Removing the uterus (or hysterectomy) is a fairly common surgical procedure. Indications for it may be different: uterine fibroids, various neoplasms and tumors (including ovarian cystomas in postmenopause), endometriosis. This volume of surgery is proposed in the case when preservation of the diseased organ is no longer possible, since it is accompanied by a high risk of complications (bleeding, malignancy, progression of the process)
Such operations began to be carried out about a hundred years ago, so experience in this area of gynecology has been accumulated quite a lot. A large number of clinical studies have also been conducted, which allow us to draw certain conclusions regarding the consequences of the operation and the quality of life of the operated patients. The modern level of gynecology and medical equipment make it possible to perform a hysterectomy using laparoscopy (in the case where the size of the uterus makes it possible), which guarantees high precision during the operation and quick recovery after it.
However, almost every woman for whom doctors recommend hysterectomy is much more concerned about the consequences of the operation. Although, quite often, you need to worry more about the pathology that is an indication for surgery.
How will life change? Will it be necessary to change something radically, to adapt to the functioning of an organism deprived of such an important organ as the uterus? How will the operation affect your sex life, and how will you now need to build your relationship with your sexual partner? Will the surgery cause changes in appearance: excess weight, rapid aging of the skin, growth of dark hair on the face and body?
If we try to answer all these questions briefly, the answer will be: “No radical changes will occur - neither in lifestyle, nor in appearance.”
And if you want a more detailed explanation, then read on.
Why do such questions arise?
A stable stereotype operates in a woman’s mind:
No uterus - no menstruation - menopause occurs. Menopause = old age.
Women are confident that removal of the uterus will entail an artificially induced unnatural restructuring of the body, which will lead to premature aging, decreased libido, and the extinction of many functions. There will be problems with health and well-being, frequent mood swings, causeless fatigue - which, in turn, will affect relationships with others, especially with loved ones. Psychological problems will be layered on top of physiological problems, and it will become difficult to achieve mutual understanding and trust in the family. The result is sad - early old age, loneliness, a sharp decrease in the quality of life, a feeling of guilt and inferiority.
In fact, this stereotype is quite easy to destroy if you understand the anatomical structure of the female body and understand the purpose of the uterus, the mechanism of menstruation and menopause. We will try to help you do this!
Scheme of implementation
Extirpation is performed exclusively in a surgical hospital with all the necessary equipment and a full complement of medical personnel. To alleviate the plight of a patient who is indicated for hysterectomy without or with appendages, she is given adequate pain relief: general, endotracheal or intravenous type, regional, epidural or spinal model, combined.
The exact mechanism of implementation is determined depending on whether excision is required with the tubes or other parts of the reproductive system. The algorithm is influenced by the access route, be it the supravaginal system or any other. Common points for successful intervention, regardless of the type of operation, are:
- intersection and ligation of round ligaments;
- mobilization followed by removal of appendages when the diagnosis requires it;
- mobilization with bladder displacement;
- intersection of vascular bundles;
- dissection of the prevesical fascia;
- intersection of ligaments with ligation;
- opening of the vaginal vault;
- vaginal hemostasis;
- peritonization.
The last point provides for limitations of the operating area from the main abdominal cavity. The plan can vary, be supplemented, or change points depending on the modification of the manipulation.
The uterus and its functions (briefly about the main thing)
The uterus is an organ of the female body that performs certain functions (for more details, see the section “Normal anatomy of the pelvic organs”). It is intended for the development of the embryo and gestation of the fetus. During the process of childbirth, the uterus also takes a direct and very active part - it contracts, thereby facilitating the expulsion of the fetus.
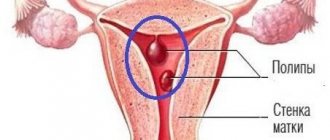
Inside, the uterus is, as it were, “lined” with a mucous membrane, the endometrium. The endometrium is saturated with blood vessels, and the blood supply increases noticeably towards the middle of the menstrual cycle and in the second phase (doctors say: “the endometrium thickens”). The body needs this so that the fertilized egg is safely fixed in the uterus and begins to develop. If fertilization does not occur, then the vessels do not receive nutrition, the upper layer of the endometrium separates and is rejected by the body. Menstruation begins.
When the uterus is removed, there cannot be menstruation, because there is no endometrium, the body simply has nothing to expel. However, this condition has a completely different nature than menopause. It's called "surgical menopause."
Types of operations and procedures
There are several ways to perform a hysterectomy, and which method is best for the patient depends on the reason for the procedure, previous surgeries, the presence of other diseases and the experience of the operating surgeon.
Abdominal hysterectomy
Removal of the uterus through an incision in the lower abdomen is performed under general anesthesia.
Before surgery, the bladder is emptied by inserting a catheter through the urethra. The catheter is removed after 2–3 days.
After disinfecting the surgical field, the doctor makes an incision in the lower abdomen and opens the abdominal wall. The uterus is completely removed after separation from neighboring organs (bladder, colon) and ligation of blood vessels.
It is sometimes necessary to remove the ovaries along with the uterus (hysterectomy with adnexectomy).
If necessary, a plastic drain is placed to allow secretions and blood to drain.
Vaginal hysterectomy
This is the removal of the uterus through the vaginal canal.
The procedure is more complex but less traumatic, so recovery and hospitalization are shorter compared to abdominal hysterectomy.
The operation is performed through the vaginal canal, without an incision in the abdomen. The uterine ligaments are separated and the organ is pulled out through the vagina.
Laparoscopic hysterectomy
Laparoscopic surgery is a procedure in which special laparoscopic instruments and cameras are inserted through small surgical incisions in the abdomen so that the inside of the human body can be seen on a screen.
Combinations of laparoscopic surgery with vaginal insertion are possible.
Laparoscopy has recently become a common method for a number of operations because it is less traumatic. After it, recovery occurs faster.
All operations usually last no more than two hours.
What is menopause
Menopause is the decline of ovarian function. They produce less and less sex hormones (estrogen, testosterone, progesterone), and the egg does not mature in them.
Estrogens (female sex hormones) are very important for the condition of bone tissue and blood vessels, so their absence very often leads to problems with the musculoskeletal system and blood circulation.
Decreased production of testosterone (male sex hormone) leads to a lack of sexual desire (libido). Active hormonal changes occur in the body - it is this that can lead to external changes such as excess weight, aging skin, and hair loss. Removal of the uterus cannot cause hormonal changes because the ovaries will continue to function and produce sex hormones.
Clinical studies prove that when the uterus is removed, the ovaries work in the same mode and during the same period, which is planned, “programmed” by the body genetically.
Estrogens are produced regardless of whether the uterus is removed or left, they continue to have a positive effect on bone tissue and the cardiovascular system. Testosterone is also produced, so libido does not decrease and the quality of sexual life does not change in any way.
Moreover, if you are familiar with such a condition as premenstrual syndrome (PMS), then it will persist. Because PMS is caused by the cyclical work of the ovaries.
Precautionary measures
Regardless of whether the formation of a stump or complete excision is planned, the preparation algorithm remains identical. First, the patient needs to find an experienced surgeon who will agree to perform the manipulation. It is best to base your choice on the reviews of women who have already experienced such a difficult period in life. You can find their responses on thematic websites or you will need to visit a specialized medical city forum.
Many people are concerned about the price, but all clinics adhere to their own strategy for setting costs, taking into account the qualifications of the medical staff, the instruments used, and medications. Before making a final decision in favor of a radical measure, a woman needs to sign up for a routine gynecological examination. During the appointment, the doctor will write out directions for a number of tests, the standard package of which includes:
- clinical examination of blood, urine;
- analysis for blood group and Rh factor;
- a smear from the vagina and cervix, which characterizes microscopy, PCR and oncocytology;
- colposcopy;
- ultrasound examination of the pelvic organs;
- X-ray of the lungs;
- electrocardiogram.
A mandatory point of the plan is blood biochemistry, which allows you to determine the level of hormonal content of the body, as well as identify markers of the inflammatory process. Along the way, testing detects antibodies to infections.
Those representatives of the fairer sex who have not passed a coagulogram, liver and kidney tests, and a test for electrolytes will not be allowed to undergo surgery.
Sometimes the victim’s condition is very advanced, which requires auxiliary consultation with related specialists of a narrow profile. This could be a cardiologist, who should help find out whether the body can cope with the load of general anesthesia, or a pulmonologist with a vascular surgeon. The risk group includes victims with a high probability of developing thrombosis.
They will have to sign up for a Doppler ultrasound so that the doctor can evaluate the condition of the veins of the lower extremities. Additionally, antispasmodics and other medicinal pharmacological products may be prescribed. When, during preparation, it turns out that the body is infected with an infectious disease, you will first have to get rid of the source of the disease with the help of antimicrobial drugs.
Only such a thorough approach will guarantee final success, and the consequences of what is done will not hit women’s health too hard.
Approach to surgery
If the doctor believes that it is necessary to remove the uterus, this does not mean that the uterine appendages (ovaries and fallopian tubes) also need to be removed. The modern approach clearly suggests that the ovaries, as well as the cervix, if they are healthy, can be left.
It has also been proven that the risk of developing ovarian cancer after hysterectomy is reduced. Some sources provide the following statistics: the risk of developing ovarian cancer in women after a hysterectomy is 1/300, while in women with a preserved uterus it is 1/80.
Possible complications
Vaginal hysterectomy can cause emotional disturbances in which women feel depression, inferiority, loss of sexual desire, and increased anxiety. The risk of such complications is especially high in patients of reproductive age.
In some cases, the following undesirable consequences are also noted:
- osteoporosis;
- pain during sex;
- suture dehiscence, suppuration, swelling, infection;
- blood clot formation;
- temperature increase;
- excessive external or internal bleeding;
- prolapse of the vaginal vault;
- problems with urination.
With a high-quality preoperative examination and professional vaginal surgery, these complications are eliminated or minimized.
Psychological consequences of hysterectomy
The right psychological attitude is the key to your good health, quick recovery after surgery and a return to your usual lifestyle. For a favorable psychological state, first of all, you need trust in the doctor and confidence that your body will function the same as before the operation (which is indeed true). A positive attitude and support from loved ones are very important.
Many women attach a certain symbolism to the uterus, endowing it with super-meaning. In their minds, the uterus is, as it were, identified with the feminine essence. You can read above that the actual situation is different. If you attach great importance to the opinions of others and want to protect yourself from their negative psychological impact, then you do not necessarily need to tell them (including all close relatives, except your husband) about the details of the operation. This is the case when “a lie is for salvation.” Remember that the most important thing in this case is your health. Both physical and psychological.
Vaginal removal cost
You can see the cost of individual procedures on the website. When choosing a treatment method, doctors take into account indications, contraindications, as well as the client’s financial capabilities.
Our employee calculates the final price for all necessary procedures after examining and consulting the patient. Treatment with drugs takes precedence over surgery. If the patient is of reproductive age, the doctor does everything possible to preserve her ability to conceive. Vaginal hysterectomy is indicated only as a last resort.
You can make an appointment at our clinic through the website or by phone. Our consultants will answer all your questions in detail and tell you about the procedures and treatments that interest you.
Author of materials
Obstetrician-gynecologist of the first category
Bychkov Alexey Alexandrovich
Other articles:
Hysteroscopy Hysterectomy Hysteroscopic removal of uterine polyp Vacuum removal
Prices for vaginal hysterectomy
| G-1 | Initial appointment with an obstetrician-gynecologist | 1200 rub. |
| G-2 | Repeated appointment with an obstetrician-gynecologist | 1000 rub. |
| G-3 | Taking a smear | 420 rub. |
| G-5 | Insertion of an intrauterine device | 2600 rub. |
| G-6 | Removal of the intrauterine device with treatment | 2100 rub. |
| G-7 | Colposcopy | 1700 rub. |
| G-8 | Cauterization of cervical erosion | 5500 rub. |
| G-9 | Conization of the cervix with histological examination | 9000 rub. |
| G-10 | Removal of condylomas | 2000 rub. |
| G-11 | Cervical biopsy (without the cost of histological analysis) | 3500 rub. |
| G-13 | Opening a Bartholin gland abscess | 7000 rub. |
| G-14 | Separate diagnostic curettage (without the cost of histology and anesthesia) | 8000 rub. |
| G-15 | Taking an aspirate from the uterine cavity | 2600 rub. |
| G-18 | Diagnostic hysteroscopy | 12000 rub. |
| G-21 | Hymenoplasty (hymen restoration) | 22000 rub. |
| G-21.1 | Hymen incision | 7000 rub. |
| G-22 | Hysteroscopy | 15,000 rub. |
| G-23 | Diagnostic laparoscopy | 22000 rub. |
| G-24 | Laparoscopy planned | 27,000 rub. |
| G-25 | Emergency laparoscopy - ectopic pregnancy (with intra-abdominal bleeding), rupture of an ovarian cyst | 35,000 rub. |
| G-26 | Complicated laparoscopy - pelvic adhesions | 39,000 rub. |
| G-27 | Plastic surgery of the anterior (posterior) vaginal wall | 28,000 rub. |
| G-28.1 | Laparotomy 1st category of complexity | 30,000 rub. |
| G-28.2 | Laparotomy 2nd category of complexity | 35,000 rub. |
| G-28.3 | Laparotomy 3rd category of complexity | 40,000 rub. |
| G-29 | Emergency laparotomy | 40,000 rub. |
| G-30 | Hysteroresectoscopy | 18,000 rub. |
| G-31 | Intimate plastic surgery | 27,000 rub. |
| G-32 | Sling surgery for urinary incontinence | 27,000 rub. |
| G-33 | Surgery for prolapse of the vaginal walls using mesh prostheses | 30,000 rub. |
| G-34 | Vaginal hysterectomy | 32,000 rub. |
| G-35 | Removal of Bartholin's gland cyst | 20,000 rub. |
| G-36 | Screening examination for detection of ovarian cancer of the uterus (appointment, examination, colposcopy, oncocytology) | 3000 rub. |
| G-39 | PNVL (perineovaginal lift) | 45,000 rub. |
| G-40 | Echohysterosalpingoscopy of the fallopian tubes with contrast injection | 1000 rub. |
Go to the full list of paid gynecology services
Sex life after hysterectomy
For 1-1.5 months, sexual intercourse after removal of the uterus (as after other operations) is prohibited. This is primarily due to the necessary time required for the wound to heal.
When your body recovers and you realize that you can lead your normal life again, there will be no obstacles to sexual communication. Sensitive areas that bring a woman pleasure during sexual intercourse are located not in the uterus, but in the vagina and external genitalia.
Of course, the degree of trust in your relationship with your sexual partner plays a very important role here. It is quite possible that he will feel constrained and insecure, will try to adapt to your new state, be afraid of sudden movements and experience banal fear. At the same time, his feelings will be determined exclusively by yours. He will perceive everything adequately if you have a positive attitude towards the situation.
Remember that your partner also needs reliable information. Feel free to discuss his questions and concerns with him. If necessary, contact a gynecologist for a joint consultation - perhaps your partner will take his words with a greater degree of confidence. He must be sure that your sexual attraction and sensations will not undergo serious changes, and you can still be a desirable and sensual woman for him. The same as you were before.
So, you just need to weigh the pros and cons. The consequences of having the uterus removed will not cause you any discomfort. The choice between your health after removal of a diseased organ and your imaginary fears about changing your appearance and lifestyle is always yours.
Late rehabilitation after hysterectomy
If the operation was performed by laparoscopy, then sick leave is provided for 30 days, and for a normal uncomplicated operation - 45 days. Although there are cases where women felt good after 3 weeks and went to work.
This period begins immediately after discharge and is considered no less important than the period of early rehabilitation. You need to be no less responsible about your health and direct all efforts towards restoring the normal functioning of all organs.
During the postoperative rehabilitation period, the woman also takes medications, including enzyme, hormonal and restorative agents. While at home, you need to limit physical activity and not put stress on the muscles of the pelvic floor and abdominal cavity. If medicinal exercise has been recommended, it should not be neglected to avoid complications.
You need to abstain from sex for a month. If there is pain or suspicious discharge, you should consult a doctor. Most likely, he will prescribe additional medications and extend the period of sexual rest.
After leaving the hospital, nutrition should also not be left unattended. You need to eat only healthy foods, while limiting confectionery, alcohol, spicy, smoked and fatty foods. You need to drink as much fluid as possible, as it helps detoxify the body.
In most cases, after rehabilitation, a woman’s quality of life remains unchanged, namely:
- the menstrual cycle is restored;
- hormonal levels return to normal;
- libido remains the same;
- the opportunity to lead an active sex life returns.
Naturally, a woman loses her reproductive function, but life does not end there.
How does the absence of a uterus affect quality of life?
After physical healing, if everything went well and there is no risk of tissue sagging, the main problem may be a lack of acceptance of yourself and your body. This is a separate topic and the next task: the help of a good psychologist, the support of loved ones and your own decisive attitude will come in handy here. Otherwise, a woman can lead an active life: work, relax, have sex, go to fitness, enjoy her favorite activities - there are no obstacles to any of this after recovery. Then you just need to monitor your health: monitoring body weight and regular preventive examinations at such intervals as determined by the attending physician are especially important.
For good health, the state of hormonal levels is important - therefore, if the ovaries have been removed, then a patient of reproductive age may be prescribed replacement therapy. It will help compensate for the lack of estrogen and progesterone, female hormones responsible for maintaining youth and greatly influencing the psycho-emotional state.
What are the advantages of laparoscopic surgery compared to abdominal surgery?
Laparoscopy is a minimally invasive surgical method that is beneficial not only in the case of a small uterus, but also in the case of a large uterus. An important difference from abdominal surgery for the patient is that postoperative pain is less, which allows most patients to return home the very next day after surgery, and also resume daily activities much faster.
Main patient bonuses:
- Mild postoperative pain
- Lower risk of blood loss
- Lower risk of postoperative complications (inflammation, fever, wound inflammation)
- Faster recovery and ability to return to daily activities faster
- Best cosmetic effect
In case of various complaints related to uterine diseases, removal of the uterus is the most effective treatment method. Many studies have shown that after such an operation, even if the patient had doubts about choosing this particular method, ~95% of women were satisfied with the decision to undergo a hysterectomy.
Rehabilitation
The duration of the rehabilitation period depends on the type of hysterectomy and the general condition of the patient’s body. Upon completion of the operation, she remains under the supervision of doctors in the intensive care unit. She is given narcotic analgesics for the first 24 hours. Within a day, the patient is recommended to expand her physical activity and even sit up in bed, as this reduces the risk of adhesions and stimulates intestinal function. For the same purposes, after completing the early rehabilitation period, it is recommended to perform special gymnastics exercises. Discharge from the hospital occurs on the third or fourth day after laparoscopy and two weeks after laparotomy.
Hysterectomy at the CELT clinic
This operation is performed in our multidisciplinary clinic using endoscopic equipment. This approach is as gentle as possible and allows patients to recover much faster after the procedure. Surgical intervention is performed by specialists who have decades of experience in this field. They practice an individual approach and have modern equipment and effective medications at their disposal. Thanks to him, patients recover much faster. Contact CELT!
Is it possible to refuse the operation?
The doctor's job is to properly inform the woman about her health, treatment options, and risks. She must understand well that we are talking about a serious threat to life. It is also important to convey that after surgery, most normal activities are still available.
In case of refusal for a conditionally malignant pathology, the patient will be registered for disease control, and she will be called once every three months for an examination to check how the problem cells behave. At the same time, an ultrasound examination and aspiration biopsy are performed each time, and oncocytological tests are also taken. If a woman has been diagnosed with a borderline tumor at least once, then a test for cell malignancy should be carried out at each examination.
Here the doctor will also focus on the patient’s age and reproductive abilities: with three or four confirmations of atypical hyperplasia, he will suggest drug therapy or installation of a hormonal device to control the growth of the endometrium, but only on condition that the uterus does not bleed. This will slow down or stop the increase in mucosal thickness, normalize the cycle and eliminate abnormal bleeding. At the same time, the IUD also performs its main contraceptive function.
If the disorder is determined in a woman aged 45-49, then she will be offered a conservative-radical method - surgical treatment. In case of refusal, she is registered at the dispensary and visits the doctor once every three months for control ultrasound, aspiration biopsy, oncocytology and histological examination of the endometrium.
Patients in this group can be controlled in this way until the onset of menopause.
But this does not mean that after menopause you can forget about preventive examinations!
According to the medical protocol, having reached this period, the patient should be seen by a doctor once a year to undergo screening diagnostics in the same way: a visual examination by a doctor, an ultrasound examination, a test for tumor markers, or an extended colposcopy, and cytology tests. This applies to all women without exception.
Murad Alimardonov,
gynecologist-oncologist, candidate of medical sciences, clinic “Medicine 24/7”
“Unfortunately, the practice of cancer screening is not popular in our country - this is why most cancers of the female genital organs are detected already at the second or third stage. If, after forty years, all women underwent these tests, the disease could be diagnosed much earlier, which would greatly increase the chances of a healthy and long life. In addition, the prevention of malignant diseases of the genitourinary system and their treatment in the early stages costs the state much less than working with advanced forms.”
Indeed, if you look at the WHO’s calculations, using the example of the United States, you can see that prevention programs will cost at least three times less for the economy.
What are the advantages of modern diagnostics?
Previously, atypical hyperplasia had only one treatment option - removal of the uterus. This method was used for any age and regardless of whether the patient had given birth or planned to do so in the future.
This was explained by the difficulty of controlling the disease in the absence of normal diagnostic methods. The older generation remembers how traumatic curettage procedures were. Now it is possible to easily, quickly and on an outpatient basis, that is, without going to the hospital, to do all the tests. In just an hour and a half, a general blood test is taken, an ultrasound examination, or ultrasound, is performed - and it immediately becomes clear whether the epithelium is outside the normal range. If the doctor sees the excessive thickness of this layer, the patient is offered an aspiration biopsy - a technique that is convenient in that it does not require expansion of the cervical canal, without which it was previously impossible to identify the danger of cells inside the organ.
Preparation for vaginal hysterectomy
A planned operation requires a comprehensive examination of the patient in order to exclude contraindications and draw up a detailed plan. To do this:
- gynecological examination;
- testing for the presence of hepatitis and HIV viruses;
- general blood and urine tests;
- testing of the blood coagulation system.
- rapid diagnosis of syphilis;
- vaginal smear for flora and infectious processes;
- transvaginal ultrasound scan of the pelvic organs.
- electrocardiography;
- endoscopic hysteroscopy;
- colposcopy.
Immediately before surgery, the patient needs to remove hair from the genitals and perineum and undergo a cleansing enema. If she suffers from varicose veins of the lower extremities, she needs to bandage her legs with elastic bandages. You should avoid eating food at least eight hours before surgery.