscopy and herniography (X-ray with the introduction of a contrast agent into the patient’s body). As part of the diagnostic analysis of the development of the disease, ultrasound examination of both the hernial formation itself and the organs of the genitourinary system can be very effective.
Diagnostic measures
✅ Diagnosing a hernia infringement is not difficult. In most cases, an external examination is sufficient, during which you can detect a painful protrusion in the groin area or on the anterior abdominal wall. A clear sign of the disease is the absence of a cough impulse and symptoms of intestinal obstruction.
, abdominal ultrasound and radiographic examination are prescribed for differential diagnosis .
Symptoms of femoral hernias
An obvious symptom of the development of a femoral hernia, especially in the early stages of the disease, is the observation of a small tumor-like protrusion in the area of the inguinal folds. In the reducible form of the disease, this symptom may disappear or be much less noticeable when the patient assumes a supine position. Further progress of the femoral hernia may be characterized by painful sensations in the area of the hip joints, aggravated not only by exercise, but also by walking or by changes in weather conditions.
How is a strangulated hernia treated?
⚠ Therapeutic tactics for strangulated hernia consist of emergency surgical intervention.
During the operation, the surgeon releases the compressed organs and examines the extent of their damage. If necrotic areas are found in the intestines, they must be removed immediately. The hernial opening is closed with special synthetic materials or the patient’s own tissues.
In case of a strangulated hernia of the white line of the abdomen and other parts of the abdominal wall, it is prohibited:
- adjust the protrusion independently;
- take laxatives;
- administer antispasmodics and analgesics.
Treatment
The most effective surgical therapy is femoral hernia repair, performed in a hospital. Treatment of a femoral hernia is carried out using hernioplasty (classical plastic surgery involves one’s own tissues), which involves suturing the hernial sac with a synthetic thread that dissolves over time. Also, instead of suturing the defects, using local tissues of the patient, a prosthesis made of synthetic mesh is installed, which blocks the femoral canal at the beginning of the hernial sac. Prevention of risky circumstances plays a very important role in preventing the development of this hernia disease. Among the measures that can reduce the risk of developing the disease, as well as its complications, include, for example, the use of bandages during pregnancy and significant physical activity, balanced nutrition, careful and consistent physical therapy of the muscles of the lower abdomen, timely treatment of diseases of the intestines and genitourinary tract, as well as refusal to smoking to prevent chronic cough.
Treatment of strangulated hernia in our clinic
Specialists at the herniology center in Kaliningrad are ready to provide routine care to patients with hernias of the anterior abdominal wall. Emergency operations in case of strangulation are carried out in emergency hospitals in the city.
☝ We recommend that you seek routine help in a timely manner and not wait for serious complications such as strangulated hernias. In this case, the risks of complications will be minimal, and surgeons will do everything possible to get you back to your normal life as quickly as possible.
To find out the details of hernia treatment at the clinic for reconstructive surgery of the anterior abdominal wall, sign up for a consultation by phone: ☎ +7 (4012) 971-961.
Classification
Femoral hernia
Based on the location of the exit gate, several types of femoral hernia are distinguished:
- Typical femoral hernia (exits through the inner part of the vascular lacuna, which turns into the femoral canal).
- Femoral lacunar ligament hernia (exits directly through a defect in the lacunar ligament).
- Femoral-total hernia of the vascular lacuna (the protrusion occupies the entire vascular lacuna).
- Femoro-intravaginal hernia of the vascular lacuna (exits in the area of the vagina itself).
- Femoral-lateral hernia of the vascular lacuna (exits between the artery of the iliac and pectineal ligament on the lateral side).
- Hesselbach's hernia (femoral hernia of the muscle lacuna) is formed in the area of the femoral nerve.
Based on the location of hernial protrusions, they are divided into:
- unilateral femoral hernias, 60% of which are hernias on the right and 30% on the left;
- bilateral femoral hernias account for about 10%.
Taking into account the clinic, the following are distinguished:
- reducible (retracts into place at rest on its own);
- irreducible (does not disappear when changing body position);
- disadvantaged.
Becker's hernia
Highlight:
- Primary Baker cysts, the formation of which occurs in the absence of any intra-articular pathology (found in children/adolescents).
- Secondary Baker cysts (formed due to damage to intra-articular structures).
According to their shape, cysts are classified as slit-shaped, crescent-shaped, oval, grape-shaped and horseshoe-shaped cysts.
How to prevent pain?
In order not only to remove, but to prevent the appearance of pain, you simply need to prevent the appearance of a hernia. Simple rules must be followed:
- move correctly and work on your posture, avoid flat feet;
- carry weights only evenly in a backpack on your back;
- when lifting weights, try to hold the load symmetrically, and in no case on one shoulder or in one hand;
- do not bend or turn while carrying a heavy load;
- monitor body weight, avoiding its excess;
- regularly try to hang on the horizontal bar or swim, unloading the spine, and do therapeutic exercises;
- after reaching a certain age, check the level of calcium in the blood, prevent osteoporosis;
- in winter, and especially in the presence of ice, you need to refrain from sudden movements, since falls and injuries are a risk factor for protrusion and hernia.
This way you can avoid severe back pain. If you already have a protrusion, or, moreover, a hernia, and they bother you regularly, then the best way is a modern minimally invasive surgical intervention.
Currently, they are being carried out with great success in Bulgaria, the Czech Republic, and including Russia. These are cold plasma and laser nucleoplasty, vaporization, endoscopic microdiscectomy. As a result, either the appearance of a hernia from the protrusion is prevented, or the cartilaginous protrusion itself is eliminated, and the nerve roots, muscles and ligaments no longer compress anything. Only surgery can lead to radical extraction and improve the quality of life.
Preparing for surgery
During the consultation, the surgeon will prescribe a set of necessary examinations:
- ECG.
- X-ray of the lungs or fluorography.
- Blood and urine tests - general, biochemical.
- Blood tests for hepatitis, HIV, syphilis, coagulation, blood group and Rh factor.
You should definitely tell your doctor about the medications you are taking; you may have to stop them for a while. Your doctor will tell you more about preparing for surgery during your consultation. You can undergo a comprehensive examination at GMS Clinic in 1 day.
List of sources
- Zatsarinny V.V., Muravyov S.Yu., Uspensky I.I. Morphological changes in the abdominal muscles in hernia patients. Current issues of clinical and experimental medicine: collection. abstract conf. young scientists. St. Petersburg; 2011:164-166.
- Styazhkina S.N. Abdominal hernia: textbook / comp. S.N. Styazhkina, V.A. Sitnikov, M.N. Klimentov et al. Izhevsk, 2011. 86 p.
- Makushin V.D., Danilova I.M. Backer cyst (review of the problem according to the literature) // Genius of Orthopedics. - 2000. - No. 1. - P. 110-113.
- Kamshilov B.V. Types of synovial cysts in the popliteal region // New Horizons: IV Trans-Ural. festival of scientific research, technical and applied creativity of youth: Abstracts. report region scientific-practical conf. - Kurgan, 2002. - Part 2. - P. 95-96.
- Mironov S.P., Orletsky A.K., Nikolaev K.A. Modern approaches to the diagnosis and treatment of popliteal cysts. Kremlin Medicine 2005; 2:33–6.
Forecast
Femoral hernia
With a non-strangulated femoral hernia, in most cases the prognosis is favorable and after suturing the hernia the patient returns to his usual lifestyle. In the absence of timely treatment, there is a risk of the formation of an irreducible hernia, and in 80-90% of cases strangulation occurs.
Baker's hernia
Cysts that have formed recently (usually after excessive physical strain on the knee joints) are characterized by a benign outcome. In the presence of persistent synovitis of the joint, the cyst becomes chronic and its contents are joint fluid. In chronic cases, the fluid in the joint capsule is partially resorbed, which leads to its thickening. With a long course, daughter cysts, synechiae and septa can form. In cases of rapid accumulation of effusion, rupture of the cyst is possible with the spread of articular fluid through the interfascial spaces of the lower leg.
Advantages of tension-free hernioplasty
Modern medicine has improved many surgical techniques for hernia repair, and one of the most minimally traumatic options is tension-free hernioplasty. This technique has undeniable advantages:
- Mild pain syndrome
- Fast rehabilitation (hospital stay is reduced to 1 day)
- No risk of relapse
- 2-3 weeks are enough for complete recovery
The entire operation lasts less than an hour and has an excellent cosmetic effect.
Tests and diagnostics
Femoral hernia
Early forms of femoral hernias present difficulties for their diagnosis, but diagnosing a complete hernia based on patient complaints and physical examination data does not cause significant difficulties. Of the instrumental methods, the most informative and mandatory is ultrasound, which makes it possible to identify their contents.
If necessary, the following may be prescribed: cystography , colonoscopy , cystoscopy , irrigography , CT . Differential diagnosis includes inguinal hernia , femoral artery aneurysm , abscess / tumor , thrombophlebitis .
Baker's hernia
The diagnosis is made on the basis of complaints, visual examination and palpation of the knee joint. Ultrasound/MRI are used as instrumental methods.