What is anal itching (itching in the anus)
Anal itching is a pathological sensation of persistent itching in the anus.
It can be either an independent disease or a manifestation of other diseases, such as anal fissure, hemorrhoids, helminthic infestations, dysbacteriosis, diabetes mellitus, etc. If a person is bothered by itching in the anus, then he feels both physical and psychological discomfort. A person suffering from severe itching in the anus changes his usual lifestyle and experiences problems with sleep disturbances. If you do not pay proper attention to this problem, this can lead to scratching or the appearance of anal fissures, through which infection can occur. The consequences of particularly advanced cases can be very serious. The formation of ulcers, bleeding, and the disease becoming chronic are possible. In some cases, itching and burning in the anus are quite persistent, as a result of which it is not so easy to cure them.
Anal itching - causes
Many people wonder why there is itching in the anus. Below are the main and most common causes of itching in the anus, which can cause discomfort for people of all ages.
Anal itching after defecation can occur due to insufficient hygiene in the anus, which naturally leads to such an unpleasant burning sensation.
Periodic itching in the anus in older people is a fairly common complaint, which is explained by the consequence of natural dry skin. Itching in the anus may appear for the same reason in case of dehydration.
Another common cause of itching in the anal area is increased moisture in the anal area. This condition is typical for people with excessive sweating, and also occurs in people suffering from frequent diarrhea or fecal incontinence.
There are other everyday causes that can lead to itching and burning of the anus. Constant use of a hard washcloth, rough toilet paper, caustic detergents or difficult-to-rinse soap - all this can lead to such an unpleasant consequence as itching in the anus.
The use of certain medications, including certain types of antihemorrhoidal drugs, topical gels and ointments, and birth control suppositories, can also cause discomfort.
Eating certain types of food sometimes causes anal itching; lovers of hot, spicy foods mostly suffer from this. The components included in such products can cause irritation of the mucous membrane.
The most common cause of frequent and short-term itching in the anus is insufficient hygiene in the anus. Which naturally leads to skin irritation in this area.
In rare cases, mild itching in the anus may be a result of hair removal in that area.
There are a number of diseases that are accompanied by anal itching of varying intensity:
- Proctological diseases: sphincteritis, proctitis, anal fissure, hemorrhoids
- Gynecological diseases: inflammation of the external genitalia
- Viral infections: genital warts
- Fungal diseases: thrush, actinomycosis
- Dermatological diseases: seborrhea, lichen planus, inflammation of the sweat glands, psoriasis, atopic eczema)
- Diseases associated with metabolic disorders (pancreatitis, liver failure, diabetes mellitus, etc.)
- Other diseases: bacterial, helminthic infestations, pubic lice, scabies;
In addition, itching in the anus can be a consequence of neurosis or result from the use of certain medications.
There are cases when it is not possible to identify the cause of itching in the anus, then they talk about idiopathic itching, which is caused by a decrease in the contractile function of the sphincter and the secretion of mucus from the rectum, which leads to irritation of the skin around the anus.
It is worth noting that there is such a disease as chronic proctosigmoiditis, the course of which can be secretive. In this case, the only clinical symptom will be redness and itching of the anus. The occurrence of anal itching in this case occurs as a result of a sharp change in the acid-base balance of the sigmoid and rectum, as well as the presence of proteolytic enzymes in the feces, which leads to an increase in the amount of residual nitrogen in the perianal zone, which has an irritating effect on nerve receptors.
Many people have a question, what are the symptoms of anal itching? Usually the only manifestation of this disease is itching around the anus. If you do not pay proper attention to pain and itching, abrasions and scratches can form in the anus, subsequently the skin in this area becomes thinner and becomes susceptible to damage. Microtraumas can lead to infection of the body. Anal itching often occurs in the evening or at night, and thereby provokes insomnia.
There are two main types of anal itching, which are classified depending on the course of the disease.
Acute and severe anal itching mainly appears suddenly and is intense, while in the anus there is moistening of the skin, which leads to additional irritation.
The course of chronic anal itching is characterized by slow development with a gradual increase in discomfort. In this case, as a rule, the skin in the anus area is prone to dryness.
Causes of intestinal inflammation after radiation therapy
The following mechanisms underlie radiation damage to the intestine:
- Damage to the intestinal epithelium that develops under the influence of ionizing radiation. This leads to its focal necrosis, desquamation (peeling) and atrophy.
- Development of nonspecific inflammation of the mucous membrane and submucosa. The tissues are infiltrated by neutrophils, hyperemia, swelling, and bleeding are observed.
- Due to trophic disorders (arterioles are damaged), the blood supply to the affected areas of the intestinal mucosa deteriorates, which further aggravates ischemia and necrosis. As a result, atrophic changes progress with the development of fibrosis of the submucosal layer.
- Against this background, pathogenic flora begins to join, which causes infectious complications, including sepsis.
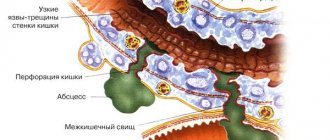
The end result of long-term trophic disorders of the intestinal wall and necrosis is the formation of strictures (narrowing of the lumen), the formation of fistulous tracts, the formation of telangiectasias and the development of bleeding from them.
How is anal itching diagnosed?
Despite the apparent simplicity of the symptoms of the disease, talking about the presence of itching in the anus and its treatment is possible only after consulting a proctologist. After all, this may be a manifestation of other diseases, so it is necessary to establish the cause of the itching, and in the case of a secondary symptom, only competent specialists can determine the underlying pathology. When diagnosing severe itching in the anus, a wide range of laboratory tests are used.
To establish the probable cause of the malaise, information may be required about the nature and characteristics of itching near the anus, its duration, intensity, and the relationship between the appearance of itching and diet, consumption of spicy foods or alcoholic beverages. Any observation of the patient can contribute to a quick diagnosis, which ultimately leads to a reduction in treatment time for the disease.
During the initial examination, the doctor notes signs of inflammation in the anus and takes a scraping. Also, each patient is required to undergo a three-time stool test to check for the presence of worm eggs.
When women complain of itching near the anus, an additional consultation with a gynecologist is carried out in order to exclude infectious diseases of the genital organs.
In some cases, if men complain of anal itching, an ultrasound examination of the prostate may be indicated.
If stool abnormalities are detected, a bacteriological analysis of stool is performed.
If it is necessary to examine the rectum to identify inflammatory bowel diseases, colonoscopy, irrigoscopy or sigmoidoscopy are performed. Colonoscopy, unlike other examinations, allows us to detect inflammation of the mucous walls of the intestine throughout the large intestine.
Another stage of the study for anal itching is a blood test for sugar content, as well as for the presence of metabolic disorders, which may be accompanied by skin itching.
If functional insufficiency of the anal sphincter is suspected, sphincteromanometry is performed.
If anal itching is accompanied by constant diarrhea or constipation, then in this case it is worth conducting research for the presence of pathologies of the upper digestive tract, such as ultrasound of the abdominal cavity and gastroscopy.
Classification of radiation proctitis
Depending on the severity, the following types of radiation proctitis are distinguished:
- Catarrhal proctitis. During the examination, a hyperemic, loose, edematous intestinal wall is discovered. There may be increased mucus production. This form of proctitis is considered mild.
- Erosive-desquamative proctitis. This form is manifested by foci of destruction of the epithelium with the formation of erosion - a tissue defect within the epithelial layer.
- Ulcerative proctitis - destruction spreads to deeper layers of tissue and involves the mucous membrane and submucosa in the process.
- Fistulous proctitis. A through perforation of the intestinal wall is formed with access to the pelvic cavity or with the involvement of nearby organs, for example, the bladder or vagina.
There is a classification of radiation proctitis based on the rectoscopic picture:
- There is local redness and friability of the intestinal mucosa, telangiectasias and dilated blood vessels are noted).
- Against the background of hyperemia and edematous intestinal mucosa, ulcers covered with a gray scab are found.
- Against the background of inflammatory lesions, strictures of the intestinal wall are detected.
- Against the background of ulcerative lesions, strictures and fistulas or intestinal perforation are detected.
Treatment of anal itching
Already at the initial stage of the disease, many wonder how to treat anal itching. The presence of just one symptom can create the impression that the disease is not serious and the feeling that treatment for itching in the anus should be very simple. But this is not always true, and the treatment of such a disease can be very lengthy.
The main direction of treatment for anal itching is to determine the cause of its occurrence and its subsequent eradication, while topical agents can be used to alleviate the patient’s condition.
If you have a question about how to treat anal itching, then you need to take into account, despite the desire for independent treatment, that only a doctor can provide qualified help. There are many manifestations of anal itching, and the reasons for its presence are completely different, and for each individual case it may be necessary to use specialized medications or undergo treatment procedures.
In cases where redness and itching of the anus are secondary, treatment is aimed at identifying and getting rid of the underlying pathology.
If the underlying disease has an infectious cause, then antibiotic therapy is prescribed; in cases of fungal infection, fungicidal agents are prescribed.
In cases of helminthic infestation, the patient is advised to take anthelmintic drugs.
It is worth noting that diseases in which inflammatory processes are observed in the large intestine require a full course of appropriate treatment. For hemorrhoids, anal fissure, and rectal prolapse, not only therapeutic treatment may be required, but also, in some cases, surgical intervention.
If itching near the anus acts as a clinical symptom of such serious pathologies as syphilis, diabetes mellitus, liver cirrhosis, hepatitis, then treatment can become quite lengthy and complex.
For topical use, special ointments, as well as microenemas (with 3 percent protargol or collargol, oils, and herbal decoctions) are used as a means to reduce discomfort and reduce itching. To suppress persistent pain, in some cases electrosleep and central electroanalgesia are used.
In rare cases, when the cause of anal itching cannot be identified, treatment must be applied symptomatically. Sedatives are prescribed, and careful, but not excessive, personal hygiene in the anal area is indicated, as well as limiting certain types of drinks and solid foods, which can lead to irritation of the mucous membrane and skin of the anal area. These are products such as alcohol, tea, cola, citrus fruits, chocolate, pepper, hot seasonings.
If the itching in the anus is constant, this can lead to scratching, which in turn contributes to bacterial skin lesions, eczema, ulcers, and bleeding.
It should be noted that when the first signs of the disease appear, it is necessary to consult a specialist, and not try to get rid of anal itching on your own, because only a doctor can competently answer the question about the reasons for its occurrence and the appropriate treatment after conducting the necessary research. By refusing to visit a specialist at an early stage of the disease, you increase the likelihood that the disease will progress to the stage of chronic pathology and then the treatment of anal itching will become longer and more labor-intensive.
Untimely initiation of therapy, as well as incorrect self-diagnosis followed by self-medication, in some cases can lead to a deterioration in the patient’s well-being and not only prevent recovery, but also lead to progression of the disease.
On methods of diagnosis and conservative treatment of anorectal diseases
Despite the fact that anorectal pathology has long attracted the attention of researchers, until now it has received insufficient attention. Basically, surgical methods of treatment are described, to the development of which A. V. Vishnevsky, A. N. Ryzhikh, M. Kh. Levitan, Zh. M. Yukhvidova, V. D. Fedorov, G. I. Vorobyov made a significant contribution.
The purpose of our article is to present traditional and modern methods of diagnosis and conservative treatment of anorectal diseases.
Diagnostics
Since ancient times, methods such as examination of the anus and digital examination of the rectum have been used to diagnose anorectal pathology. Later, rectoscopy began to be used. These techniques have not lost their importance to this day.
Examination of the anus is the first stage of examination if anorectal pathology is suspected. The method makes it possible to identify external hemorrhoids and hemorrhoidal fimbriae, external openings of fistulas, and anal fissures. With idiopathic anal itching and proctitis, weeping and excoriation of the skin around the anus can be observed; with paraproctitis localized in the subcutaneous tissue, hyperemia and swelling of the perianal skin can be observed. When examining the anus, you can see an anal polyp, prolapse of internal hemorrhoids, the mucous membrane of the anal canal, or all layers of the rectum.
Digital examination has always been and remains a mandatory part of a proctological examination. The importance of this method was repeatedly emphasized in his speeches by Academician V. Kh. Vasilenko. He was supported in this by Professor V.M. Mysh, who wrote: “The scope of diagnostic capabilities of sigmoidoscopy is limited to diseases of the intestine itself, while digital examination through the rectum is an extremely valuable and widely available method for studying both the intestine itself and a number of adjacent organs.” In the diagnosis of rectal cancer, digital examination is of particular importance and makes it possible in 88% of cases to detect a tumor, determine the degree of its displacement, the distance from the anus (which is important for choosing the method of surgical intervention), and the narrowing of the intestinal lumen. In addition to examining the rectum, this method determines the condition of neighboring organs (prostate gland in men, cervix and posterior surface of the uterine body in women).
Anoscopy - examination of the anal canal and lower ampullary part of the rectum using rectal mirrors is also included in the group of methods for mandatory examination of patients with anorectal pathology. During this examination, hemorrhoids can be identified, true polyps can be differentiated from hypertrophied anal papillae, which are hyperplasia of the mucous membrane in the area of Morganian crypts, resulting from chronic inflammation in anal fissures, hemorrhoids or proctitis.
Sigmoidoscopy has long been considered the main method for visual examination of the rectum and distal sigmoid. In subsequent years, the rigid sigmoidoscope was replaced by flexible fiberglass sigmoidoscopes, which make it possible to examine the entire left part of the colon, the most common location of tumors.
Total colonoscopy is performed in cases where sigmoidoscopy reveals polyps or malignant tumors in the rectum or sigmoid colon, when an inflammatory process is detected that is not limited to the distal colon, or there is a pathological discharge (mucus, blood, pus) in the intestinal lumen coming from proximal sections.
Ultrasonography. Currently, to recognize complicated rectal pathology, ultrasound devices equipped with rectal sensors have begun to be used, which makes it possible to obtain information about the transmural spread of the inflammatory process in the distal colon, the presence of infiltrates, fistulas and abscesses.
Thus, today colonoscopy and ultrasound using rectal sensors have joined the arsenal of the above-described and well-known diagnostic methods.
Characteristics of anorectal diseases
Hemorrhoids are one of the most common diseases; it affects 10% of the population. Among proctological diseases, hemorrhoids account for 40%.
The views of researchers on the etiology of hemorrhoids are contradictory. Congenital insufficiency of the venous system, venous stagnation, constipation, and disruption of the rectal sphincter mechanism were cited as causative factors. At the same time, none of the hypotheses based on the pathology of the venous system for a long time could explain the origin of the main symptom of hemorrhoids - the release of scarlet blood. In 1975, W. Thomson experimentally proved the existence of arterial and venous components of the hemorrhoid [9]. He formulated the cause of hemorrhoids as a primary weakness of the epithelium of the anal canal, leading to slipping and displacement of the anal “cushions,” which can occur with chronic constipation or prolonged straining during bowel movements [10].
Summarizing the research conducted to study the pathogenesis of hemorrhoids, G. I. Vorobyov and co-authors came to the conclusion that “the leading factors in the pathogenesis of hemorrhoids are dysfunction of the vessels that provide blood flow through the cochlear arteries and outflow through the efferent veins” [1].
There are several classifications of hemorrhoids [1, 4–6].
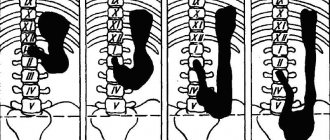
According to one of the latest classifications, hemorrhoids are divided according to their clinical course into acute and chronic, and according to their form into internal, external and combined. The chronic course of hemorrhoids, in turn, is divided into four stages: Stage I - discharge of blood from the anus without prolapse of hemorrhoids; II - loss of nodes with spontaneous reduction into the anal canal (with or without bleeding); III - periodic prolapse of nodes with the need for their manual reduction into the anal canal, stage IV - constant prolapse of hemorrhoids along with the rectal mucosa [1].
Harbingers of hemorrhoids over a long period of time (from several months to several years) may be discomfort in the anus or anal itching. The first and main symptom of the disease is anorectal bleeding of varying severity - from scanty bloody traces on toilet paper or stool to massive bleeding, leading to anemia in 1% of cases. The blood is usually bright red, but may be dark if it accumulates in the rectal ampulla. At the very beginning of the act of defecation, blood accumulated in the rectum can be released in the form of clots. More often, patients note the release of blood in the form of drops or a splashing stream. Occasionally, bleeding is observed outside the act of defecation. Hemorrhoids are also characterized by pain in the anus, which occurs during bowel movements, walking, and poor diet (eating spicy foods, alcoholic drinks). The cause of pain may be changes in the perianal area with external hemorrhoids or associated complications (anal fissure, thrombosis of the external hemorrhoidal plexuses). Anal itching occurs quite often with hemorrhoids and is a consequence of excessive mucus secretion, contamination of the anal area with blood and fecal particles. This constantly causes a feeling of wetness around the anus and soiling of the underwear. As a result, scratching appears and excoriation of the skin of the perianal area occurs (Fig. 1).
At the initial stages of the disease, conservative therapy is carried out. Attention is paid to nutrition. Alcoholic drinks and irritating foods contribute to increased hemorrhoidal bleeding, so alcohol, seasonings, spicy and salty foods are excluded from food. After defecation and toileting the anus, soft suppositories are inserted into the anus. For a long period of time, in proctological practice, suppositories of the following composition have been deservedly used for these purposes: Extr. Belladonnae 0.015; Novocaini 012; Xeroformi 0.1; But. Cacao 1.7. In case of bleeding, add S. Adrenalini 1:1000 gtt to the above composition. IY. Other candles listed below are currently in use.
In acute hemorrhoids and hemorrhoids complicated by thrombosis of the hemorrhoid, conservative therapy is first carried out, aimed at eliminating the inflammatory process and regulating stool. On the first day, cold is prescribed to the perineal area, in subsequent days - warm sitz baths with a weak solution of manganese after stool and rectal suppositories of the above composition, as well as suppositories or ointment Ultraproct, Posterizan, Proctoglivenol, Relief, Relief Ultra or Advance. These drugs are prescribed rectally in the form of cream or suppositories 2 times a day after stool and at night. In addition to local therapy, drugs that have a venotonic and angioprotective effect are prescribed orally. One of these drugs, Detralex, belongs to the group of flavonoids and is a combination of diosmin and hesperidin. The drug helps reduce the distensibility of veins, increase their tone, reduce stagnation and improve microcirculation. Detralex is prescribed 6 tablets per day for the first 4 days, then 4 tablets per day for the next 3 days.
The second drug in the same direction, Phlebodia 600, is non-micronized diosmin. The drug is prescribed according to the following regimen: 2–3 tablets per day with meals for 7 days, then, if necessary, treatment can be continued at 1 tablet 1 time per day for 1–2 months. For the same purpose, Diovenor 600, an analogue of Phlebodia 600, is used.
In case of prolapse of nodes, frequent exacerbations that do not respond to conservative therapy, and heavy recurrent bleeding, surgical treatment is indicated (Fig. 2). According to the Mayo Clinic, the most satisfactory results were obtained by alloying the nodes with a latex washer and hemorrhoidectomy.
Anal fissure ranks second among anorectal diseases and is a linear or triangular mucosal defect 1.0–1.5 cm long, located near the transitional fold, above the Hilton line. The origin of the fissure is associated with many reasons, but the most important factor is trauma to the mucous membrane of the anal canal by feces, foreign bodies, and damage to it during childbirth. A predisposing factor may be hemorrhoids.
A sharp crack has a slit-like shape, smooth, even edges. Its bottom is made up of sphincter muscle tissue. With a long course of the pathological process, connective tissue grows along the edges of the crack. Its bottom is covered with granulations. In the area of the outer edge of the crack, excess tissue forms the anal (sentinel) tubercle. Thus, an acute fissure turns into a chronic one, which is an ulcer with scarred edges and a scarred bottom (Fig. 3).
Sometimes an acute crack heals on its own, but more often it becomes chronic. As a rule, there is only one crack and most often it is located on the back wall of the anal canal. Occasionally you can observe two cracks that are located one above the other. It is necessary to distinguish true cracks from various superficial damage to the perianal skin. The most common localization of cracks (at 12 o'clock on the posterior wall and at 6 o'clock on the anterior wall) is explained by the structural features of the anal sphincter. It is at 6 and 12 o'clock that the blood supply conditions are worse, and there is a great danger of injury to the mucous membrane during the passage of feces during defecation due to pressure on the posterior and anterior commissures. Trauma to the mucous membrane leads to acute pain due to irritation of numerous nerve endings and sphincter spasm. A vicious circle is formed - an anal fissure leads to a sharp pain syndrome, pain syndrome leads to sphincter spasm, sphincter spasm prevents the healing of the fissure.
A triad of symptoms characteristic of the clinical picture of an anal fissure is pain during and especially after defecation, sphincter spasm and scanty blood discharge. There are differences in the clinical picture of acute and chronic fissures. With an acute fissure, the clinical manifestations are pronounced. The main symptom is acute pain after defecation, lasting several hours. Sphincter spasm increases pain. The pain becomes throbbing. Blood is detected as droplets on the surface of the stool. Due to sphincter spasm and a feeling of fear before defecation, stool is delayed. Taking laxatives increases pain.
With a chronic fissure, the pain is less acute, its duration after stool is 5–10 minutes. Sphincter spasm is mild. When a chronic anal fissure is complicated by marginal fistulas, purulent discharge, itching, and irritation of the perianal skin appear. A chronic crack is characterized by a cyclic course. It can heal, but at the slightest strain or physical stress it opens again.
Detecting an anal fissure is not difficult. Anamnesis and characteristic complaints suggest its existence. The diagnosis becomes clear already upon examination of the anus. When spreading the buttocks, a crack or guard tubercle is discovered at its outer edge. If the crack is not visible upon examination, then a digital examination of the rectum should be carefully performed. In this case, a compaction will be detected on the affected wall of the anal canal. Sigmoidoscopy in the acute period should not be performed due to severe pain and sphincter spasm. In cases where it is necessary to differentiate an anal fissure from other diseases, the study can be carried out after a preliminary injection of 4-5 ml of 1% novocaine solution under the fissure. Differential diagnosis is carried out with coccydynia and the anal form of Crohn's disease.
Conservative treatment of an acute fissure involves, first of all, eliminating pain, sphincter spasm and normalizing stool. To normalize stool, Mucofalk can be used, containing hydrophilic fibers from the outer shell of plantain seeds that retain water. As a result, the volume of stool increases and its consistency becomes softer. The drug is well tolerated by patients and does not increase pain in the abdomen and anus, which is characteristic of many laxatives. A diet limiting spicy and irritating foods is recommended. Once a day, cleansing enemas of boiled water at room temperature are given. In this case, the enema tip is thickly lubricated with petroleum jelly and inserted along the edge of the anus opposite to the one along which the crack is located.
After cleansing the intestines, take warm (38 °C) sitz baths with a weak solution of manganese for 10 minutes. Self-stool should be avoided during this period due to the risk of increased pain and spasm. Laxatives, as mentioned above, are contraindicated, as they can increase pain. Then soft-based suppositories (Relief, Relief Advance, Ultraproct, Posterisan) are inserted into the rectum. Treatment with suppositories is carried out until the crack is completely epithelized. Cleansing enemas, as a rule, are given during the first 10 days from the onset of the disease, after which the stool is independent.
When conservative therapy is ineffective, surgical treatment is resorted to, which consists of excision of the fissure and sphincterotomy. In recent years, closed lateral subcutaneous sphincterotomy has been proposed for the treatment of uncomplicated anal fissure [3, 7], after which pain disappears faster and there are fewer relapses.
Paraproctitis is inflammation of the tissue surrounding the rectum. Among proctological diseases, paraproctitis accounts for 15%. There are three fascial-cellular spaces: subcutaneous, ischiorectal and pelvic rectal. Accordingly, paraproctitis is divided into subcutaneous, submucosal, ischiorectal and pelvic-rectal. The disease is caused by various microorganisms that penetrate into the cellular spaces from the rectum through the anal glands, damaged mucous membrane, as well as hematogenously or lymphogenously from neighboring organs affected by the inflammatory process.
Of particular importance in the pathogenesis of paraproctitis is direct damage to the mucous membrane of the rectum in the area of the posterior wall of the anal canal, where wide and deep crypts are located, which are the entrance gates of infection. From 6 to 8 ducts of the anal glands open into each crypt. Through them, the infection spreads to the perirectal tissue spaces. According to the clinical course, paraproctitis is divided into acute and chronic. Acute paraproctitis is a purulent inflammation (abscess) of the peri-rectal tissue. Chronic paraproctitis is a consequence of acute inflammation. This is a pararectal fistula, formed after spontaneous opening of an abscess or opening it surgically. The internal opening of a pararectal fistula is a defect in the rectum. The external opening is located on the skin of the perineum (Fig. 4).
In some cases, several fistula tracts and several external openings of the fistula can be observed. The disease begins with a prodromal period (up to three days), during which weakness, headache, and general malaise may be observed. Then chills, fever, and pain in the perineal area appear. When the cellular spaces of the small pelvis are affected by the type of phlegmon, the clinical picture is dominated by general symptoms caused by intoxication. As the process is limited and an abscess is formed, the intensity of the pain increases. It takes on a pulsating character.
The greatest importance in the diagnosis of acute paraproctitis is examination of the anal area and digital examination of the rectum. Upon examination, attention is drawn to hyperemia of the skin in the perineal area on the affected side. Palpation of the perineum is painful, fluctuation can be detected. Digital examination is also painful in many cases and should be performed with caution. This technique should not be neglected, since the information obtained through digital examination can be very valuable for recognizing almost all forms of acute paraproctitis.
Treatment of acute paraproctitis, carried out immediately after diagnosis, is surgical. Basic principles of treatment: 1) opening the abscess; 2) elimination of the internal opening through which the abscess cavity communicates with the rectum.
Chronic paraproctitis, as mentioned above, is a consequence of acute paraproctitis. If, when opening the abscess, the internal opening in the rectum is not eliminated, a rectal fistula may subsequently form. A rectal fistula is characterized by the presence of one or more external openings in the skin of the perineum. Pus, feces and gases may be released from the external openings of the fistula tract. The general condition of patients with chronic paraproctitis suffers little. Pain appears only when the process worsens. Depending on the location of the fistula tract in relation to the sphincter muscle, four types of fistulas are distinguished: subcutaneous-submucosal (intrasphincteric), transsphincteric, complex (extrasphincteric) and incomplete. The latter have only an internal opening in the rectum and do not have an external opening in the perineum. The source of their formation is often an anal fissure.
In the diagnosis of chronic paraproctitis, the same methods are used as for acute paraproctitis. Digital examination of the rectum makes it possible to judge the tone of the sphincter and, in some cases, detect the internal opening of the fistula. Be sure to perform probing with a button probe, which is inserted into the fistula tract through its external opening (Fig. 5).
Using a probe, the direction of the fistula tract and its relationship to the sphincter muscle are determined. Fistulography is a mandatory x-ray examination of rectal fistulas. A test with a dye is used to determine the patency of the fistula tract, the location of the internal opening and purulent cavities in the tissue. Sigmoidoscopy is performed to detect concomitant diseases and high-lying internal fistula openings.
Treatment of all types of fistulas is surgical. The operation can be considered radical only if the opening in the rectum is eliminated by excision of the fistula tract.
Proctitis is an acute or chronic inflammation of the mucous membrane of the rectum or rectum and sigmoid colon (proctosigmoiditis). Acute proctitis most often has a specific cause. It can be caused by trauma, foreign bodies, mechanical irritation during prostate massage, chemical and thermal burns, and frequent cleansing enemas. The disease may be a consequence of radiation therapy for malignant tumors of the pelvic organs (radiation proctitis) or infections (gonorrheal, dysenteric proctitis). The development of proctitis can be facilitated by diseases of neighboring organs (hemorrhoids, anal fissure, paraproctitis, Douglas pouch abscess, prostatitis, cystitis, vulvovaginitis, etc.). Long-term proctitis and proctosigmoiditis that cannot be treated conservatively should, first of all, be differentiated from distal forms of ulcerative colitis [2].
Acute proctitis has a sudden onset, may be accompanied by fever, chills, is characterized by inflammatory changes in the rectal mucosa, clinically manifested by a frequent urge to defecate, tenesmus due to constipation, a burning sensation and a sensation of a “foreign body” in the anus. Examination of the rectum with a finger and sigmoidoscopy are poorly tolerated by patients due to severe pain. The rectal mucosa is sharply hyperemic, swollen, and bulges into the lumen. The vascular pattern is blurred or absent.
Chronic proctitis, as a rule, is a consequence of an untreated acute disease or has a specific nature. Clinically, the disease is manifested by a periodic feeling of discomfort in the rectum, a feeling of incomplete emptying, periodic exacerbations, accompanied by frequent stools mixed with mucus (sometimes blood), and tenesmus. Endoscopy reveals hyperemia of varying severity and swelling. The diagnosis requires the exclusion of infectious, parasitic and other diseases.
Treatment of acute proctitis is conservative. First of all, you need a diet that excludes all irritating foods and alcohol. After complete cleansing of the intestines, 100.0 ml of warm chamomile infusion (temperature 37–38 °C) is injected into the intestine for therapeutic purposes. An oil enema is given at night (50–75 ml of warm -37–38 °C vegetable oil). Starting from the second week of the disease, morning medicinal chamomile enemas are replaced with enemas of 0.3–0.5% collargol solution. The concentration of the solution is determined by the intensity of the inflammatory process in the intestine. Oil evening microenemas are continued for 14 days. The general course of treatment is 2–3 weeks. After a 10-day break, the course of treatment should be repeated to avoid relapse.
When treating chronic proctitis, the same remedies are recommended as for acute proctitis, but the course of conservative therapy is longer. The best effect is achieved by therapeutic microenemas from a collargol solution.
Anal itching is a pathological condition characterized by persistent scratching in the anus. It is necessary to clearly distinguish idiopathic (primary) anal itching and secondary, often accompanying diseases such as hemorrhoids, anal fissure, helminthic infestations, proctitis and proctosigmoiditis. While the causes of secondary anal itching are known, the etiology of primary (idiopathic) itching is not fully understood.
Often itching in the anus is the patient's main and only complaint. According to the clinical course, acute and chronic anal itching are distinguished. The acute form is characterized by a sudden onset, a constant course, significant intensity and local changes in the skin such as wet eczema with maceration, traces of scratching, hypertrophy of the perianal folds. With chronic itching, on the contrary, the onset is slow, the skin is often dry, thinned, sometimes depigmented, there are no traces of scratching at all or they look like thin linear abrasions.
Diagnosis of the causes of anal itching always begins with determining the type of itching (idiopathic or secondary). First of all, it should be determined whether itching is a symptom of the above diseases (secondary), whether its occurrence is associated with the intake of spicy or salty foods, alcohol, contact with harmful chemicals and radioactive substances, the presence of allergies, etc. From laboratory tests, a blood test is performed for sugar content and three-time stool analysis for worm eggs. In men, urethritis and prostatitis should be excluded; in women, vaginal itching should be excluded.
Treatment of secondary anal itching consists of treating the underlying disease. For idiopathic anal itching, treatment is purely symptomatic.
A diet excluding spicy foods and alcohol is recommended. Thorough toileting of the anus after each act of defecation. After this, ointments (Posterizan, Proctosedyl, Aurobin, Emalan) are injected into the rectum. At night, warm sitz baths with a solution of manganese and microenemas from a 0.33% solution of collargol -50.0 ml are prescribed. The course of treatment is 10 days. For the next 10 days, microenemas (50 ml) of warm vegetable oil are prescribed.
Methods of conservative treatment of anal pathology are being improved as new drugs are developed. From this point of view, one should pay attention to medical collagens, which have become used in the complex therapy of many diseases.
The problem of studying collagen as a new plastic material has long attracted the attention of researchers. At the origins of the development of this direction was Academician of the USSR Academy of Medical Sciences V.V. Kovanov. As a result, a new class of medicinal dosage forms was created - plastic materials with targeted action based on the natural biopolymer of collagen. Currently, medical collagen Emalan, which is a collagen hydrogel for problematic skin and wounds, has become widely used in practical healthcare. It successfully passed clinical trials at the Burn Center of the Research Institute of Emergency Medicine named after. N.V. Sklifosovsky (1995), at the Military Hospital named after. N. N. Burdenko (1999) and in the 72nd Central Clinic of the Ministry of Emergency Situations (2009). It has been established that Emalan reduces signs of inflammation. Under its influence, hyperemia, swelling, pain disappear, itching and peeling of the skin decreases or disappears. All of the above served as the basis for the use of this drug in the treatment of anal pathology.
Of the 112 we observed during 2009–2010. 54 patients had acute and chronic anal fissures, 50 had grade I and II hemorrhoids, and 8 had idiopathic anal itching.
When treating anal fissures, Emalan was included in complex therapy. It was introduced into the rectum on a suppository and in the form of applications to the anus for 3 weeks. In 70.3% of cases, positive dynamics were noted already on days 4–5 from the start of treatment. By the end of the third week, 31 patients had complete healing of the fissures. In patients suffering from hemorrhoids complicated by anal fissure and itching (50), by the end of the third week, against the background of complex therapy, a decrease in symptoms of the disease, such as itching, pain, burning, was observed. The drug turned out to be especially effective in the treatment of patients with idiopathic (8) and secondary (6) anal itching. While taking the drug (gel applications to the anal area 3-4 times a day), a decrease in scratching, maceration and skin hyperemia was noted. By the end of the two-week course, these changes completely disappeared.
Our first experience has shown that the domestic collagen gel Emalan can be successfully used in the complex treatment of acute and chronic anal fissures, proctitis, anal itching and complicated forms of hemorrhoids. The drug makes it possible to increase the effectiveness of therapy and helps reduce treatment time.
Literature
- Vorobyov G.I., Shelygin Yu.A., Blagodarny L.A. Hemorrhoids. M. // "Mitra-Press". 2002. 192 p.
- Grigorieva G. A. Anorectal pathology. Guide to gastroenterology // M.: Medicine. 1996. T3. 606–635 pp.
- Henry M. M., Swash M. Coloproctology and the pelvic floor // M.: Medicine. 1988 (translation from English). 451 p.
- Rivkin V.L., Kapuller L.L. Hemorrhoids // M.: Medicine. 1984. 751 p.
- Rivkin V.L., Dultsev Yu.V., Kapuller L.L. Hemorrhoids and other diseases of the anal canal // M.: Medicine. 1994. 239 p.
- Rivkin V. L., Kapuller L. L. Hemorrhoids. Constipation // M.: Medpraktika. 2000. 158 p.
- Fedorov V.D., Dultsev Yu.V. Proctology. M.: Medicine. 1984. 380 p.
- Haas PF, Fox TA, Haas GP The pathogenesis of haemorrhoids. Disease of the colon and rectum. 1984. T. 27. p. 442–450.
- Thomson WHF The nature of haemorrhoids // British J. of Surgery. 1975. T. 62. p. 542–552.
- Thomson WHF The nature and cause of haemorrhoids. Proceedings of the Royal Society of Medicine. 1975. T. 68. p. 574–575.
G. A. Grigorieva , Doctor of Medical Sciences, Professor S. V. Golysheva First Moscow State Medical University named after. I. M. Sechenova , Moscow
Contact information for authors for correspondence
Anal itching in children
Children quite often suffer from itching and burning in the anus, but it is worth noting that the most common cause of this is helminthic infestation.
Diagnosis of the presence of pinworms in a child’s body is usually based on itching in the anus, which often appears at night. In some cases, with this disease, pinworms themselves can be found in the child’s stool, which look like thin little white worms. But still, if your child experiences anal itching, you should consult a doctor.
Getting rid of itching of the anus in a child of this kind is quite simple. You should only take the medications prescribed by your doctor. It is worth noting that if pinworms are detected in children, it is recommended that all family members undergo a course of treatment, due to the fact that this disease is quite easily transmitted through household means.
How is radiation proctitis diagnosed?
Diagnosing diseases is not difficult. The key point here is the presence of a history of radiation therapy and its effect on the pelvic organs, increased frequency of stool, and the presence of pathological impurities in it.
If the course is prolonged, it is recommended to examine the rectum using a rectoscope or endoscope. This will allow you to detect multiple erosions, scar deformation, atrophic changes and telangiectasias and decide on the need for endoscopic or surgical treatment.
Prevention of anal itching
You can reduce the likelihood of anal itching by following some basic rules that will help not only avoid the occurrence of such a disease, but also increase the overall vitality of a person.
Following a proper balanced and nutritious diet will not only benefit you in terms of preventing anal itching, but also in terms of benefits for your entire digestive tract. It is necessary to avoid excessive consumption of sweet carbonated drinks, coffee, tea, milk, alcoholic beverages, tomatoes, seasonings, hot peppers, citrus fruits and chocolate.
Another important point is maintaining perineal hygiene, but at the same time it should be remembered that excessive hygiene, like the use of alkaline soap or perfumed products, can lead to irritation in this area. Therefore, if you notice that any soap or gel causes a burning sensation in your anus, then you should think about choosing another product to which you will not have a similar reaction.
Despite fashion trends, you should always give preference to comfortable underwear made from natural fabrics. The use of tight-fitting clothing leads to increased sweating of the body in general, and in the anus in particular, which is also one of the causes of anal itching.
Manifestation of the disease
Symptoms of UC can be divided into typical, which are usually present at the onset of the disease, and extraintestinal.
The first include:
- diarrhea (increased frequency of bowel movements more than 3 times a day),
- the presence of blood in the stool, nighttime bowel movements (more often with pronounced activity of the process),
- tenesmus (false urge to defecate that does not end with bowel movement),
- weight loss,
- fever,
- anemia (a decrease in hemoglobin can be manifested by pale skin, rapid heartbeat, and weakness).
Extraintestinal manifestations include:
- diseases of skin joints, sclera of the iris,
- autoimmune liver damage,
- osteoporosis,
- psoriasis,
- formation of stones in the biliary system,
- fatty liver degeneration,
- thrombosis of peripheral veins.
However, extraintestinal manifestations are not strictly specific for UC, and their presence requires a careful assessment by specialists of the cause of occurrence.
Symptoms of ulcerative colitis can vary in severity. It depends on the stage of the disease, the nature of the disease (acute or chronic), severity and presence of complications. It should be remembered that, like any chronic disease, UC can occur with remissions and exacerbations, which also affects the clinical picture.