Take the first step
make an appointment with a doctor!
For a long time, this disease was not recognized as an independent disease and was considered as a type of endometriosis. There is still debate in the scientific community about the nature, causes and mechanisms of development of uterine adenomyosis. However, it poses a serious threat to women's health. in particular, their ability to conceive and bear a healthy child. In severe cases, it leads to complete and irreversible loss of reproductive function.
Definition of disease
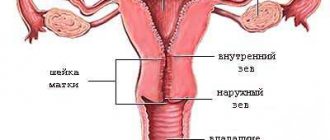
In a healthy uterus, the wall is strictly demarcated into layers, there are three in total:
- The muscle layer - the myometrium is sensitive to hormonal effects, especially to prostaglandins and oxytocin. It consists of three layers: the middle circular or vascular (the thickest), the internal longitudinal or submucosal (the thinnest), and the subserosal (outer).
- Serous - in addition to the uterus, the perimeter covers the abdominal cavity, bladder, and rectum.
- The endometrium is the membrane that covers the inside of the uterus. It is she who plays the main role in the development of adenomyosis.
The endometrium consists of two layers:
- deep basal, performing a regenerating function after menstruation
- functional, rejected during menstruation.
If it is not completely excreted with menstrual blood, and its fragments remain in the uterus, growing into its thickness, then adenomyosis occurs. The remaining tissue continues to function as usual, thickening of the uterine wall and other changes appear, and the cycle is disrupted.
What is adenomyosis?
When is surgery needed?
There are two surgical treatment options for focal adenomyosis: organ-preserving and organ-sapping.
The organ-preserving option is used in the case of the presence of one large focus of endometriosis - nodular adenomyosis; surgical treatment is similar to the removal of a fibroid node, but is technically more complex. Endometriotic infiltration can spread to an insignificant or significant part of the muscle layer, but it can be very difficult to distinguish healthy tissue from altered tissue due to the absence of a clear demarcation line or capsule, like a myomatous node. The situation is also complicated by the presence of an inflammatory process and rigidity of the uterine walls when comparing the wound surface during suturing of the surgical wound. Therefore, the operation requires a great deal of experience from the surgeon.
The goal of organ-removing surgical treatment for focal adenomyosis is the radical removal of endometrioid lesions, which allows restoring normal functioning of the body. Indications for radical surgery are:
- ineffectiveness of conservative treatment;
- multiple foci of changes;
- mixed form of adenomyosis;
- combination of adenomyosis with other diseases of the reproductive organs: fibroids, ovarian tumors, endometrial diseases, etc. in older patients who do not have reproductive plans.
Most domestic surgeons, in accordance with the recommendations of the Association of Obstetricians and Gynecologists, perform hysterectomy or supravaginal amputation of the uterus.
Classification
Adenomyosis of the uterus is classified according to its forms:
- focal - lesions are localized in the submucosa. It does not respond well to conservative treatment due to its relapsing course. Older women and women before menopause are more likely to get sick;
- nodular - multiple nodes of adenomyosis are formed according to the myomatous type from the connective tissue and glandular epithelium. Typical for young girls;
- diffuse - with adenomyosis, all layers of the uterus are affected. Penetration of pathological particles to varying depths leads to the formation of “pockets”;
- diffuse-nodular (mixed) - a combination of two types.
By stages:
- I - the mucous membrane of the uterine body is affected, the symptoms are mild;
- II - less than half the muscles are affected. Unexpressed signs: mild pain, minor non-cyclical discharge, more abundant discharge;
- III - the muscles of the uterus are affected by adenomyosis by more than 50%. The manifestations are intensifying.
- IV - involvement of the myometrium throughout its depth. Possible spread to nearby areas. The symptoms are pronounced.
If adenomyosis is not treated in stage I or II, then in phase III or IV the disease will be complicated by severe conditions.
Types of pathology
Expert recommendations
It has been proven that being overweight significantly increases the risk of developing adenomyosis. The reason is that in obese women the balance of hormones is shifted. The processes of metabolism and cellular regeneration are disrupted. The endometrium grows and affects muscle tissue. The greatest danger is obesity during menopause: excess weight complicates already complex natural processes.
Therefore, we recommend that our patients love themselves, take care of their bodies, watch their weight and eat right. From a young age, pay attention to your own health, and then adenomyosis during menopause will not be scary for you.
Causes
The etiopathogenesis of adenomyosis has not yet been sufficiently studied. The manifestation is associated with hyperestrogenism (increased production of estrogen). Progesterone causes stable remission, so the disease most likely will not progress during pregnancy.
The development of adenomyosis is influenced by the following provoking factors:
- Hormonal disbalance.
- History of IUD. This is indicated by 45% of patients with adenomyosis.
- Incorrectly selected COC.
- Heredity.
- Early or late menarche.
- Surgical interventions on the uterus and other reproductive organs. Frequent abortions and spontaneous miscarriages are especially dangerous. 70% of patients with adenomyosis have a history of adenomyosis.
- Childbirth natural or caesarean section.
- Invasive diagnosis of uterine pathologies.
- Frequent infections of the genitourinary system, including STDs.
- Rare sex or its complete absence, traumatic sexual intercourse, use of crude barrier contraceptives.
- Obesity. It is observed in 60% of patients with adenomyosis.
- Chronic stress, weakening the immune system, constant nervous tension.
- Alcohol abuse, smoking.
- Endocrine pathologies.
- Hard physical labor.
These factors will not necessarily lead to adenomyosis, but their presence, especially in combination, significantly increases the risk of developing the disease.
Scientists adhere to different theories about the likelihood of adenomyosis:
- intrauterine or congenital - it is believed that the predisposition appears in utero, when the rudiments of the uterus are formed;
- stem cells - a relatively “young” theory that involves the penetration of bone marrow cells into the muscle;
- invasive growth - when the uterus is dissected during surgical treatment, endometrioid cells directly invade the myometrium, adenomyosis develops in the scar area;
- postpartum inflammation - some scientists see a direct connection between childbirth and adenomyosis. The postpartum inflammatory process leads to disruption of the boundaries between the layers of the uterus. This can also occur after any genital surgery.
The disease can develop due to abnormalities in the structure of the uterus. For example, when the channel is insufficiently opened, which leads to an increase in pressure in the organ.
Forecast
Adenomyosis is a chronic disease prone to relapsing. The return of the disease is diagnosed in approximately every fifth fertile patient after conservative therapy or organ-saving surgery. In this regard, gynecologists can prescribe hormonal contraceptives for prevention.
In premenopausal patients, the disease is milder and during menopause it completely disappears.
Book a consultation 24 hours a day
+7+7+78
Symptoms
For adenomyosis
the structure of the uterine muscles changes. The growth of the endometrium during menstruation causes thickening of the muscle, the appearance of foci of inflammation and nodules. This prevents the evacuation of the functional plate with blood discharge during regulation, which leads to disruption of menstrual function. The clinical picture of adenomyosis is variable.
Most common symptoms:
- dysmenorrhea (severe pain during menstruation);
- brown spotting after coitus and between cycles;
- menorrhagia with blood clots;
- dyspepsia;
- anemia due to blood loss;
- weakness;
- pain in the lower abdomen, not related to regulation, of a pulling or spasmodic nature.
Sources
- Clinical guidelines – Endometriosis – 2021 – Approved by the Ministry of Health of the Russian Federation.
- Unanyan A.L., Sidorova I.S., Kogan E.A. Active and inactive adenomyosis: clinical and morphological development options, differentiated approach to therapy. Scientific article – Journal of Obstetrics, Gynecology and Reproduction, 2012.
- Linde V.A., Reznik M.V., Tarasenkova V.A. Sadikhova E.E. Modern ideas about adenomyosis. Scientific article – Bulletin of the Ivanovo Medical Academy, 2021
Share:
Doctor's opinion
Adenomyosis is rarely diagnosed at an early stage.
Usually discovered when complications occur. Precursors of the disease are heavy menstrual bleeding, pain, which patients accept as normal and do not consult a doctor. In half of the cases, adenomyosis is accompanied by endometrial hyperplasia and uterine fibroids. A prognostically important sign is a gradual deterioration of the condition. That is, the pain of menstruation increases over time. Initially, pain occurs after the onset of menstruation. Then she worries in the intervals between cycles. If these symptoms appear, even with a regular menstrual cycle, you should consult a gynecologist. — Pesegova Evgenia Vladimirovna Reproductologist, obstetrician-gynecologist
In advanced cases of adenomyosis, bloating and flatulence may occur. Often it is with these symptoms that people turn to a therapist. At this stage, treatment will already be difficult. With adenomyosis, the quality of sexual life deteriorates due to painful sensations. A woman may even gradually refuse intimacy. It is necessary not to delay time, but simply to find out the cause of these pains and begin treatment of adenomyosis.
Intoxication (vomiting, loss of appetite, diarrhea or constipation) may be mistaken by the patient for a pathology of the digestive system. Only a qualified gynecologist can connect this with adenomyosis. Young girls usually have no symptoms. But as the pathological process progresses, the main symptom in most cases becomes discomfort or pain in the lower abdomen. There is irradiation to the perineum, anus, lower back, increased during sex, menstruation, and physical activity. The woman associates such manifestations with cycle problems and turns to a gynecologist for examination and treatment.
Signs of the disease
Postoperative period
Features of the postoperative period depend on the volume of intervention and the method of its implementation. The easiest way for patients to tolerate laparoscopic or hysteroscopic organ-preserving operations. The pain syndrome in the postoperative period is moderate, activation is possible already on the first day if there are no contraindications from the anesthesiologist.
In the first few weeks, bloody discharge from the genital tract is characteristic, which gradually decreases. During this time, it is recommended to avoid excessive physical activity and sexual activity.
In general, most patients feel satisfactory after surgery and even note an improvement in their quality of life, as pain during menstruation decreases, PMS is easier and the amount of bleeding decreases.
Diagnosis of adenomyosis
To make a diagnosis, complaints are first listened to and an anamnesis is collected. A gynecological examination shows globular enlargement of the uterus, when it takes on a spherical shape. This indicates adenomyosis. If a woman does not complain about anything, then damage to the muscles of the uterus can be detected during a medical examination. And also when visiting a gynecologist about other reproductive diseases.
During a bimanual examination, not only the shape and size of the uterus is determined, but the condition of the appendages and the absence of anatomical defects are also assessed. Palpation may reveal nodules characteristic of nodular adenomyosis of the uterus
. The nodes are densely structured and filled with brownish liquid. The color is due to the mixing of blood and glandular secretions.
Diagnosis for adenomyosis includes:
- general blood and urine tests;
- biochemistry:
- smears from the vagina for microflora, from the cervical canal for oncocytology to identify precancerous conditions;
- transvaginal ultrasound sonography. The enlargement of the uterine body is visualized, structural changes in the myometrium are determined;
- ultrasonography of the pelvic organs;
- hysteroscopy is a therapeutic and diagnostic procedure that allows you to examine the uterine cavity and perform minimally invasive interventions. For example, remove nodes with adenomyosis, foci of endometriosis, polyps or cysts;
- colposcopy - examination of the uterus using a magnifying device with a lighting element - a colposcope. The device magnifies the image 40 times, so the diagnostician will not miss the slightest detail, for example, cervical adenomyosis. If necessary, to differentiate from erosion, an extended colposcopy of the cervix is performed - the suspicious area is treated with Lugol's solution or acetic acid. Unhealthy tissue will remain red, healthy tissue will turn white;
- MRI - done if there is a suspicion of cancer, the spread of adenomyosis to the outside or other organs. In this case, it will be a different diagnosis - external endometriosis.
During hysteroscopy, colposcopy or diagnostic laparoscopy, a biopsy sample is taken for morphological examination for the presence of atypical cells. When examining biomaterial, it is not always possible to detect pathology, since it is difficult to select the correct area for biopsy. A comprehensive examination allows an experienced doctor to determine changes in the layers of the uterus, the degree of damage and develop an effective treatment program for adenomyosis.
Diagnostic methods
Laparoscopic surgery is a minimally invasive technique with many advantages
To perform surgery for focal adenomyosis, I use laparoscopic access, in which all manipulations are performed through several small punctures on the anterior abdominal wall. Due to the minimally invasive nature of laparoscopic intervention:
- there is no pain after surgery;
- early activation of the patient is possible: already on the first day the patient gets out of bed;
- hospitalization lasts no more than three days;
- rehabilitation takes about two weeks.
All manipulations are carried out using the latest endoscopic equipment equipped with a video camera - the possibility of good visualization virtually eliminates the risk of developing intraoperative complications.
When performing laparoscopic surgery, my patients also have the opportunity to get rid of other diseases that require surgical treatment (fibroids, cholelithiasis, cysts, etc.) during one anesthesia. We are talking about simultaneous operations, which I was one of the first to carry out in our country.
If you are concerned about pain, discharge, menstrual irregularities and other symptoms of adenomyosis, seek medical help without delay. Remember, with focal adenomyosis of 1-2 degrees, treatment can be conservative. Treatment options for severe adenomyosis with complications are not so wide. But in any case, I strive to carry out low-traumatic treatment, choosing a technique that will be optimal in a particular case.
For many years I have been developing and performing breast-conserving laparoscopic surgeries. I have performed about 24,000 interventions on the abdominal and pelvic organs, more than 600 of which were for adenomyosis. The results of the operations are summarized in the monographs “Simultaneous laparoscopic surgical interventions in surgery and gynecology”, “Laparoscopic operations in gynecology”, as well as in numerous scientific peer-reviewed publications published in Russia and abroad.
My narrow specializations are, in addition to surgery, gynecology, urology, proctology and oncology. Operations involving damage to organs of several systems at once require high qualifications. Therefore, even with widespread endometriosis, when there is damage to other organs, you can count on my knowledge and experience.
Therapy for adenomyosis
The gynecologist takes into account the form of the disease, its stage, the patient’s age, plans for pregnancy, and concomitant pathologies when choosing a treatment regimen for adenomyosis. Conservative treatment consists of the use of anti-inflammatory drugs and antibiotics (for infections), hormonal drugs for cycle disorders, symptomatic ones, and vitamins. For local treatment, tablets or suppositories with an antibacterial effect are effective.
With diffuse lesions, the result of drug treatment is insignificant, so surgery is advisable if there are no contraindications. The most effective way to eliminate uterine adenomyosis is by a combined method, combining an invasive procedure and medications.
Surgical minimally invasive ways to combat adenomyosis:
- Hysteroscopy - performed under anesthesia. After antiseptic treatment, a speculum and dilators are inserted into the vagina, then a hysteroscope is inserted into the uterine cavity. The doctor works with manipulators, watching his actions on the monitor in an enlarged form. Limitations: acute inflammation, decompensated liver failure, endocervical stenosis, cervical cancer, menorrhagia.
- Laparoscopy is the preferred technique for nodular adenomyosis, allowing the patient to completely rid the patient of endometrioid nodes.
- Uterine artery embolization (UAE) - the uterine vessels supplying the pathological area are blocked with an embolic substance. The treatment option for adenomyosis is suitable for patients planning to give birth in the future. UAE lasts an hour and a half under local anesthesia.
Immediately after the procedure there are no significant changes in well-being. The stomach may hurt and there may be minor bleeding for 3-4 days. The rehabilitation period after gentle surgical treatment lasts up to two weeks. In order to prevent a relapse of adenomyosis, it is recommended to abstain from sex, physical activity, visiting saunas, and taking hot baths during this time. Normalization of menstrual function occurs after a month and a half. You must come for control diagnostics as scheduled.
With progressive adenomyosis, the uterus is removed if other treatment methods have not given the expected result. Hysterectomy is rarely resorted to if there are concomitant gynecological problems (large fibroids, polyps, cysts). Or with advanced adenomyosis with a significant area of damage and complications. And also in older patients, if there is no need to preserve the uterus. After a hysterectomy, recovery is long and difficult; a woman will not be able to get pregnant or give birth. Patients of childbearing age experience psycho-emotional disorders, their menstruation stops, their libido decreases, and they experience discomfort during coitus. There may be vaginal prolapse.
Treatment methods for uterine adenomyosis
How the operation is performed - my approach to treatment
When choosing treatment tactics, I adhere to an unshakable rule: only an individual approach to each patient. Therefore, I select the treatment method, taking into account a number of factors: the degree of the disease, the presence of certain symptoms, age, desire to preserve the uterus, etc. If this is possible according to indications, I always strive to perform organ-preserving surgery.
To ensure that surgical intervention is as effective as possible and at the same time safe, I use a whole range of proprietary techniques. Among the main ones it is worth highlighting several points, for example,
- Since during surgery on the uterus there is always a risk of bleeding due to the peculiarities of the blood supply to the organ, to eliminate blood loss I use a technique I have developed, for which a patent has been filed - temporary occlusion of the arteries supplying the uterus. When the blood supply is temporarily suspended, there is no risk of bleeding; all manipulations are performed with a completely dry surgical field. This approach also makes it possible to perfectly match the edges of the wound, which subsequently affects the quality of the suture. The duration of the operation is significantly reduced.
- Moreover, to accurately match the edges of the wound when suturing the uterine walls, I use through U-shaped sutures, and special clamps are used to temporarily fix the uterine wall, which also contributes to a better result. In particularly difficult cases, I use the V-loc suture system (Covidien, Switzerland). The thread, made of monofilament absorbable polydioxanone material, with notches oriented at a certain angle, slides freely in one direction and does not move in the opposite direction, which ensures ideal alignment of the wound edges. As a result, the seam is formed 3-4 times faster. In addition, there is no need to tie knots, which reduces operation time.
- During the operation, I use modern instruments - Thunderbeat (a combination of ultrasound and bipolar energy) and LigaSure (electrosurgical ligation system of dosed impact), which also increases the safety of the intervention, eliminating the risk of intraoperative bleeding. There is no need to use surgical threads and clips.
- At the first stage of the operation, I perform an inspection of the abdominal cavity and pelvic organs. If there are foci of endometriosis on adjacent structures, which often accompanies adenomyosis, I perform radical excision of these foci, otherwise there is a risk of recurrence or complications. For example, if there are foci of endometriosis on the ureters, small intestine, or fallopian tubes, for gentle removal, I use an original developed technique - shaving, in which the foci are shaved off without unnecessary tissue trauma. Foci located on the peritoneum and ovaries are also subject to removal; existing adhesions are dissected.
If organ-preserving surgery is not possible, then I remove the uterus while preserving the ovaries, which avoids the early onset of menopause and preserves natural hormonal levels. Patients should know that removal of the uterus cannot cause the disappearance of sexual desire or the inability to obtain sexual satisfaction, since the uterus does not produce sex hormones, but is only a target for them. The result of removing the uterus will be only the absence of menstruation and the inability to bear a fetus. Also, in most cases, I perform an operation with preservation of the cervix (in the absence of its diseases - endometriosis, multiple cysts, dysplasia, etc.), which allows preserving the anatomy of the pelvic floor (sexual life does not change, since there are no changes on the vaginal side).
You can ask questions and sign up for a consultation by phone: +7 (495)222-10-87
or fill out the form below
Thank you, your question has been sent successfully, we will contact you soon!
Ask a new question
Complications
The consequences of uterine adenomyosis can be severe. The most serious is infertility, which occurs due to hormonal imbalance. To conceive and bear a child, a healthy endometrium is necessary, which is not the case with adenomyosis. The embryo simply will not be able to implant normally into the uterine cavity. If adenomyosis is treated correctly and in time, pregnancy will occur.
Other complications of the disease:
- scarring of tissue, formation of adhesions, which will interfere with natural conception;
- disruption of the menstrual cycle caused by structural changes in the uterine muscles during adenomyosis, due to which it cannot normally perform its contractile function;
- malignancy;
- development of external genital (beyond the uterus) or extragenital endometriosis (beyond the boundaries of the reproductive organs, not only into nearby tissues, but throughout almost the entire body);
- pelvic pain syndrome.
At an advanced stage of adenomyosis, intestinal obstruction, anemia, and decreased immunity may occur.
Types and degrees
There are 3 types of uterine endometriosis:
- focal (the pathological process affects only some areas of the uterine wall)
- nodular (foci of the disease grow locally, forming capsular nodes)
- diffuse (endometrioid heterotopias are formed throughout the mucous uterine layer, forming cavities in the myometrium)
Degrees of the disease:
- first (the lesions grow no deeper than the layer of muscle tissue of the uterus)
- second (foci grow up to half of the myometrium)
- third (the pathological process covers almost the entire muscle layer)
- fourth (the lesions affect neighboring organs and the peritoneum, and fistulas form in the uterus leading to the pelvis of the sick woman)