Intestinal obstruction is a complex of symptoms that develop against the background of a complete or partial disruption of the movement of food through the intestines. Intestinal obstruction is a dangerous condition, which, if left untreated, is inevitably complicated by peritonitis, intestinal necrosis and leads to the death of the patient. Therefore, you need to start treating this disease as early as possible. [1,2]
- Causes and types of acute intestinal obstruction
- Consequences of intestinal obstruction
- Symptoms of intestinal obstruction
- Diagnosis of intestinal obstruction
- Treatment of intestinal obstruction and first aid
Causes and types of acute intestinal obstruction
Depending on what caused its development, there are:
- Dynamic or functional obstruction. It develops due to a violation of intestinal motility - its spasm or paralysis.
- Mechanical intestinal obstruction. It develops due to the closure of the intestinal lumen and the impossibility of transit of its contents. Here they distinguish:
- Strangulated intestinal obstruction, from the Latin strangulatio - strangulation. It develops due to compression of the intestine or its mesentery, as a result of which the blood supply to the intestine is disrupted. This is a very dangerous condition as it can lead to necrosis of the intestinal wall.
- Obstructive intestinal obstruction. Develops due to blockage (obstruction) of the intestinal lumen by foreign bodies (calculi, parasites), tumor or scar deformation. [1]
Depending on the site of development, colonic and small intestinal obstruction are distinguished.
In oncology, intestinal obstruction most often has an obstructive nature and develops as a complication of colorectal cancer, when the tumor blocks the lumen of the colon, usually in its terminal stages. Obstruction can also develop as a result of compression of the intestine by a tumor of another organ, for example, the uterus or prostate gland. [3]
Small intestinal obstruction occurs less frequently. As a rule, its cause is carcinomatosis of the visceral peritoneum. Primary tumors in this region are extremely rare. [4,5]
Preventive actions
The effectiveness of treatment depends on the etiology of the disease and the qualifications of the surgeon, because accurate diagnosis and timely and correct treatment measures minimize the likelihood of complications. It is also necessary to take into account the age of the patient: older patients have an increased risk of complications.
Prevention is aimed at treating diseases that cause intestinal obstruction:
- control of helminthiasis;
- timely diagnosis and removal of tumors;
- prevention of adhesions;
- preventing traumatic injuries;
- healthy eating;
- the right way of life.
The multidisciplinary clinic CELT has a powerful diagnostic and treatment base and experienced specialists of the highest level.
Consequences of intestinal obstruction
The development of obstruction triggers a cascade of pathological processes that affect the body systemically. With tumor obturation, the onset, as a rule, is blurred due to incomplete occlusion of the intestinal lumen, but as the tumor grows, the situation worsens. Acute obstruction, as a rule, develops due to complete obstruction of dense feces in the area of the intestine narrowed by the tumor.
In the first time after the development of obstruction, there is an increase in intestinal peristalsis. It's as if he wants to overcome an obstacle. As intestinal contents accumulate, the intestinal wall becomes overstretched, water-electrolyte and metabolic disturbances occur, motor function sharply weakens, and then intestinal paralysis occurs.
At the second stage, disturbances in the secretory-resorptive activity of the intestine and disturbances in parietal digestion develop, the enzymatic activity of enterocytes is blocked, as they are rejected, and the regenerative activity of the crypts is first inhibited and then completely stopped.
Under such conditions, the activity of intestinal bacteria and the so-called symbiont digestion is activated. It is not physiological and is inferior in efficiency to normal, parietal digestion. As a result, rotting and fermentation occurs, as well as the accumulation of a large number of products of incomplete breakdown of proteins, some of which have a toxic effect. [9]
As the process progresses, the immune defense mechanisms are disrupted, which leads to the active proliferation of anaerobic bacteria that secrete exo- and endotoxins. They act systemically on the body - they disrupt tissue microcirculation, lead to central nervous system disorder, and disrupt cellular metabolism. Due to these effects, the permeability of the intestinal wall to bacteria increases, and they can spread into the abdominal cavity, blood and lymph flow, causing peritonitis and even sepsis.
Water and electrolyte disturbances also progress. Due to disruption of the intestine, increased filtration of fluid occurs; it is not absorbed back and accumulates in the afferent loop of the intestine. Under normal conditions, about 10 liters of liquid enter the gastrointestinal tract per day (including food, drink, saliva and secretions of the digestive glands). About 8-9 liters should be absorbed back, but this does not happen due to impaired reabsorption. Fluid accumulates in the adductor section of the intestine, causing it to expand. This, in turn, leads to reflex vomiting, which further worsens dehydration. Against this background, electrolyte disturbances quickly develop, which ultimately lead to renal and heart failure. [1.10]
Book a consultation 24 hours a day
+7+7+78
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Appointment with a surgical doctor (primary, for complex programs) | 3 000 |
| X-ray of the abdominal cavity (survey) | 2 400 |
| Diagnostic laparoscopy | 40 000 — 60 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Symptoms of intestinal obstruction
- Pain. This is one of the very first signs of intestinal obstruction. It is observed in absolutely all patients. With tumor obstruction, pain occurs suddenly, for no apparent reason, and may even be one of the first signs of cancer. It has a cramping character. The greatest pain occurs at the time of peristaltic contractions, after which it subsides a little for a couple of minutes. Gradually, the intensity of the pain increases and after a few hours it becomes unbearable. They subside only on the 2-3rd day, when paralysis of the intestine already develops - “noise at the beginning, silence at the end”, a symptom of “grave silence”, when there are no sounds of peristalsis at all.
- Vomit. If the obstruction is located at the level of the small intestine or the right part of the large intestine, vomiting will be present in the early stages, as a sign of reflex irritation of the gastrointestinal tract. If there is obstruction of the terminal sections, vomiting will most likely not occur at first, or it will occur at large intervals. During breaks, patients may suffer from nausea, hiccups or belching. If intestinal obstruction persists, vomiting becomes indomitable, first the stagnant contents of the stomach and then the intestines are released, up to vomiting of feces. This is a bad sign, because it indicates that vomiting is a symptom of toxic cerebral edema, and it cannot be eliminated by draining the gastrointestinal tract.
- Retention of stool. This symptom is observed with obstruction at the level of the sigmoid and rectum. If there is high obstruction at first, the stool may persist.
- Bloating. There are 4 signs here: asymmetry of the abdomen, palpable bulge of the intestine, peristaltic contractions of the intestine that can be seen with the naked eye, tympanic sound upon percussion.
- Bloody or mucous discharge from the rectum. They usually occur with cancer of the terminal sections of the intestine and are associated with the secretion of mucus by the tumor, its disintegration, or injury from feces. [1,4,6]
In the process of developing the clinical picture of intestinal obstruction, three periods are distinguished (see Table).
Table 1 - Clinical picture of intestinal obstruction.
| Period | Symptoms |
| Early – up to 12 o’clock | The main symptom of this period is cramping swelling in the abdomen. Vomiting develops rarely and only with obstruction (blockage) at the level of the small intestine. |
| Intermediate – from 12 hours to 24 hours | At this time, the symptoms continue to increase and turn into a detailed picture. The pain becomes intense and even unbearable, without contractions, an enlarged abdomen, vomiting, and signs of dehydration appear. |
| Late – more than 24 hours. | The patient's condition worsens, the temperature rises, and a systemic inflammatory response develops, including peritonitis and sepsis. Shortness of breath and heart failure worsen. [4] |
Treatment tactics
At the first symptoms of the disease, the patient must be immediately hospitalized in a hospital. Before being examined by a surgeon, it is prohibited to take painkillers or any other medications, or to cleanse the stomach and intestines, so as not to blur the clinical picture and cause harm.
If intestinal obstruction is diagnosed in its initial stage, conservative treatment methods can be used:
- Emptying the stomach and intestines from food and feces using probing and siphon enema.
- Taking antispasmodics in the presence of spasms or drugs that stimulate peristalsis in case of intestinal paresis.
- Intravenous drip infusions of saline solutions to achieve water-electrolyte balance.
- Colonoscopy for diagnostic and therapeutic purposes.
If a conservative approach to treatment does not eliminate the disease, it is necessary to think about mechanical obstruction or the development of complications and resort to surgical intervention.
The following surgical treatment options are used:
- unraveling intestinal loops;
- cutting adhesions;
- hernia repair in the presence of a hernia;
- excision of a necrotic area of the intestine;
- the application of a colostomy to remove feces outside (in case of malignant neoplasms and the impossibility of anastomosis).
After the operation, drug correction is carried out, which, as a rule, includes antibiotic therapy, detoxification measures, restoration of peristalsis, etc. The main goal of treatment is to save the patient’s life and prevent possible complications that may develop if the disease is not diagnosed and treated in a timely manner. The most life-threatening consequences are pain shock, sepsis and peritonitis.
Diagnosis of intestinal obstruction
The diagnosis of intestinal obstruction can be suspected based on the patient’s characteristic complaints. Confirmation is made using instrumental examination. [eleven]
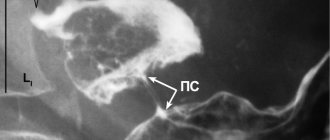
The simplest, fastest and most accessible diagnostic method is a survey radiography of the abdominal organs. The photographs reveal characteristic features:
- Kloiber's cup - dilated intestinal loops in the form of domes are visible, and there is a horizontal level of liquid in them. This painting resembles a bowl turned upside down. There may be several bowls; in the picture they are layered on top of each other.
- Intestinal arcades - arise due to swelling of the loops of the small intestine with gases; a horizontal level of fluid is visualized in the lower knees of the intestine.
- Kerking's folds - due to stretching of the jejunum on radiographs, it takes on the appearance of an extended spring.
- X-ray studies with contrast can also be used, for example, a study of the passage of barium suspension through the gastrointestinal tract, or irrigoscopy. However, these methods take a lot of time and delay the decision on the need for surgery.
Other diagnostic methods used:
- Endoscopic examination, such as colonoscopy or sigmoidoscopy. Such a study helps determine the localization of the tumor and the level of stenosis in the obstructed intestinal segment. In some cases, it is possible to pass a probe through the stenotic area and drain the afferent intestine. Colonoscopy is not performed if the patient’s condition is severe, there are symptoms of peritonitis and there is a risk of tumor perforation.
- CT. Using this study, it is possible to visualize the tumor, its size and the extent of stenosis (narrowing). In addition, the relationship of the cancer with surrounding tissues can be assessed and the presence of metastases can be determined.
- Ultrasound. In case of obstruction, an increase in the intestinal lumen, accumulation of air (gases) in it, and thickening of the intestinal wall due to inflammation are visualized. With the development of systemic inflammatory processes, free fluid may be detected in the abdominal cavity. [1,7,8]
Regional endoscopic anatomy.
In his work, the endoscopist should strive for the most accurate description of the level or boundaries of the location of the zone of pathological changes in the colon. Regardless of changes found in the distal colon, colonoscopy should consist of a complete examination of the entire colon, and in some diseases, the terminal ileum. The localization of the pathological focus is described in standard anatomical terms (cecum, colon, sigmoid colon, etc.). For a more detailed endoscopic description of the level of the lesion, the ascending, transverse colon, descending and sigmoid colon are divided into proximal, middle and distal thirds. In the rectum, the level of damage is expressed by the distance (in centimeters) from the edge of the anus. The close functional connection of the cecum, the bauginian valve and the terminal ileum, as well as the frequent combination of pathological changes in these sections, causes many authors to classify them as a separate ileocecal region of the intestine. In the colon, the distribution of the pathological formation is noted along the circumference (entire circle, semicircle, circles, etc.). In the rectum, due to topographical features (the proximity of many organs), the level of damage is supplemented by an indication of the orientation of the affected intestinal wall. Only the anal canal and the ileocecal region can serve as absolutely reliable landmarks in the colon. However, to assess the localization of the pathological focus, a number of techniques are used, the combined use of which in most cases makes it possible to accurately determine the location of the distal end of the apparatus in the intestine. Each individually is not flawless and their results can be considered with a certain degree of probability. These include:
- palpation determination of the location of the device through the abdominal wall (with pronounced adhesions, the reliability decreases);
- transillumination method (unconstant; in some cases it produces false positive results);
- taking into account anatomical landmarks (curves may not be pronounced; with severe edema, the shape of the circular folds may be altered; with elongation of the transverse colon or sigmoid colon, the number of haustrae may be increased.).
Treatment of intestinal obstruction and first aid
If a patient is suspected of intestinal obstruction, he is immediately hospitalized in a hospital, since the timing of treatment directly affects the prognosis. Both conservative and surgical methods are used.
As part of conservative therapy, the following procedures are used:
- Bowel decompression. For this purpose, removal of intestinal contents above the site of obstruction using probe aspiration or enemas can be used.
- Correction of water and electrolyte disturbances, replenishment of fluid loss. For this purpose, infusions of crystalloid solutions are prescribed.
- Pain relief. Antispasmodics and analgesics are prescribed, for example, atropine, platyphylline, etc.
- Replenishment of protein loss - infusion of protein drugs.
- To prevent infectious complications, broad-spectrum antibiotics are prescribed.
- Stenting of the intestinal lumen. Using an endoscope, a self-expanding stent is inserted into the site of intestinal obstruction. It pushes tumor tissue apart and maintains the intestine in a straightened state, ensuring the free passage of its contents. This way, time is gained for more thorough preparation for the planned intervention. [7,9]
This is especially important for cancer patients, since extensive tumor damage leads to the need for a colostomy. Placement of a stent for tumor obstruction allows time for neoadjuvant or perioperative chemotherapy. This will reduce the volume of the tumor mass and, possibly, even perform radical surgery. In other cases, this provides a chance to perform bypass anastomoses. For patients with end-stage colorectal cancer, who have a high risk of complications from surgery and anesthesia, stenting is the mainstay of treatment for intestinal obstruction. After the procedure, the patient continues to be monitored and surgical treatment is resorted to only in case of life-threatening complications. [1]
In all other cases, surgery is indicated, since the tumor will continue to grow and sooner or later a relapse of obstruction will occur.
In a compensated condition, surgical intervention can be delayed for up to 10 days; in a subcompensated condition, it is performed as early as possible, after the patient has stabilized. And if there are symptoms of peritonitis, emergency surgery is performed.
In any case, during surgery for intestinal obstruction, the abdominal cavity is opened (laparotomy) and revised. The location of the tumor, its relationship with surrounding tissues, and the presence of visible metastases are determined. An assessment of the viability of the intestinal wall is also performed to determine the extent of resection.
Ideally, radical removal of the tumor is performed through resection of the affected part of the intestine and restoration of intestinal continuity through anastomosis. Unfortunately, when obstruction develops against the background of a malignant process, it is very difficult and risky to perform such a volume of surgery in one stage, since there are extensive tumor lesions.
As a rule, in such cases palliative operations are performed:
- Performing a bypass anastomosis around a fragment of intestine with a tumor. Thus, the impassable (obstructed) section is excluded from the digestive chain.
- Stoma removal - a section of the intestine located above the site of obstruction is brought out onto the anterior abdominal wall in the form of an opening. Through it, the intestinal contents will be drained into a special bag - a colostomy bag.
Ostomy is a mutilating operation and is difficult for patients to endure morally. But in this situation, saving the patient’s life comes first. If possible, after stabilizing his condition and eliminating the consequences of intestinal obstruction, further treatment is carried out, for example, chemotherapy, radiation therapy, and, if the results are satisfactory, reconstructive interventions are performed to restore the integrity of the intestine. [1,5,7]
Book a consultation 24 hours a day
+7+7+78
Bibliography:
- Clinical recommendations: Acute intestinal obstruction of tumor etiology in adults. — Ministry of Health of the Russian Federation. — 2021.
- Methodological development for the practical lesson “Acute intestinal obstruction” Ed. USMA, Yekaterinburg, 2011 - 25 p.
- Clinical recommendations: Acute intestinal obstruction of tumor etiology. - Moscow, 2014.
- B. O. Kabeshev, S. L. Zyblev. Acute intestinal obstruction. — A practical guide for doctors. — Gomel, 2021.
- M.Yu. Kabanov, I.A. Solovyov, O.V. Balura. — Results of complex treatment of patients with acute intestinal obstruction of carcinomatous origin. - Bulletin of the Russian Military Medical Academy, 1(37)-2012.
- A.V. Pugaev, E.E. Achkasov, M.G. Negrebov. — Intussusception intestinal obstruction in adults. — Surgery, 5 — 2021.
- National clinical guidelines “Acute non-tumor intestinal obstruction”. — Russian Society of Surgeons. — 2015.
- Abdukarimova M.K. — X-ray diagnosis of intestinal obstruction. — Bulletin of AGIUV. — 2008, No. 5(8).
- Patrick Jackson, and Mariana Vigiola Cruz. — Intestinal Obstruction: Evaluation and Management, Am Fam Physician. 2021 Sep 15;98(6):362-367.
- Bertrand Trilling, Edouard Girard. — Intestinal obstruction, an overview — Rev Infirm. 2021 Jan;(217):16-8. doi: 10.1016/j.revinf.2015.10.028
- Thévy Hor, François Paye. — Diagnosis and treatment of an intestinal obstruction. — Rev Infirm. 2021 Jan;(217):19-21. doi: 10.1016/j.revinf.2015.10.030.
Clinical manifestations
Manifestations of the disease develop quickly, and it is extremely important to diagnose it in a timely manner.
Characteristic clinical symptoms of intestinal obstruction can be identified:
- severe pain;
- delayed bowel movement (lack of stool and gas);
- vomit;
- flatulence.
Delayed bowel movements and lack of natural gas release are another sign characteristic of colonic obstruction and are accompanied by bloating.
Abdominal pain is a mandatory symptom of the disease. The pain syndrome is always pronounced and marks the beginning of the development of the disease; it can be constant or cramping in nature with a gradual increase in intensity, up to the development of painful shock. The patient takes a characteristic body position that brings relief - he presses his legs to the anterior abdominal wall.
Vomiting, which does not bring relief, is also characteristic of this pathology, however, you should pay attention to some features of this symptom. Repeated vomiting at the very beginning of the disease may indicate that the problem is localized in the small intestine. Pathology located in the lower sections is accompanied by infrequent vomiting, which appears at the stage of intoxication.
If the patient is not helped at the onset of the disease, intoxication occurs, the clinical signs of which are:
- increased body temperature;
- development of peritonitis;
- increased frequency of breathing (shortness of breath);
- increased heart rate (tachycardia);
- sepsis;
- urinary disturbance;
- dehydration.
In the terminal stage of the disease, death can occur.