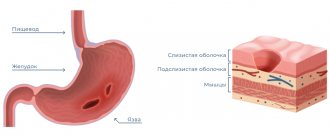
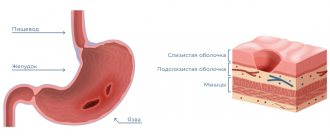
Erosive gastritis is an inflammatory disease. It affects the gastric mucosa, causing the formation of erosions of various sizes on it. These formations do not penetrate deep into the walls of the stomach and do not leave marks after healing.
It is the depth of penetration into the stomach wall that distinguishes erosive gastritis from an ulcer. The latter disease can affect not only the inner surface, but also deeper tissues and even the muscle layer.
Erosive gastritis is dangerous due to complications. Statistics show that a fifth of gastric bleeding is associated with erosions on the mucous membrane. Therefore, in modern gastroenterology, this form of the disease is increasingly referred to as “hemorrhagic gastropathy or gastritis” and “papular gastropathy.”
Erosive gastritis is a common pathology. A quarter of examinations for heartburn, abdominal pain, and nausea end with this diagnosis. The disease affects both men and women. The disease can develop at any age. True, young children are diagnosed much less often.
Studies show that in recent years, cases of diagnosing erosive gastritis have become more frequent. According to some studies, the incidence of diseases has increased tenfold. Scientists attribute this to an increase in the amount of stress, disruption of diet and quality of nutrition. This may also be due to improved diagnostic methods. When carrying out preventive examinations, the disease can be identified at the initial stage, even in the absence of complaints.
Consult a gastroenterologist
Don't delay treatment
Causes of erosive gastritis
In the vast majority of cases, the development of the disease is caused by Helicobacter pylori. However, doctors tend to believe that the mere presence of bacteria in the stomach is not enough. For the disease to appear, a combination of several factors is necessary.
The bacterium Helicobacter pylori was isolated in 1981. It is resistant to acidic conditions and is capable of secreting enzymes that weaken the protective environment of the stomach walls. By multiplying, this microorganism causes local inflammation and the formation of erosions. Helicobacter pylori is quite resistant to antibacterial drugs, which makes treatment difficult.
Research shows that more than 70% of the world's population is infected with Helicobacter pylori. At the moment, this is the most common infection. However, for various reasons, in most cases the presence of bacteria in the body does not cause the development of the disease and infection proceeds unnoticed.
In addition to the presence of pathogenic microorganisms in the stomach, the development of erosive gastritis can also be provoked by other reasons:
- severe stress
- chronic mental stress
- regular alcohol intake
- eating disorder with long periods of fasting
- eating spicy and salty foods
- smoking in the morning before breakfast
- taking certain medications
- liver and pancreas diseases
- chronic gastrointestinal diseases
- diabetes
- harmful working conditions
- reflux of the contents of the duodenum into the stomach
The combination of infection by pathogenic microorganisms with provoking factors reduces the protective function of the body. There is a release of bile, increased production of pepsin and acid. This significantly impairs the ability of the epithelium to regenerate and produce protective mucus and leads to the appearance of defects in the gastric mucosa and the formation of erosive gastritis.
Classification of forms of erosive gastritis
- Primary erosions (have no connection with previously identified pathology) and secondary (the result of progression, existing disease).
- Malignant (appears in the presence of an oncological process) and benign (can be single or multiple).
- Immature (young formations) and mature (have areas of tissue necrosis).
Based on the type and shape of formations on the mucous membrane, the following types are distinguished:
- superficial (small, flat in shape and with a distinct edge);
- full (raised above the surface of the mucosa);
- polypoid (can have a diameter of up to one and a half centimeters, do not heal for a long time and constantly worsen).
Symptoms of erosive gastritis
Patients suffering from erosive gastritis can present many different complaints, both specific and nonspecific:
- nausea and rare episodes of vomiting
- decreased appetite or complete absence of it
- increased gas formation
- heartburn
- belching
- pain in the epigastrium on an empty stomach or an hour and a half after eating
- sudden weight loss
- black stool due to bleeding
- vomiting black-brown mass
Patients may also complain of increased drowsiness and fatigue, decreased tolerance to usual stress, the appearance of shortness of breath and tachycardia. Such symptoms may indicate the presence of hidden bleeding.
The pathology symptoms listed above indicate that the disease may have symptoms of gastric bleeding and the presence of mucosal defects.
Erosion of the stomach and duodenum
Classification:
- Erosion as a manifestation of a malignant or systemic process in the gastric mucosa (cancer, lymphoma, Crohn's disease, etc.).
- Benign erosions: acute erosions (hemorrhagic);
- “chronic” erosion (erosion completa); erosions can be single or multiple;
- chronic erosive (lymphocytic) gastritis;
- erosive-hemorrhagic gastritis and duodenitis.
In addition, it is advisable to distinguish primary erosions and so-called secondary erosions that accompany the underlying disease.
Classification issues remain relevant to this day.
At the World Congress of Gastrointestinal Endoscopy, a Round Table meeting was devoted to terminology and semantics in endoscopy, in particular, it was discussed what terminology and classification of erosions to use when interpreting endoscopic examinations and when there is erosion as a complication or as a disease.
Attempts to classify erosive processes have been made by other authors. The definition of chronic erosions seems especially difficult.
In the medical literature, along with the term “chronic erosion,” the term “complete” erosion (erosion complete) is widely used, and with the development of numerous chronic erosions, the term “smallpox” (varioloform) gastritis, chronic erosive (verrucous) gastritis is used. In our opinion, the most The term “chronic erosion” seems acceptable, indicating the phase of the process (exacerbation or remission).
It is much more difficult to classify duodenal erosions. It is proposed to distinguish between acute and chronic erosions of the duodenum, but the authors admit that it is much more difficult to differentiate erosions of the duodenum than the stomach.
As a result of studies, it was established that the concentration of serum gastrin in patients with gastric erosions corresponds to normal values; in patients with erosive duodenitis and duodenal ulcer in the phase of incomplete scarring, the concentration of gastrin is almost the same. A slight difference was noted in the content of pituitary hormones (GH, TSH), progesterone and estradiol in patients with erosive duodenitis and with incomplete scarring of the duodenal ulcer.
Gastroduodenal erosions occur in various conditions of the acid secretion function of the stomach; There is no clear relationship between the tendency of erosion to heal and the level of gastric acid secretion.
An important practical issue is the question of the characteristics of the course of erosive damage (the duration of their existence, the tendency to relapse).
Studying the evolution of erosions and acute ulcers and determining the duration of their existence is a difficult task, largely dependent on the timing and thoroughness of endoscopic examination of the stomach. Dynamic endoscopic observation of patients with gastroduodenal erosions (endoscopy was carried out at various intervals from 2 to 7 times) showed that flat (acute) erosions last on average 7-10 days, but sometimes up to 2-8 weeks (depending on the prevalence and severity of the process ). Acute erosions almost always affect the proximal parts of the stomach (subcardial section, body of the stomach). Chronic erosions can be detected in the stomach for a long time (up to 6 years or more). Erosion of this type is localized, as a rule, in the antrum of the stomach. Duodenal erosions exist for a long time, for many weeks and months.
The question of the tendency of erosions to relapse is important. We concluded that only a portion of the erosive lesions recur. In these cases, chronic erosions occur in the antrum of the stomach, and flat defects of the mucous membrane are more often observed in the duodenal bulb. In most cases, there was no tendency for the reappearance of erosions of the stomach and duodenum.
Various clinical syndromes have been identified in patients with gastroduodenal erosions. Hemorrhagic syndrome is observed in approximately 20% of patients with erosive lesions of the stomach and duodenum, often in the form of repeated bleeding. Sometimes this syndrome is manifested by black stools (melena), less often by vomiting mixed with blood or “coffee grounds” vomiting, a collapsed state, and a decrease in hemoglobin. But, as a rule, the bleeding is hidden, so-called occult, in nature. Patients gradually develop chronic posthemorrhagic anemia. Signs of occult bleeding - general weakness, slowly progressing anemia, the presence of occult blood in the stool - are a direct indication for a thorough examination of the upper gastrointestinal tract. Of course, it is necessary to exclude damage to the colon and rectum during a comprehensive diagnosis. An ulcer-like syndrome is most often observed in patients with gastroduodenal erosions. Patients complain of periodic pain in the epigastric region associated with food intake, heartburn, belching, and nausea.
In patients with erosions and ulcers of the stomach and duodenum, symptoms of chronic diffuse liver diseases, lesions of the biliary tract and pancreas, diseases of the esophagus, tumors of the gastrointestinal tract, diseases of the cardiovascular system,
Dynamic endoscopic observation of patients with gastroduodenal erosions makes it possible to speak in favor of the hypothesis that acute and chronic erosions are stages of the same process. Chronic erosions can exist for many months and even years. They usually disappear, but sometimes transform into polyp-like folds or changes in the mucous membrane such as focal hyperplasia (“warty gastritis”).
One of the most difficult problems is the relationship between erosions and chronic ulcers. The hypothesis about the continuous development of the process from ecchymosis through hemorrhagic erosion to ulcer did not meet with unanimous support. Some scientists argue that erosions and ulcers are different lesions that do not transform into one another. There is doubt that erosion is a prestage of an ulcer. Others do not completely deny the possibility of acute erosions turning into chronic ulcers. T. loshida during dynamic endoscopic examination observed the transition of acute erosions into acute multiple gastric ulcers.
We observed that erosive gastritis and duodenitis often precede the development of duodenal ulcers. It is also possible to develop erosions at the site of a duodenal ulcer during its healing. As you know, Japanese researchers consider this outcome to be one of the options for healing duodenal ulcers. A unique variant of peptic ulcer disease can also be considered simultaneous or staged recurrent damage by erosions of the terminal part of the esophagus, the outlet part of the stomach and duodenum, which was observed in several patients in the autumn and spring periods over a number of years.
Thus, there is an undoubted relationship between gastroduodenal erosions and peptic ulcer disease. This is evidenced, firstly, by relapses of the ulcerative process, starting with erosive lesions of the stomach, the debut and healing of duodenal ulcers in the form of erosions of the bulb, as well as the very frequent combination of erosive gastritis and duodenitis with duodenal ulcer (in 37 and 44% of cases, respectively ).
Undoubtedly, the question of the possibility of transforming erosive lesions into polyps and (or) stomach cancer is always very important.
The hypothesis of Japanese researchers about the transition of erosions through the stage of verrucous changes into polyps and cancer has been studied in different countries. L. It is possible to transform chronic erosions into polypoid formations, the morphological study of which reveals moderate changes in the gastric glands and cystically dilated ducts, but at the same time does not reveal typical signs of an adenomatous polyp. A group of researchers did not observe the development of polyps in patients with chronic erosions for 4 years.
Sometimes erosions develop at the apex of polyps; in this case, it is difficult to resolve the issue of the primacy of erosive damage. Long-term dynamic observation of 90 patients with chronic erosions revealed their disappearance, or the appearance in their place of focal hyperplasia (what endoscopists usually call “warty”, or verrucous, gastritis of the stomach). Nevertheless, the presence of focal hyperplasia at the site of chronic erosions, the peculiarities of the histogenesis of the epithelium in their area, and the identification of chronic erosions at the apex of polyps do not exclude the possibility of the evolution of chronic erosions with focal foveolar hyperplasia into hyperplasiogenic polyps. In any case, in our opinion, there is a possibility of such a transition.
The hypothesis about the natural evolution of chronic erosions into a cancer process is supported by few authors studying this issue. The research results do not confirm the hypothesis about the transition of erosions into a cancerous process.
Studies of the severity of dysplasia found in various lesions of the stomach (polyps, ulcers, erosions, chronic gastritis) indicate that with gastric erosions, mostly mild or moderate dysplasia is detected.
In our opinion, these data serve as indirect evidence of the thesis about the insignificant probability of malignancy in chronic erosions, but, of course, it is difficult to completely exclude such a possibility in a particular case. Therefore, the doctor must carefully examine the patient using gastrobiopsy and morphological study of drugs over time.
Summarizing the results of observations and literature data, we can assume that it is not yet possible to confidently support the hypothesis about the natural evolution of chronic erosions into a cancer process. We should first of all exclude the possibility of the existence of an early form of cancer (type II c) or ulceration that arose against the background of an infiltrative process in stomach (cancer, lymphomatosis). We cannot exclude the possibility of the simultaneous existence of a cancer process and chronic erosions in the stomach.
It is necessary to remember the existence of an early cancer process in the form of erosive and ulcerative lesions, which has been proven by the work of Japanese doctors (type II c). Secondly, we should talk about gastric erosions that accompany the development of a cancerous process in the stomach or tumors of the colon and rectum.
How is erosive gastritis diagnosed?
Erosive gastritis has symptoms similar to other gastrointestinal diseases. Therefore, to clarify the diagnosis, additional examination is prescribed. Most often, doctors recommend the following laboratory and instrumental studies:
- a general blood test to determine the presence of anemia;
- determination of occult blood in feces;
- taking a section of the mucosa for cytology and histology;
- PCR for diagnosing Helicobacter pylori infection;
- fibrogastroscopy (FGDS) with a biopsy of the inflamed area;
- radiography with contrast.
Sign up for FGDS
Don't delay treatment
Directions for treatment in the presence of a chronic disease
When infected with Helicobacter pylori, the only cure is eradication of the infectious agent. The functions performed include preventing the spread of infection, preventing the possibility of bacteria becoming unsusceptible to antibiotics, reducing the duration of the course of therapy and the number of drugs and the risk of side symptoms.
Antibiotics like tetracyclines and penicillins and medications based on metronidazole, proton pump inhibitors, bismuth agents, and the like are used as tools that prevent the spread of bacteria or the exacerbation of chronic moderately atrophic gastritis
Treatment of erosive gastritis
For the treatment of pathology, conservative tactics are usually chosen. Surgery is very rarely required.
The basis of successful treatment is diet and regular medication. Doctors usually prescribe a set of tablets to destroy Helicobacter pylori, relieve symptoms of the disease and stimulate healing of the mucous membrane.
Since Helicobacter pylori is an antibiotic-resistant microorganism, a combination of three or four drugs is chosen to destroy it. Treatment is not easy and takes quite a long time.
If there is bleeding, in addition to taking medications, the doctor may recommend thermo- or electrocoagulation of the mucous membrane, laser exposure, staples or endoscopic stitching.
During treatment of the pathology, the patient should adhere to a fractional diet plan. There should be at least 5 small meals a day. To reduce the likelihood of mechanical damage to the mucous membrane during healing, you should eat grated food or cooked with steam. It is also necessary to avoid eating too hot or cold foods, and avoid eating salty, fried, fatty and spicy foods. Sodas, strong coffee, tea and alcoholic drinks are not allowed.
Nutrition for gastritis with low acidity
Fermented milk products are perfect for gastritis with low acidity.
With this type of gastritis, food is not completely digested because there are not enough digestive enzymes and insufficient hydrochloric acid is produced.
Products on such a diet should stimulate the production of gastric juice. The food receptors that trigger this mechanism are affected by the following foods and dishes:
- strong and rich broths and soups,
- sweet and sour fruits, citrus fruits,
- pickles and pickled vegetables,
- fermented milk drinks (kumys, ayran, kefir),
- sour fruit juices,
- sour non-carbonated mineral waters.
To stimulate the release of enzymes, chew food thoroughly.
Prevention
You can prevent the onset of the disease by observing personal hygiene measures, maintaining your diet, and giving up smoking and drinking alcoholic beverages. When working in hazardous industries, you should take precautions. When diagnosing diseases, carry out their timely treatment. You should also avoid stressful situations.
Why choose American Medical Clinic?
- Team of professionals. Candidates and doctors of medical sciences, professors and associate professors of departments of leading universities, doctors of the first and highest qualification categories work in the clinic 24 hours a day, 7 days a week. We work without holidays or weekends to ensure that you are healthy and happy.
- Regular professional development. Each doctor regularly takes advanced training courses, attends seminars, goes on internships, participates in conferences, and undergoes training abroad. This helps maintain the qualifications of doctors at the highest level. Today, the training of AMK doctors allows them to train young doctors, acting as experts at European-level seminars.
- Hi-tech. We regularly invest not only in training and professional development of personnel, but also in purchasing the most modern equipment from leading European manufacturers.
- The value of time. The American Medical Clinic has created all the conditions for a comfortable, comprehensive examination and diagnosis of a patient on the day of treatment.
- Trust from clients. Over 25 years of impeccable work, more than 500,000 patients have entrusted their health to us. More than 80% of patients recommend us to their family and friends.
- Guarantees. We are 100% responsible for the quality of the services provided, the high level of which is confirmed by many years of experience. The attention and sensitive attitude of doctors with more than ten years of experience in medical practice give a sustainable positive result.