Symptoms of duodenal diseases
Pathologies of the small intestine usually manifest as follows:
- Pain in the epigastric region, which occurs more often a few hours after eating, at night.
- Nausea.
- Lack of appetite.
- Heaviness after eating
- White coating on the tongue.
Also, duodenal diseases can be accompanied by symptoms that are characteristic of lesions of the pancreas, gallbladder and other organs. This indicates a significant spread of the pathological process.
Stages
Oncologists distinguish 4 stages of cancer of this localization. They differ in the size of the tumor focus and spread to adjacent tissues
:
- The first stage is a small tumor, with clearly defined contours, located in the area of the mucous layer with slight ingrowth into the submucosal layer. There are no metastases.
- The second stage is the spread of the tumor to the muscle layer, but without spreading to adjacent tissues. Single metastases to regional lymph nodes are possible.
- The third stage is a significant increase in the tumor with its extension beyond the intestine. Germination into surrounding tissues occurs and metastases occur.
- Stage four – the tumor is large, metastases form in distant organs, and lymph nodes are affected.
According to TNM classification
The severity of duodenal cancer is assessed based on three criteria.
T – this primary tumor can have 4 degrees:
- T1 – the tumor focus grows on the mucous membrane, growing into the inside of the intestine;
- T2 – the lesion extends to the muscle layer of the intestine;
- T3 – cancer grows into the outer wall of the intestine;
- T4 – tumor spread to surrounding tissues.
Damage to the lymph nodes is indicated by the following stages.
- N0 – tumor cells in the area of the lymph nodes are not determined;
- N1 – 1-2 lymph nodes are affected, which are located next to the intestines;
- N2 – tumor cells were detected in distant lymph nodes.
To determine the extent of the tumor, the M0 and M1 classifications are used. In the zero stage there are no distant metastases; in the first stage, duodenal cancer has given distant metastases.
Diagnosis of duodenal diseases
The main methods used in the diagnosis of duodenitis are as follows:
- Gastroduodenoscopy is the most informative method that helps to determine or exclude the disease. This endoscopic procedure determines whether there are inflammatory processes on the mucous membrane, whether erosions, duodenal ulcers, or duodeno-gastric reflux have developed. The study is carried out on an empty stomach with possible preliminary sedation of the patient.
- Examination of biopsy material or a urease breath test helps determine the presence of Helicobacter infection.
- X-ray examinations (performed less frequently).
When contacting a clinic for diagnostics, you must remember that most of the proposed procedures are performed on an empty stomach. A preliminary consultation with a gastroenterologist will allow you to properly prepare for the tests, which will significantly increase their information content.
Classification of chronic duodenitis
Classification of chronic duodenitis:
1) chronic duodenitis , mainly bulbitis , of acidopeptic origin;
2) chronic duodenitis, combined with atrophic gastritis or enteritis;
3) chronic duodenitis that developed against the background of duodenostasis;
4) local duodenitis (papillitis, peripapillary diverticulitis).
According to the endoscopic picture there are:
1) superficial chronic duodenitis;
2) atrophic chronic duodenitis;
3) interstitial chronic duodenitis;
4) erosive-ulcerative chronic duodenitis.
Treatment of diseases of the duodenum
Treatment of the digestive system is extremely variable. In the early stages, sometimes it is enough to reconsider your diet, and perhaps go on a strict diet and give up bad habits, such as:
- smoking;
- excessive caffeine consumption;
- alcohol consumption;
- abuse of spicy foods and synthetic carbonated drinks.
At this stage, it is important to exclude stress factors that affect the patient’s psycho-emotional state. Most diseases can be successfully treated with courses of drug therapy, which must be completed several times a year with regular adjustments of medications by a specialist.
At the Professor Gorbakov Clinic, treatment for diseases of the duodenum is selected depending on:
- identified pathology;
- patient complaints;
- the degree of disorders of the digestive system.
Our specialists also give dietary recommendations that help improve digestion, restore acidity regulation, normalize sphincter functions, and avoid consequences such as the development of diseases of various organs. In case of duodenal ulcer (peptic ulcer), consultation with a neurologist or psychologist is strongly recommended to exclude the influence of stress and psycho-emotional factors.
results
In all studies, two zones of narrowing were determined: contracted or opened PS and BDS (Fig. 1). Between the stomach and the duodenal bulb, a contraction zone of the PS, 0.75 cm long, is determined, which regulates the evacuation of chyme from the stomach. The contrast agent did not penetrate distal to the bulb due to contraction of the BJ. The width of the base of the bulb is equal to the width of the antrum of the stomach facing it.
Rice. 1. Sight radiograph of the gastroduodenal junction.
In 47 (56%) cases of group 1, no other sphincters were found in the duodenum. In cases where there was no tight filling of the duodenum with a contrast agent, the lacunae of the folds of the mucous membrane, smeared with barium, created a feathery relief. The width of different sections ranged from 1.2 to 4 cm. The widest was zone B, the less wide was zone A, and the narrowest was zone B (see table). During fluoroscopy, the barium suspension quickly and without delay entered the jejunum.
Width of different sections of the duodenum and length of sphincters, cm
In 16 observations, a narrowing was detected in the second part of the duodenum at a distance of 2-3 cm caudal to the apex of the bulb, but always cranial to the middle of the second part, where SO is usually localized. In this place, instead of a feathery pattern, 2-3 lines parallel to the intestinal wall were identified. Their length ranged from 1 to 3 cm (on average 2.05±0.09 cm) (Fig. 2). In all cases, this narrowing was localized in the same place, i.e., it was not related to peristaltic contraction.
Rice. 2. Simultaneous contraction of the Kapandji (1) and Ochsner (2) sphincters.
A second narrowing was found in 20 cases. It was located in the third part of the duodenum in projection LIII and was most often shifted to the left of the midline. In 2 cases, it represented the X-ray negative distance between the barium-containing sections of the duodenum (see Fig. 2). In 10 patients, instead of a feathery pattern, parallel folds of the mucous membrane are visible in this area. The length of the narrowing ranged from 2 to 4.2 cm (average 3.2 ± 0.15 cm). In 8 cases, it was not possible to measure the narrowing, since only the proximal edge of the narrowing was differentiated, over which the contrast agent stopped above the contracted zone was concentrated.
In 4 of 8 patients of group 2, after taking an acidified barium suspension, contraction zones in the duodenum were not always recorded and quickly disappeared. The X-ray picture did not differ from that in patients of group 1. Noteworthy was the slow evacuation from the duodenum due to the pendulum-like movement of barium between the sphincters. In 4 (50%) patients, the contraction in the third part of the duodenum turned out to be so strong and prolonged that it resembled that during SVBA (Fig. 3). However, during the study, the contraction zone disappeared without a trace.
Rice. 3. Radiographs of the gastroduodenal zone after taking barium with vitamin C. a - contraction of the Ochsner sphincter; b — pendulum-like movement of the contrast agent between the sphincters of Kapandzhi (1) and Ochsner (2).
In patients of the 3rd group, the width of the duodenum is significantly smaller in zones A and B compared to that in patients of the 1st group. The width of zone B was the same in both groups (see table). In almost all patients of group 3, diverticula were located in the descending and horizontal parts of the duodenum (Fig. 4). One patient had multiple diverticula: including in the stomach, 5 diverticula of different sizes in the duodenum, and at least one diverticulum in the jejunum. In one case, the diverticulum was located in the ascending part of the duodenum [5].
Rice. 4. Diverticulum in the descending part of the duodenum between the sphincters of Kapandzhi (1) and Ochsner (2).
On 23 direct radiographs (group 4) with contrast of the duodenum, we measured the distance between the sharply interrupted border of the dilated duodenum and the level of the SMA, if it was recorded on CT, MRI or midline LIII. This distance ranged from 2.5 to 4.6 cm (average 3.30 ± 0.15 cm). In 13 cases, a sharp narrowing of the duodenum began to the right of the right edge of the vertebra (Fig. 5, a, b). In 3 cases, it was possible to measure the length of the entire narrowed segment of the duodenum, since the contrast agent was located both cranially and caudally from it (see Fig. 5, c, d). Taking into account all research methods, in at least 29 (83%) of 35 patients with SVBA described in the literature, the length of duodenal contraction averaged 3.30±0.15 cm and only in 6 (17%) patients the length narrowing in the duodenum was within 1 cm.
Rice. 5. Radiographs of patients with SVBA. a — sharp compression of the duodenum occurred to the right of the right contour of the third lumbar vertebra (white arrow), a black arrow indicates ulcerative deformation of the duodenal bulb [6]; b — the distance between the compressed wall of the duodenum and the midline of the spine, where the aortomesenteric angle is located, is 4.6 cm (white arrow), the height of the third lumbar vertebra (black arrow) is 2.5 cm [7]; c — a black arrow indicates a radio-negative distance of 5 cm in length between the barium-contrasted proximal dilated part and the normal width of the abducens colon, the white arrow indicates the location of the SMA [8]; d - X-ray negative distance between the contrasted segments of the third part of the duodenum, corresponding to the narrow segment, is equal to the height of the third lumbar vertebra, i.e. 2.5 cm [9].
Anatomy
Most people have a variety of shapes. Even in the same person, the shape and location of the organ can change over time. First, let's talk about the structure of the duodenum.
Structure
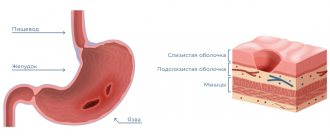
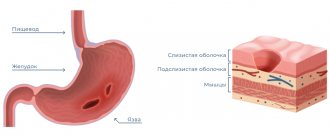
The organ has several layers:
- outer shell;
- muscle layer with longitudinal and circular layers;
- submucosa, thanks to which the mucous membrane can be collected in layers;
- mucous layer covered with villi.
Location
The organ has four main parts:
- Upper, or initial. It is located approximately at the level of the first lumbar vertebra or even the last thoracic vertebra.
- Descending. It is located to the right of the lumbar region and touches the kidney.
- Bottom, or horizontal. It goes from right to left, and then passes next to the spine and bends upward.
- Rising. Forms a bend and is located at the level of the second lumbar vertebra.
Where is the duodenum located? Most often it is located at the level of the second or third lumbar vertebrae. The location may differ for each person and is influenced by a large number of factors, such as age and weight. For example, in elderly and thin people the organ is located slightly lower than in young and well-fed subjects.
The photo clearly shows where the duodenum is located in humans
The intestine is in contact with other abdominal organs on all sides:
- liver;
- bile ducts;
- pancreas;
- right kidney;
- ureter;
- ascending colon.
The length of the duodenum is 25-30 cm.
Functions
Let us highlight the main functions of the duodenum:
- production of enzymes and duodenal juice necessary for normal digestion;
- motor and evacuation function, that is, responsible for moving food gruel;
- secretory;
- regulation of bile pancreatic enzymes;
- supporting communication with the stomach. She is responsible for opening and closing the gatekeeper.
- adjusting the acid-base balance of food. It makes the food bolus alkaline.
Since the duodenum is the initial section of the entire intestine, it is here that the processes of absorption of nutrients that come with food and drink actively occur. This is where the stage of intestinal digestion begins.
Digestion
After the food bolus enters the initial part of the colon, it mixes with bile, secretions of the intestinal walls, as well as fluid from the pancreatic ducts. The acidic environment of food is then neutralized by bile, thereby protecting the mucous membrane. In addition, bile breaks down fat and breaks it down into small emulsions, which speeds up the digestion process.
Under the influence of bile secretion, fat breakdown products dissolve and are absorbed into the intestinal walls, and complete absorption of vitamins and amino acids occurs. It is also worth noting that bile regulates intestinal motility, stimulating the contraction of its muscles. Thanks to this, the food bolus moves faster through the intestinal lumen and is promptly evacuated from the body.
Pancreatic juice also plays an important role, with the help of which starch is digested, as well as proteins and fats. The duodenal glands produce intestinal juice, which mostly consists of mucus. This secret promotes better breakdown of proteins.
Considering all of the above, we can say that the duodenum plays a huge role in the digestive process. It saturates the food bolus with the necessary enzymes and ensures further digestion.
DPC ensures the normal course of digestive processes