Oncological diseases are a real scourge of modern humanity. Every year, more and more new cases of cancer of various localizations are registered all over the world, and colon cancer ranks third among them. Early detection of this disease gives a good prognosis and allows the use of more gentle, non-disabling methods of treatment. Therefore, such great importance is attached to preventive examinations using reliable research methods.
The “gold standard” of modern diagnosis of colon tumors is colonoscopy. This procedure is also called fibrocolonoscopy (FCS) or video colonoscopy. Currently, colonoscopy in St. Petersburg is carried out in comfortable conditions for the patient, using general anesthesia (anesthesia).
What is the essence of colonoscopy?
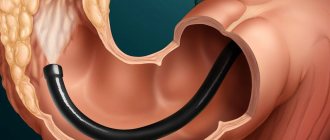
Fibercolonoscopy is an examination of the surface of the mucous membrane of all parts of the large intestine using an endoscope camera. The device used in this case is called a colonoscope; its working part is carefully inserted into the intestinal lumen through the anus. Modern models look like a flexible thin tube; if the doctor is sufficiently qualified, their advancement is not accompanied by severe pain and does not lead to tissue damage.
The image received by the camera is processed and transmitted to the monitor screen. The level of detail depends on the hardware class, screen resolution and the presence of additional software.
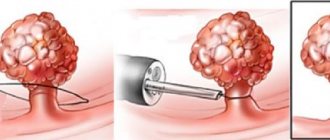
If suspicious (modified) areas of the mucous membrane or space-occupying formations are identified, the doctor performs a biopsy - using manipulators, he separates a piece of tissue for subsequent analysis. It is also possible to simultaneously remove small tumors (for example, polyps).
A comfortable option for FCS is to carry out the procedure under anesthesia, when the patient is immersed in a controlled medicated sleep. In this case, the team of doctors includes an anesthesiologist-resuscitator. After completing the procedure, the patient stays in the clinic for some time and returns to everyday life within a few hours.
Why is it better to do the procedure at the Central Clinical Hospital of the Russian Academy of Sciences?
When choosing a clinic for an informative, but not very pleasant (without anesthesia) examination, you should first of all focus not on the cost of the procedure, but on factors such as the experience and qualifications of doctors, hospital equipment, and patient reviews. The Central Clinical Hospital of the Russian Academy of Sciences offers many advantages:
- painlessness of the procedure;
- high-precision modern equipment;
- high level of qualification of specialists;
- professionalism of experienced doctors in making a diagnosis and prescribing effective treatment;
- affordable price of the procedure.
The clinic staff considers tactfulness, attention, willingness and ability to help to be a priority in relations with patients. Already at the first meeting, during the consultation, the doctor simply and clearly conveys important information about colonoscopy - how to prepare for it, how long the examination will last, what can and cannot be done the day before and on the day of the procedure. This creates a certain mood and inspires trust. This means that the result of a well-thought-out treatment method after an informative, most gentle diagnosis will be wonderful.
What can be revealed
FCS with anesthesia allows you to:
- carry out differential diagnosis between chronic diseases with colitis syndrome;
- identify diverticula;
- detect polyps and other benign neoplasms and remove them endoscopically;
- detect malignant tumors (cancer) of any form at the earliest stages, when they are still small in size and limited to the mucous membrane and submucosal layer.
At the moment, FCS is the most informative, reliable and safe way to assess the condition of the wall of the large intestine and identify any neoplasms located here.
Why do this research?
Diseases of the large intestine (rectum and colon) have become increasingly common in the last decade. Many doctors, regardless of specialization, encounter the phenomenon of chronic constipation (colostasis) in their daily practice. Being, of course, most often a symptom of many other, not only proctological diseases, constipation in many cases becomes an independent syndrome that has no “apparent” cause. Today it is clear that chronic constipation plays an important role in the development of other lesions of the colon, including polyps and cancer.
At the age of 45–50 years, benign polyps often appear in the colon and begin to grow slowly, most of which are true glandular adenomas, precancerous diseases. For a long time they are completely asymptomatic and are detected only during sigmoidoscopy and colonoscopy. This often leads to a late diagnosis of colon cancer, because in the vast majority of cases these are stages of one process. Other very common diseases that doctors of various specialties encounter in their practice are functional intestinal dyspepsia, dysbiosis, irritable bowel syndrome and various forms of colitis.
Medical statistics also confirm the importance of colonoscopy. Mass examinations (screening) have shown that 25% of practically healthy adults are diagnosed with proctological diseases (every fourth practically healthy person). As with other diseases, outpatients outnumber inpatients.
Noteworthy is the fact of such a nonspecific condition, which is defined as colon aging syndrome, and its connection with certain diseases of the colon, including polyps and cancer. This syndrome is not determined by the age of the patient, but by the duration of functioning of the decompensating organ system, since intestinal pathology, as a complex therapeutic problem, often remains behind the scenes.
Is it possible to replace the FCC with something?
As an alternative, FCS often offers irrigoscopy and CT. In fact, these techniques cannot fully replace endoscopic examination. They do not allow a detailed and targeted examination of the tumor, do not detect small defects in the mucous membrane and do not allow a biopsy. In addition, these techniques involve the use of radiation, which imposes certain restrictions on the timing of re-diagnosis.
Fibercolonoscopy is the optimal method for assessing the condition of the walls of the large intestine and the most informative way for the early detection of colorectal cancer.
Unfortunately, more than 1/3 of malignant colon tumors are diagnosed at late stages, which explains the high mortality rate from this disease. In many cases, this is due to patients’ unreasonable refusal of recommended regularly repeated endoscopy. The lack of information content and reliability of screening studies carried out in clinics, with preference for laboratory or X-ray diagnostics, is also of certain importance.
Side effects of colonoscopy
Colonoscopy usually goes without consequences. Serious complications occur very rarely. Most often they are associated with the doctor’s lack of experience in performing such endoscopic manipulations. Possible risks include:
Why is anesthesia needed for FCS?
Colonoscopy under anesthesia relieves the patient of the physical and psychological discomfort associated with the insertion and advancement of the colonoscope tube. He will not experience pain during a biopsy, if there is a need to take tissue samples for histological examination.
Anesthesia makes it possible to avoid the formation of fear of repeated FCS, so that the patient in the future will not avoid the recommended scheduled regular examinations. According to reviews, after a colonoscopy in a state of medicated sleep, there is no pain in the anus and in the abdomen.
The use of anesthesia also improves the quality of the examination. Moderate muscle relaxation in a sleeping patient and the absence of involuntary resistance on his part give the doctor the opportunity to carefully examine the folds of the mucosa in all parts of the large intestine.
Preventing constipation after colonoscopy
Prevention of constipation after colonoscopy begins at the preparation stage. So, the doctor will prescribe a suitable laxative for complete cleansing and give recommendations regarding the use of other medications.
It is important to adhere to a special diet some time before the diagnostic procedure. This will help improve visualization of the inner surface of the intestine, eliminate the formation of large amounts of gas and reduce the likelihood of complications. Lack of thorough preparation may lead to the need to repeat the procedure, so you should not neglect preparation.
In order to prevent disturbances in bowel function after endoscopic intervention, it is important to adhere to the recommendations of a specialist. Your doctor may prescribe the following medications:
- analgesics for pain relief;
- defoamers, sorbents to eliminate increased gas formation: with low risks of developing constipation;
- laxatives;
- prebiotics to normalize intestinal microflora.
If there are no contraindications to moderate physical activity, it is important to move. Light exercise and walking are suitable. It is better to avoid heavy loads.
Compliance with the drinking regime is of great importance in the prevention of constipation in general and after colonoscopy in particular. It is important to drink up to 2 liters of water per day to ensure normal bowel function and normal stool consistency. If you take diuretics, ask your doctor how much fluid you need per day.
When determining the required volume of water, we need to take into account all the liquid that we consume per day: tea, soups, vegetables, fruits (they also contain water). But none of the above can completely replace water; it will only reduce the required volume.
After the intervention, it is important to adhere to a special diet. The principles of postoperative diets are suitable, but not with such strict restrictions. So, the daily menu should include cereals, lean meats and fish, and fermented milk products. You need to avoid smoked meats, marinades, spicy foods, fried and fatty foods, as well as ready-to-eat foods - sausages, confectionery, etc.
If constipation may occur due to a disease of the digestive system, seek your doctor's recommendations for prevention.
Preparing for the FCC
Preparing the patient for the study includes:
- Examination to exclude contraindications to anesthesia. It is necessary to donate blood for general and biochemical tests, do an ECG (with interpretation), if you have chronic diseases, consult a therapist, and if there are severe hormonal disorders, consult an endocrinologist.
- Following a certain diet aimed at reducing gas formation in the intestines and reducing the volume of intestinal contents. For 3–5 days before the procedure, fruits, vegetables, seeds, nuts, most cereals, legumes, and sweets (sweets, chocolate, baked goods) are excluded from the diet. Consumption of milk and fatty fermented milk products is undesirable. Alcohol, juices with pulp, and strong broths are prohibited.
- Avoid eating for 16–20 hours before your scheduled examination. You can drink water and prescribed medications no later than 3-4 hours before the procedure.
- Limit smoking; it is advisable to temporarily quit smoking a few hours before anesthesia.
- Cleansing the large intestine to the state of transparent, slightly colored and liquid stool. Previously, repeated enema was used for this; now drug preparation for the procedure is preferred. ICLINIC doctors recommend using the drug Moviprep for this; a detailed dosage regimen can be clarified with the clinic’s specialists.
Preparing for a colonoscopy is the most important stage of the study. Properly performed bowel cleansing significantly increases the degree of visualization of the upper parts of the colon, expands the diagnostic capabilities of the technique and increases the reliability of the results. And following the rules of preparation for anesthesia makes it easier to tolerate and eliminates the risk of complications.
A delicate problem
Very often, a trip to the proctologist is postponed until the last minute. And talking about any problems with the intestines is considered something shameful. But you need to understand that if you contact specialists in a timely manner, then diagnosing any problem will not be difficult.
In most patients, the imagination often works “in the wrong direction.” They have a distorted understanding of how this research is conducted. Many people think that they are in for torment and inconvenience, but medicine has long stepped forward in this aspect and has created all the conditions for complete comfort for patients.
How often should you have a colonoscopy?
According to modern clinical guidelines, indications for FCS include:
- Previously diagnosed chronic bowel diseases.
- The patient has a history of a polyp or other benign neoplasm in the gastrointestinal tract.
- Identification of indirect signs of a tumor according to other research methods (ultrasound, radiography, irrigoscopy, etc.).
- The patient develops symptoms suspicious of tumor growth. These include unstable stools, recurrent or chronic abdominal pain, persistent low-grade fever, detection of blood or mucus in the stool (outside the phase of acute diarrheal infectious syndrome), chronic treatment-resistant anemia (iron deficiency or B12 deficiency), persistent increase in ESR and a number of other signs.
- The patient has cancer risk factors, a hereditary history of gastrointestinal cancer. Currently, permanent residence in large cities and in areas of increased industrial pollution is considered as a predisposition to cancer, including colorectal localization.
Persons with chronic gastrointestinal pathology, previously diagnosed diverticulitis and intestinal polyposis are recommended to undergo fibrocolonoscopy at least once a year. The frequency of visits is determined by the doctor individually; in some cases, diagnostics are carried out every 6–8 months. People from the high-risk group aged 40–45 years are recommended to undergo FCS once every 2 years, and after 45 years – annually.
“We can do more than our patients think. Even some colleagues don’t always know what we are capable of,” says Alexey Petkevich, an endoscopist with 22 years of experience. He has performed several thousand endoscopic procedures and operations, thanks to which his patients did not end up on the operating table of surgeons. About the features of gastro- and colonoscopies, screening and prevention of colorectal cancer, the possibilities of its treatment at the RCMC - in an interview with a specialist.
Alexey Alekseevich Petkevich.
Endoscopist, head of the endoscopic department of the Republican Medical Clinical Center. Work experience - 22 years. In RCMC - since 2010. Before that, he worked as a doctor at the Polotsk Oncology Center for 12 years. “The main rule is this: if a person has a stomach ache and he cannot explain to himself the cause of the pain, he definitely needs to see a doctor.” “
In our department, we conduct two main studies: gastroscopy and colonoscopy,” Aleksey Alekseevich begins the conversation. — A little less often, because bronchopulpomonology is not our specialty, we do bronchoscopy. This means that the endoscope is inserted into the lumen of the bronchial tree, and we can see a lot: tumors, narrowings, and foreign bodies.
Today, endoscopy has made great progress. We can do more than our patients think. Even some colleagues don’t always know what we are capable of. In cases where previously there were all indications for surgical treatment, we can now help endoscopically.
- For example?
“We recently worked with a patient who had very complex choledocholithiasis. A huge stone was discovered in the bile duct, which had formed after the gallbladder was removed. The size of the stone was about two centimeters; it was impossible to catch it with the endoscopic basket. In different clinics they tried to help the girl more than once by penetrating the bile duct through the duodenum. But they couldn’t, because the case was really difficult.
We decided to carry out a rather complex procedure: we cut the papilla of Vater with a needle, penetrated it with a cholangioscope [a subsidiary endoscope that is inserted into the main one. - Note], they found a stone. Then they used a laser to destroy it into small pieces that could be removed with ordinary baskets.
In general, today this is a fairly developed branch of endoscopy, which opens up a lot of opportunities. In essence, we are taking work away from surgeons, which benefits patients: during surgical operations, the rate of complications is an order of magnitude higher.
— What usually brings a person to endoscopic examinations?
— I would divide endoscopy from the point of view of prevention and treatment into two large groups: the one where there are no indications for endoscopy, and the one where there are.
“Indicated without indication” is another way to call screening. We have developed colon screening in our clinic. We conduct its study without indications or symptoms in patients over 50 years of age. Although, I think this lower threshold will shift to 45 years. If there are indications for gastro- or colonoscopy, then, as a rule, patients are referred for these procedures by therapists, gastroenterologists or surgeons. The patient should not prescribe endoscopy for himself. What symptoms usually bring people to the doctor? In the esophagus - this is a violation of swallowing, in the stomach - pain in the upper abdomen. In the large intestine - constipation, diarrhea, blood in the stool. A drop in hemoglobin can be a symptom of both stomach and colon diseases. In this case, endoscopic examination is also indicated. The retelling can take a long time.
Therefore, the main rule is this: if a person has a stomach ache and cannot explain to himself the cause of the pain, he should definitely consult a doctor.
Abdominal pain, indigestion, loss of appetite or increased appetite may all be indications for testing. But differentiating pain is the doctor’s concern. The patient cannot diagnose himself. He will only read articles on the Internet and find one diagnosis worse than another.
Gastroscopy: when is it prescribed, how long does the procedure last, how to prepare for it and why do a biopsy
— Let's talk about gastroscopy. Performing this procedure, which is commonly called “swallowing a probe,” is not always easy. What challenges do you face and how do you solve them?
“There are patients who have a strong gag reflex or are not psychologically ready for this study. Some people are so stressed that they basically cannot undergo the examination without anesthesia. In such cases, intravenous anesthesia helps. The patient is sleeping, the doctor is performing the procedure. Everything goes smoothly.
- Who decides whether to give anesthesia?
— The patient together with the doctor. It happens that at the initial appointment a person does not know that he may have a similar reaction. And when he comes for research, the tense state may come as a surprise to everyone. In order not to harm the patient, we stop the procedure and give a recommendation for subanesthetic endoscopy. Before it, the patient must be examined and prepared. There are no problems with this in our clinic.
— How long does the procedure take under anesthesia?
- The same as without it. An examination of the stomach, for example, lasts about 7 minutes.
Some patients ask: “Do it for me quickly.” But this is the wrong approach. It must be done as long as necessary to examine all areas of the stomach, scan in a narrow spectrum of illumination, assess the condition of the mucous membrane, identify submucosal formations, narrowing or compression of the stomach, and so on. A quick examination can reveal gross pathology, but anything less noticeable requires a more detailed examination.
— What rules should the patient follow before the gastroscopy procedure?
- First of all, it must be on an empty stomach. Food leaves the stomach on average after six hours - from 4 to 8. If patients have narrowing or ulcerative scars, then this period extends to 12 hours. We generally recommend not eating after 6 pm the night before, but drinking is fine. In the morning - neither drink nor eat. The stomach should be empty.
— What is dangerous about breakfast or a light snack before the procedure?
— Firstly, food residues interfere with research. Secondly, they are truly unsafe for the patient. If vomiting occurs, a person may accidentally inhale food, causing pneumonia.
Experienced doctors can distinguish food that has just been eaten from food that has been in the stomach for many hours, no matter how disgusting it may sound to the average person. We see that some people forget about the rule and hope to “slip through somehow.” But this is really dangerous, especially if they mislead the anesthesiologist. If a patient vomits unnoticed while under anesthesia, this can even lead to death.
Therefore, we have a rule: if we go into the stomach with a probe and see that there is food there, we immediately take out the endoscope and stop the study, because this is dangerous not only for the health, but also for the life of the patient.
— Is a biopsy always done during gastroscopy? What does this depend on?
— With conventional endoscopy, if we do not see indications for an extended biopsy, material is taken from two zones: from the antrum and body of the stomach. This is necessary in order to assess the presence of Helicobacter infections and atrophy (thinning of the gastric mucosa), which in the future can lead to a malignant process.
Is a biopsy always performed? We insist that this always be the case. The exception is when patients are on drugs that reduce blood clotting. Otherwise it may lead to bleeding. It happens that we do not do a biopsy if the patient refuses. He has this right.
Colonoscopy: how to overcome fear, why anesthesia, how to prepare for the examination
— From the age of 50, Belarusians are subject to a colorectal cancer screening program and must undergo a colonoscopy. Right?
- Yes. From 2014 to 2018, research work was carried out at our center. This was a large program for screening and secondary prevention of colorectal cancer in Belarus, for which we took the best world experience. Its result was the creation of an order, thanks to which colon cancer screening is being introduced in the country.
Moreover, of all cancer localizations, this screening can be called the most difficult - in terms of its organization and implementation.
- Why?
- At least because of the psychological barrier. It is one thing to take blood from a vein, another to do a colonoscopy, in which a probe is inserted through the anus. In addition, feces are examined for occult blood. This means you need to take a sample yourself. For many, this is a difficult psychological barrier to overcome.
Plus, to perform a colonoscopy, the intestine must be prepared - it must be washed of feces. This is not always easy either. If anyone has been preparing, they will understand immediately. If not, then this is what it looks like: you need to drink 4 liters of the drug and survive the induced diarrhea.
It is not easy to persuade people to undergo these procedures. When we were working on the program, every fifth person refused to participate in it for free.
— A 50-year-old person who is eligible for colorectal cancer screening undergoes a colonoscopy. If nothing is found, when should it be done next time?
— Primary colonoscopy is done at 50 years of age. Based on its results, it is determined how long it will take to carry out the procedure next time.
If the colon is absolutely clean, the doctor did not find anything - the next colonoscopy should be done in 10 years. If there are polyps, the period depends on their number and morphological state. On average - from 3 to 5 years.
Every year, colonoscopy is performed only for those who have a genetic predisposition to colon cancer. These patients are only 10 percent.
There is no fulminant course of cancer. It has been proven by science: if nothing is found in the intestine, if its mucous membrane is clean, without adenomas, then in 10 years a person will not die from cancer. And even if after 10 years something appears, it will be curable and treatable. We did not come up with this standard; it is practiced in the USA and Europe.
— Your colleague, oncologist Yuri Slobodin, says that now the rate of development of colorectal cancer is such that it can come out on top. Are you also seeing this trend?
- Certainly. We identify an adenoma (polyp) in every third patient. This is a strong indicator for assessing the work of the endoscopist in particular and the endoscopy department in general. If it is below 20 percent, it means that the endoscopist is not working well.
Our average rate for the screening program, that is, among patients who did not need to have a colonoscopy according to indications, is about 35 percent. Interestingly, the figure is approximately the same in the group of patients aged 45-50 years.
— Are polyps the precursors of colorectal cancer?
- They are called adenomas in another way. It is believed that this is an intermediate stage between healthy mucosa and cancer. Adenoma has two degrees of dysplasia: low and high. The next step is cancer.
— If the patient is under 50 years old, for what indications can he be prescribed a colonoscopy?
- When a person has unexplained constipation, diarrhea, bleeding in the stool, decreased hemoglobin, or large tumors are found in the abdominal cavity, metastases without a primary focus.
— Is colonoscopy always performed under anesthesia?
— There is a group of patients who can have a colonoscopy really painlessly. But, unfortunately, not everyone.
I have been working as an endoscopist for 22 years and have more than once entered into discussions with younger colleagues who say that “yes, everyone can do it without anesthesia.” To which I answer: “A patient to whom you could not do it simply did not come to you.” I've performed over 11,000 colonoscopies and I'm probably qualified to say that.
Most patients need to have a colonoscopy under anesthesia or sedation. The patient must be calm during the procedure. Then, accordingly, the doctor will be calm. All together this means that the level of diagnosis will be higher. When the doctor gets tired of the patient’s nervousness, his eyes become blurred. This increases the likelihood of overlooking minor pathologies. Sometimes nurses help. Ours are already so experienced that sometimes they see polyps before the doctor. I am happy to work with such colleagues. And this does not at all humiliate my dignity as a doctor.
— That is, anesthesia is used in cases where it is impossible to carry out the procedure without psychological stress?
— Let's put it this way: about 90 percent of our procedures are performed under intravenous anesthesia. This is the highest figure. We were the first to establish such a flow. We have a recovery room and all the conditions so that the patient is protected and we can perform the procedure painlessly.
During the first colonoscopy, I cannot predict how the patient will behave. And I won’t be able to give a guarantee that “I will treat this patient without pain, and this one with pain.” With anesthesia, I know for sure that the patient will be calm. But in general, the number of patients who write on the Internet that a colonoscopy is terribly painful is 5-10 percent. A person who has had the procedure done and was not in pain is unlikely to start writing reviews and spreading the word that he had a colonoscopy.
— How long does this procedure take?
— It all depends on the skill and qualification level of the specialist. As elsewhere, different people need different amounts of time to do the same job.
I can perform a colonoscopy in 20 to 40 minutes. But this does not mean that everyone can do this. It can be done in 15 minutes if the intestine is prepared and it is not anatomically changed. The Japanese standard is 5 minutes there, at least 10 minutes back. More is possible, and this is welcome. As paradoxical as it sounds, with experience and excellent equipment, our time for the procedure increases. Because in reality we see more complex things that are invisible on endoscopes of previous generations. If we find small polyps that do not raise doubts about the presence of invasive cancer, we remove them immediately. That is, the patient does not go to the second round - with repeated preparation for colonoscopy, four liters of the drug, and so on.
If there are doubts about polyps, we take a biopsy to examine the formation for the presence of cancer cells.
— Do I understand correctly that a polyp will sooner or later turn into cancer?
- Not always. According to various sources, benign neoplasms of the colon transform into malignant ones in 8-15 percent of cases. But if we find an adenoma, then it needs to be removed. We will not leave it even with an 8-15 percent risk.
— What causes a benign tumor to become malignant? Just because it has such a “life cycle”? Or could this be influenced by some factors?
— There are a lot of factors. The first is nutrition. Today we cannot imagine our life without “chemistry”. Everything we eat eventually turns into feces. Naturally, all the substances eaten will be released along the gastrointestinal tract. They stay the longest in the large intestine. Accordingly, this is where they show their aggression most.
If we eat foods that contain fewer harmful chemicals, we will be less likely to get any tumors. If you constantly throw smoked meats, fats, and the like into your intestines, then the situation will be the opposite.
By the way, smokers have a very high risk of colon cancer. I don’t know how to explain this yet. But in studies of groups of smokers, the incidence of colon cancer is higher.
In general, colon cancer is spreading across the planet by leaps and bounds. In 2014, we prepared an article in which there was data that every year 600 thousand people die from colon cancer in the world. Five years later, this number surpassed the 800 thousand mark. And this is despite the presence of screening programs in many countries of the world. Morbidity and mortality rates are rising. Although there are countries, including the United States, in which both mortality from colon cancer and morbidity are decreasing.
***
— In your department, you have the opportunity to record the research itself. For what?
- Firstly, if necessary, review the recording with the surgeon and plan medical tactics.
We can also record the research and show it, in case there are questions that we didn’t see something.
It happens that patients go somewhere else for consultation. For example, to Israel. They take the notes and show them to other doctors.
— What can be considered complications during endoscopic examinations and operations?
— Endoscopy has two serious complications: bleeding and perforation.
I've had perforations on even the smallest polyps when I didn't expect it to happen. We analyzed situations and found reasons. In medicine, you need to treat any pathology with respect, because when a doctor begins to think that he has become something more than just a doctor and a person, then something terrible happens.
We must always remember that we are simple people who can make mistakes out of the blue. You need to be prepared for this at any moment. The most valuable clinic and the most valuable doctor is the one who knows how to not just operate, but how to get out of difficult situations. We don’t deliberately provoke them, but if something happens, it becomes a most valuable experience. Just like in aviation, all instructions are written in blood. It's about the same with us.
****
— Endoscopy is more than even your colleagues think, you said at the beginning. It gives more opportunities and fewer complications...
“And it is easier to tolerate, and patients recover faster than with surgery. After all, for example, with cholecystitis, it is not the site of the removed gallbladder that takes longer to heal, but the cut abdomen. Laparoscopic and minimally invasive surgeries can avoid this.
— How is the decision made: will a surgeon operate on a person or will an endoscopist work with him?
“We always have time to give it to the surgeons.” Therefore, we work with the patient as much as possible, doing everything possible with the arsenal of tools that we have.
If we see that we no longer have the opportunity to continue endoscopic treatment, we refer the patient to surgeons.
— What operations do endoscopists perform?
— First of all, submucosal desection. If there is no invasion - penetration into the muscular plate of the mucosa, then the malignant tumor can be removed. Basically, the fight is against tumors that have high-grade dysplasia, that is, when there is one step left to a malignant tumor, but it is still soft and can be peeled off. But you need to work like a jewel. However, as in any business.
FCC in ICLINIC: competent approach and modern technologies
ICLINIC Medical Center specializes in the prevention and diagnosis of cancer of the digestive system. Our diagnostic equipment is certified, has high grades and is additionally equipped with special software to increase the information content of studies. The colonoscopes used have a reduced tube diameter, high-precision cameras and monitors, and allow virtual chromoendoscopy of the smallest formations identified. All this ensures high diagnostic information content and reliability of the FCS.
The base price for video colonoscopy at ICLINIC in St. Petersburg is 5.5 thousand rubles. It may change during additional consultations with an anesthesiologist, endoscopist, leading specialist E.I. Levchenko, when using anesthesia of varying complexity, when taking a biopsy.
The affordable price of colonoscopy at our ICLINIC center in St. Petersburg is an opportunity to undergo a highly accurate examination of the large intestine using high-quality equipment and in comfortable conditions. Each patient receives a qualified written report drawn up in accordance with current clinical guidelines and protocols. The ICLINIC doctor also gives recommendations on the prevention and treatment of identified changes, and will suggest the optimal program for further examination.
To do a videocolonoscopy at ICLINIC, you can contact our administrators using the feedback form or by calling the phone numbers listed on the website.
When can I get my colonoscopy results?
A description of the intestinal condition can be obtained a couple of days after the procedure. If a biopsy was performed during colonoscopy, the time period increases until the histological examination data is obtained. In the conclusion, the compliance of the patient’s intestinal tube with certain criteria is indicated, as well as additional manipulations performed (if any). In addition to documents, you will be given a disc with a photograph or a reproduction of the colonoscopy process. Patients pass on the information received to the attending physician to determine further tactics for patient management.
Test for the probability of stomach cancer
Are you over 45 years old?
Did your relatives have cancer?
You have chronic diseases of the gastrointestinal tract: - chronic gastritis, - peptic ulcer, - chronic colitis and other inflammatory bowel diseases, - Crohn's disease, - ulcerative colitis, - previously identified polyps of the stomach and intestines, - identified submucosal epithelial formations of the gastrointestinal tract -intestinal tract?
Have you had surgery on the stomach and intestines?
Do you have scar-adhesive changes in the gastrointestinal tract?
Do you smoke (more than 1 cigarette per day)?
Do you make mistakes in your diet (low consumption of vegetables and fruits, high consumption of meat and animal fats)?
How to use fiber correctly
An adult should receive from 25 to 35 grams of fiber per day so that his gastrointestinal tract functions stably and predictably. This amount is quite difficult to obtain from diet alone, even if your diet includes vegetables and legumes - the main sources of dietary fiber. Therefore, you can choose an effective drug for yourself.
One of them is the English drug “Fitomucil Norm”. It does not contain preservatives, flavor enhancers or dyes. It contains only plant components:
- plantain seed shell (psyllium);
- dried home plum fruits.
“Fitomucil Norm” is packaged in portioned packages. The contents of the sachet should be mixed with a glass of liquid at room temperature and drunk. Drink a glass of water. In case of constipation, it is generally important to maintain a drinking regime: at least 1.5–2 liters per day. The product gently stimulates the intestines and does not cause pain or bloating. You will find detailed information about the drug on the website.