Thyroiditis is a group of diseases in which, for some reason, inflammation occurs in the thyroid gland. As the process progresses, its work is disrupted, the amount of hormones it produces increases or decreases. Without treatment, thyroiditis can lead to the destruction of gland cells, including complete atrophy.
Thyroiditis symptoms are curable (with timely initiation of therapy). Let's take a closer look at the causes and symptoms of thyroiditis, treatment options, and whether it is possible to protect yourself from the disease.
Thyroiditis and its types
Inflammation (including in the thyroid gland) occurs for various reasons and can occur in different ways. Based on these factors, according to the International Classification of Diseases (ICD-10), the following main types of thyroiditis are distinguished:
- Autoimmune or chronic Hashimoto's thyroiditis (in honor of the Japanese scientist who studied and described the disease in 1912).
- Acute - an infectious lesion with focal or diffuse (complete) inflammation in the gland.
- Subacute - has three forms: granulomatous, lymphocytic and pneumocystis.
- Chronic – inflammation of the fibrous type.
There are also such types of thyroiditis as postpartum and medicinal. The first can develop in pregnant women, appear after childbirth, and the second appears as a side effect of medications. This pathology cannot be treated separately; everything returns to normal on its own after a while.
General symptoms of thyroiditis of the thyroid gland include general weakness and malaise, neck pain, which increases with pressure on the area where the thyroid gland is located. Later, swelling and bradycardia develop, memory and performance deteriorate, and body temperature decreases.
Any signs of malfunction of the thyroid gland are a good reason to urgently visit a doctor.
You should not self-medicate or suppress symptoms with medications. This will not help, but will only make the situation worse. You will still have to treat the disease, but it will be much more difficult.
Any disease is easier to treat in its early stages.
With us you will receive full qualified medical care. We do not apply standard approaches to all patients. Individual treatment is selected for each patient after a thorough examination. Make an appointment at the Kutuzov Diagnostic and Treatment Center. We pay maximum attention to the problems of each patient and are always ready to help you.
Each form of inflammation has its own characteristic features of course and treatment.
Diffuse euthyroid goiter: diagnosis and treatment
The term “diffuse euthyroid goiter” (DEG) refers to visible and/or palpable enlargement of the thyroid gland.
DEZ is a general diffuse enlargement of the thyroid gland without disrupting its function. The main cause of ECD is insufficient iodine content in the environment and, as a consequence, reduced iodine consumption by the population through usual food products. Depending on the prevalence of ECD, sporadic and endemic goiter are distinguished in the population.
Goiter is considered endemic if in the surveyed region the incidence of goiter in children of primary and secondary school age is more than 5%. DEZ is a pathology of young people. In more than 50% of cases, it develops before the age of 20, and in women goiter develops 2-3 times more often than in men, and, as a rule, during those periods when the need for iodine is increased (puberty, pregnancy , lactation).
According to the criteria adopted by WHO, UNICEF (United Nations Children's Fund) and ICCIDD (International Council for the Control of Iodine Deficiency Disorders), a region can be considered free of iodine deficiency if the median iodine content is between 100 and 300 µg/l, and the prevalence goiter does not exceed 5%. In Russia there is practically no territory that is free from the risk of developing iodine deficiency goiter. According to epidemiological surveys from 1991–2006, the frequency of various forms of goiter in the Russian Federation ranges from 10 to 40%.
The most common cause of ECD is iodine deficiency. In this case, hypertrophy and hyperplasia of the thyroid gland are compensatory in nature and are aimed at providing the body with thyroid hormones. What are the mechanisms of such adaptation to insufficient iodine intake?
Firstly, the absorption of iodine by the thyroid gland increases due to increased active uptake.
Secondly, there is a predominant synthesis of triiodothyronine (T3), which is the most active thyroid hormone, while its synthesis requires not 4, but only 3 iodine atoms.
Thirdly, the secretion of iodine by the kidneys decreases, the reutilization of endogenous iodine increases, which increases the efficiency of the biosynthesis of thyroid hormones.
Fourthly, the iodine content in the colloid decreases (due to the preferential synthesis of monoiodotyrosine rather than diiodotyrosine) and thyroglobulin in the colloid (due to increased proteolysis).
In the early stages of goiter development (i.e., in children, adolescents and young adults), compensatory hypertrophy of thyrocytes occurs. The thyroid gland is represented by a mass of small follicles that practically do not contain colloid. Such a goiter is called parenchymal, it is the result of successful adaptation.
Another morphological variant of DEZ is colloid goiter. It consists of large follicles containing a huge amount of colloid. When this type of goiter forms, a number of mechanisms interfere with the optimal functioning of the thyroid gland. An imbalance occurs between the synthesis and hydrolysis of thyroglobulin, and the degree of iodization of thyroglobulin decreases. There is a leakage of iodine from the thyroid gland and a decrease in the synthesis of iodothyronines. Changes of this type predominate in the thyroid tissue of operated patients.
There is no doubt that all adaptation reactions are stimulated and controlled by thyroid-stimulating hormone (TSH). However, as has been shown in many studies, TSH levels do not increase in ECD. A number of in vivo and in vitro studies have provided new data on the autoregulation of the thyroid gland by iodine and autocrine growth factors (AGFs). According to modern concepts, an increase in TSH production or an increase in the sensitivity of thyrocytes to it is only of secondary importance in the pathogenesis of iodine deficiency goiter. The main role is played by AGF, such as insulin-like growth factor type 1 (IGF-1), epidermal growth factor (EGF) and fibroblast growth factor (FGF), which, in conditions of decreased iodine content in the thyroid gland, have a powerful stimulating effect on thyrocytes. It was experimentally shown that when KI was added to the thyrocyte culture, there was a decrease in TSH-induced, cAMP (cyclic adenosine monophosphate)-mediated expression of M-RNA IRF-1, with its complete cessation with a significant increase in the dose of iodide.
It is well known that iodine itself is not only a substrate for the synthesis of thyroid hormones, but also regulates the growth and function of the thyroid gland. Thyrocyte proliferation is inversely related to intrathyroidal iodine content. High doses of iodine inhibit iodine absorption, its organization, synthesis and secretion of thyroid hormones, and absorption of glucose and amino acids. Iodine, entering the thyrocyte, interacts not only with tyrosyl residues in thyroglobulin, but also with lipids. The resulting compounds (iodolactones and iodaldehydes) are the main physiological blockers of ARF production. Many different iodolactones have been identified in the human thyroid gland, which are formed due to the interaction of membrane polyunsaturated fatty acids (arachidonic, doxahexene, etc.) with iodine in the presence of lactoperoxidase and hydrogen peroxide.
In conditions of chronic iodine deficiency, there is a decrease in the formation of iodine lipids - substances that inhibit the proliferative effects of ARF (IRF-1, FGF, EGF). In addition, with insufficient iodine content, the sensitivity of these ARFs to the growth effects of TSH increases, the production of transforming growth factor-b (TGF-b), which is normally an inhibitor of proliferation, decreases, and angiogenesis is activated.
All this leads to an enlargement of the thyroid gland, the formation of iodine deficiency goiter.
In general, the development of ECD depends on many factors that are not fully understood. In addition to iodine deficiency, other factors related to the development of goiter include smoking, taking certain medications, emotional stress, and areas of chronic infection. Gender, age, and hereditary predisposition also matter.
With endemic goiter, genetic predisposition can only be realized in the presence of a corresponding external factor - iodine deficiency in the environment. In the absence of a genetic predisposition, mild or even moderate iodine deficiency may not lead to the formation of a goiter, since this deficiency will be compensated by the more efficient functioning of the systems that provide the synthesis of thyroid hormones. In case of severe iodine deficiency, even the maximum activation of compensatory processes cannot always prevent the formation of goiter in individuals who do not have a genetic predisposition.
To assess the degree of enlargement of the thyroid gland by palpation, WHO (2001) recommends the following classification.
Zero degree - there is no goiter (the volume of each lobe does not exceed the volume of the distal phalanx of the subject's thumb).
1st degree - the goiter is palpable, but not visible with a normal neck position. This also includes nodular formations that do not lead to an enlargement of the gland itself.
2nd degree - the goiter is clearly visible in the normal position of the neck.
The sensitivity and specificity of the palpation method for assessing the degree of goiter is quite low. Therefore, to accurately determine the size and volume of the thyroid gland as part of an epidemiological study, ultrasound examination (ultrasound) is recommended.
The volume of the thyroid gland is calculated taking into account the width (W), length (L) and thickness (T) of each lobe and the ellipsoidal correction factor using the following formula
V shzh = [(Shpr x Dpr x Tpr) + (Shl x L x T)] x 0.479.
In adults, goiter is diagnosed if the volume of the gland, according to ultrasound, exceeds 18 ml in women and 25 ml in men. In a child, the volume of the thyroid gland depends on the degree of physical development, therefore, before the study, the child’s height and weight are measured and the body surface area is calculated using a special scale or formula. In children, the volume of the thyroid gland is compared with standard values (depending on body surface area).
The clinical picture of DEZ depends on the degree of enlargement of the thyroid gland, since its function remains normal. The mere fact of a slight enlargement of the thyroid gland with its normal function has practically no effect on the functioning of other organs and systems. In the vast majority of cases, in conditions of mild to moderate iodine deficiency, a slight enlargement of the thyroid gland is detected only with a targeted examination.
In conditions of severe iodine deficiency, goiter can reach gigantic sizes. Also, against the background of DEZ, nodular goiter may subsequently develop, including those with autonomously functioning nodes.
Treatment of DEZ
Measures to eliminate iodine deficiency in the USSR were taken thanks to epidemiological studies begun before World War II by the outstanding endocrinologist surgeon and prevention specialist O. V. Nikolaev. They included the mass production of iodized table salt, the use of iodine tablets among risk groups, and the creation of goiter dispensaries. Against the backdrop of this program, iodine deficiency in Russia was largely overcome in the period from 1955 to 1970. After this happened, as a sign of “victory over ECD,” it was decided to gradually curtail measures to eliminate it, and the diagnosis of “endemic goiter” replace with “hyperplasia of the thyroid gland.”
In Western Europe, until the 60s of the last century, preparations of thyroid gland extracts were used, the effectiveness of which was determined not only by the content of thyroid hormones, but also by a large amount of iodine.
Today, there are three options for conservative treatment of DEZ:
- monotherapy with levothyroxine,
- monotherapy with iodine preparations,
- combination therapy with iodine and levothyroxine.
Monotherapy with levothyroxine has been scientifically substantiated in the treatment of ECD by describing the regulation of the thyroid gland by the hypothalamic-pituitary system. In an experiment on rats, it was shown that artificially simulated severe iodine deficiency leads to an increase in the level of TSH, which, in turn (as well as exogenously administered TSH), can lead to the formation of goiter. It was assumed that under conditions of iodine deficiency, the synthesis and secretion of thyroxine T4 and T3, for which iodine is the main structural component, are reduced, which, according to the principle of negative feedback, leads to increased secretion of TSH. Therefore, the main goal of levothyroxine therapy was to suppress TSH, which contributes to an increase in thyroid volume (suppressive therapy). However, it has been repeatedly shown that the decrease in gland volume does not depend on the degree of TSH suppression. There are also studies showing that the average TSH level in iodine-deficient areas is significantly lower than in those areas where iodine intake is normal. Moreover, there is experimental data demonstrating that the administration of TSH cannot stimulate the growth of follicles containing a sufficient amount of iodine.
As mentioned above, the administration of levothyroxine has been widely used for the treatment of ECD in the past. At the same time, excellent results were achieved at the initial stage. Many clinical studies have shown that after only 3-4 months from the start of therapy, there was a significant (at least 20%) decrease in the volume of the gland. The literature provides data on the effectiveness of using various doses and combinations of thyroid hormones. So T3 at a dose of 50 mcg per day is most effective for reducing the volume of the thyroid gland. Further options follow as efficiency decreases:
- (T4 50 mcg + T3 12.5 mcg) twice daily;
- T4 150 mcg per day + iodine 150 mcg per day;
- T4 75 mcg per day + T3 18.75 mcg per day;
- T4 200 mcg per day;
- T3 37.5 mcg per day.
The doses most often used in clinical practice are 150 mcg in adults and 100 mcg in adolescents. However, numerous studies have clearly demonstrated the “withdrawal phenomenon” - an increase in the size of the thyroid gland almost to the initial level a short time after stopping treatment. This phenomenon is explained primarily by the fact that when TSH is suppressed, the activity of the Na+/I–symporter decreases, and consequently, the active uptake of iodine by the thyroid gland decreases. Against the background of a sharp drop in intrathyroidal iodine content when the drug is discontinued, new growth of the gland occurs. Also, side effects of thyroid hormone therapy include the possible occurrence of drug-induced thyrotoxicosis, tachyarrhythmia, and osteoporosis, which limits the use of this group of drugs in long-term treatment of ECD. However, sometimes, in order to quickly achieve a therapeutic effect, they resort to prescribing a short-term course of treatment with levothyroxine with a further transition to maintenance therapy with iodine preparations.
Monotherapy with iodine preparations is etiotropic therapy. Work over the past 10–15 years has shown that an increase in TSH production or an increase in the sensitivity of thyrocytes to it is only of secondary importance in the pathogenesis of iodine deficiency goiter. With insufficient iodine intake into the gland, the amount of iodinated lipids (the main inhibitors of growth factors) decreases, which has a powerful stimulating effect on the growth of thyrocytes.
The main role is given to local ARFs, such as IRF-1, ERF and FRF.
The stage of “revival” of DEZ therapy with iodine began in the 80s of the last century. Many studies were limited by the fact that ultrasound measurement of the size of the thyroid gland could not be performed at that time. Thus, G. Hintze and D. Emrich in 1983, in their work devoted to the treatment of iodine deficiency goiter, used the neck circumference as the main marker of changes in the volume of the thyroid gland. The authors showed that the administration of 400 mcg of iodine is also effective in reducing the volume of the thyroid gland, as is 150 mcg of levothyroxine (assessed 12 months after the start of treatment), and, unlike levothyroxine, the result of iodine therapy persists for a long time after its discontinuation .
With the increasing introduction of ultrasound into practical medicine, randomized controlled studies are beginning to be conducted on the effect of various treatment regimens on the course of iodine deficiency goiter. At the same time, iodine doses ranged from 100 mcg and higher, including pharmacological ones, in the case of using iodized oil. The administration of 100–150 mcg of iodine has proven itself in the treatment of goiter in children.
In adults, iodine at a dose of 100–150 mcg per day was not as effective as in children, but a tendency to a decrease in the volume of the thyroid gland is also observed. In the scientific literature of the 80s of the XX century. You can find works where iodine was used to treat goiter in doses of 500 mcg, 400 mcg, and 300 mcg per day. And all of them demonstrate comparable effectiveness of iodine monotherapy with levothyroxine monotherapy and combination therapy with iodine and levothyroxine, as well as the most persistent effect after drug withdrawal. However, there is evidence that the use of high doses of iodine sometimes causes thyroid dysfunction (hypo- or hyperthyroidism). And although more significant evidence is needed to recognize this fact, the following position is currently generally accepted: therapeutic doses of iodine for ECD are almost no different from preventive ones and amount to 150–200 mcg per day. Thus, in a double-blind, placebo-controlled study in Germany, the effectiveness of 200 mcg of iodine for the treatment of iodine deficiency goiter was confirmed. The volume of the thyroid gland decreased by 38% over 6 months and remained this way for at least the same time. Another study assessed the effect of 200 mcg iodine and 100 mcg levothyroxine on gland size. Comparable efficacy was shown between the two dosages, with further emphasis on the fact that the degree of thyroid volume reduction was independent of TSH levels.
Numerous recent studies have demonstrated success in reducing the prevalence of goiter through the implementation of universal salt iodization programs. As for group prevention, 150 mcg of iodine per day is now sufficient for adolescents, and 200 mcg for pregnant and lactating women.
In the scientific literature of recent years, the issue of the development of autoimmune processes in the thyroid gland while taking iodine-containing drugs has been widely discussed. At the same time, there are works both confirming this influence and denying it. G. Kahaly in his works studied the effectiveness and safety of low doses of iodine for ECD. He noted that when using 200 mcg of iodine per day, an increase in the level of antibodies to thyroid peroxidase, antibodies to thyroglobulin, and a significant increase in lymphocytic infiltration in the gland tissue occur only in 97% of cases. In contrast to these facts, a group of researchers from Austria did not find the above-described changes at all when prescribing 200 mg of iodine to patients with iodine deficiency goiter. In general, the development of autoimmune processes in the thyroid gland most likely depends on the population characteristics of the region, which requires more detailed, carefully planned studies.
Combination therapy with iodine and levothyroxine can be carried out either by simultaneous administration of levothyroxine and potassium iodide, or by using their fixed combinations. Among them, the most commonly used drugs contain 100 mcg of levothyroxine and 100 mcg of iodide (iodothyrox). Iodotirox therapy has been repeatedly shown to have a number of benefits.
Firstly, by influencing several pathogenetic mechanisms of goiter formation, both hypertrophy and hyperplasia of thyrocytes are suppressed. This makes it possible to achieve results comparable in effectiveness to levothyroxine monotherapy (with a much lower content), which, in turn, reduces the number of side effects associated with taking thyroid drugs.
Secondly, the tendency to develop a “withdrawal phenomenon” during a short break in treatment is also reduced.
Thirdly, the suppression of TSH levels is less pronounced, for example, compared to the effect of levothyroxine at a dose of 150 mcg.
- The reduction in goiter volume is more pronounced with combination therapy (40%) than with levothyroxine monotherapy (24%) (Schumm et al.).
- The frequency of side effects of levothyroxine and potassium iodide is lower (since lower dosages are used than with monotherapy).
- The effect (reduction of goiter) develops faster than with potassium iodide monotherapy.
- There is no need to titrate the dose of levothyroxine, since the ratio of active ingredients is optimal.
There is a lot of work confirming these benefits. One of them compared the treatment of DEZ in 74 randomly selected patients. Patients received either 150 mcg levothyroxine or 100 mcg levothyroxine + 100 mcg iodine for 6 months. During combination therapy, the decrease in gland volume was somewhat more pronounced (30% compared to 25%, the difference is not significant). The reduction in gland size did not depend on the degree of TSH suppression. In addition, in the group of patients receiving combination treatment, it was subsequently possible to maintain a reduced gland volume with replacement therapy of 100 mcg of iodine daily. In the group of patients treated only with levothyroxine, such prophylactic treatment was less effective. The second study included 82 patients who were randomly prescribed either 100 mcg of levothyroxine or 100 mcg of levothyroxine + 100 mcg of iodine for therapeutic purposes for 6 months. The decrease in gland volume with levothyroxine was 24% compared to 40% with the combination of drugs; the differences were statistically significant. Thus, in adult patients, the combination of levothyroxine plus iodine is a preferable treatment compared to iodine monotherapy (at least in the same doses) and is comparable to a similar dose of levothyroxine. Many researchers note that 150 mcg of iodine in combination with an individually selected dose of levothyroxine at a rate of 1 mcg/kg body weight is more preferable for the treatment of endemic goiter in adults.
Summarizing the above, we can conclude that the main goal in the treatment of iodine deficiency goiter is not only to reduce the volume of the thyroid gland, but also to maintain the achieved result. For this purpose, iodine preparations are suitable both in the form of monotherapy and as part of combination therapy with levothyroxine.
The question remains what to prescribe first. It is obvious that the intrathyroidal iodine concentration increases significantly more during the initial intake of iodine preparations than when taking drugs combined with levothyroxine. This fact once again confirms the etiotropic nature of iodine therapy, as well as the advisability of starting treatment with the prescription of iodine preparations.
In our opinion, the treatment algorithm for DEZ can be presented as follows.
- For the treatment of children with ECD, potassium iodide is recommended at a dose of 100-150 mcg per day, for adolescents - at a dose of 150-200 mcg per day.
- Treatment of adults should be carried out at a young age (up to 45–50 years), since this is more likely to achieve the desired result, and there is also a low risk of having functional autonomy of the thyroid gland, in which iodine intake can provoke thyrotoxicosis. In the first 6 months, taking 200 mcg of potassium iodide per day is justified.
Persons with ECD over 45–50 years of age are advised to undergo active dynamic surveillance with annual determination of TSH levels and ultrasound examination of the thyroid gland.
- If there is no significant effect from taking iodine preparations, after 6 months a switch to combination therapy may be recommended. In this case, preference should be given to either a fixed combination of 100 mcg of iodine and 100 mcg of levothyroxine (iodothyrox), or an individually selected dose of levothyroxine at the rate of 1 mcg/kg of body weight in combination with 150 mcg of iodine per day.
But, based on modern ideas, no matter what initial treatment of goiter is carried out, its abrupt cessation cannot be recommended without further preventive measures - the use of iodized salt.
Literature
- Gerasimov G. A., Fadeev V. V., Sviridenko N. Yu., Melnichenko G. A., Dedov I. I. Iodine deficiency diseases in Russia. M., 2002.
- Gartner R., Dugrillon A., Bechtner G. Evidence that iodolactones are the mediators of growth inhibition by iodine on the thyroid // Acta Med Austriaca. 1996; 23(1–2): 47–51.
- Knudsen N., Bulow I., Laurberg P., Ovesen L., Perrild H. Low socio-economic status and familial occurrence of goitre are associated with a high prevalence of goitre // Eur J Epidemiol. 2003; 18(2): 175–81.
- Kohn LD, Shimura H., Shimura Y., Hidaka A., Giuliani C., Napolitano G., Ohmori M., Laglia G., Saji M. The thyrotropin receptor// Vitam Horm. 1995; 50: 287–384.
- Edmonds C. Treatment of sporadic goitre with thyroxine // Clin. Endocrinol. 1992; 36(1): 21–23.
- Einenkel D., Bauch KH, Benker G. Treatment of juvenile goitre with levothyroxine, iodide or a combination of both: the value of ultrasound grey-scale analysis// Acta Endocrinol. 1992; 127(4): 301–306.
- Hintze G., Emrich D., Koebberling J. Treatment of endemic goitre due to iodine deficiency with iodine, levothyroxine or both: results of a multicentre trial. //Eur. J. Clin. Invest. 1989; 19(6): 527 – 534.
- Leisner B., Henrich B., Knorr D., Kantlehner R. Effect of iodide treatment on iodine concentration and volume of endemic non-toxic goitre in childhood// Acta Endocrinol. 1985; 108(1): 44–50.
- Feldkamp J., Seppel T., Becker A., Klisch A., Schlaghecke R., Goretzki PE, Roher HD Iodide or L-thyroxine to prevent recurrent goiter in an iodine-deficient area: prospective sonographic study// World J Surg. 1997; 21(1): 10–14.
- Wilders-Truschnig MM, Warnkross H., Leb G. The effect of treatment with levothyroxine or iodine on thyroid size and thyroid growth stimulating immunoglobulins in endemic goiter patients // Clin Endocrinol (Oxf). 1993; 39(3):281–286.
- Papanastasiou L., Alevizaki M., Piperingos G., Mantzos E., Tseleni-Balafouta S., Koutras DA The effect of iodine administration on the development of thyroid autoimmunity in patients with nontoxic goiter// Thyroid. 2000; 10(6): 493–7.
- Kahaly GJ, Dienes HP, Beyer J., Hommel G. Iodide induces thyroid autoimmunity in patients with endemic goitre: a randomized, double-blind, placebo-controlled trial // Eur J Endocrinol. 1998; 139(3): 290–297.
- Pfannenstiel P. Therapie der endemischen Struma mit Levothyroxin und Jodid. Ergebnisse einer multizentrischen Studie // Deutsche Med. Wochenschr. 1988; 113(9): 326–331.
- Saller B., Hoermann R., Ritter M., Morell R., Kreisig T., Mann K. Course of thryroid iodine concentration during treatment of endemic goiter with iodine or combination of iodine or levothyroxine // Acta endocrinologica. 1991; 125:662–667.
E. A. Troshina , Doctor of Medical Sciences N. V. Galkina ERC RAMS, Moscow
Autoimmune Hashimoto's thyroiditis
It develops if a person has a congenital predisposition to pathologies of the immune system at the gene level. Hashimoto's thyroiditis is characterized by mutations that affect antibody production. The immune system begins to perceive thyroid cells as foreign and dangerous to the body. It produces special proteins - antibodies, which act on the thyroid gland and disrupt its functioning. This form of pathology has a protracted, chronic course and can be a lifelong condition.
Causes of chronic autoimmune thyroiditis:
- Excess iodine in the body (mainly due to diet).
- Herpes.
- Deficiency of vitamins and minerals, primarily selenium.
If we are not talking about diffuse goiter, when the entire organ is enlarged, then classification by localization is applied:
- Unilateral – neoplasms on one side.
- Double-sided - on both sides.
In women, Hashimoto's thyroiditis is up to 10-20 times more common. The average age of patients is from 40 to 50 years, but younger people are increasingly becoming ill.
Symptoms of Hashimoto's chronic thyroiditis appear due to decreased activity of the organ (hypothyroidism). Among the main ones:
- Loss of energy, constant drowsiness.
- Unreasonable weight gain.
- Bad mood.
- Coldness of the body.
- Hair loss, even baldness.
- Stool disorders.
- Growth of the gland in size, but without pain.
- An increase in the interval between menstruation, up to their cessation, is a characteristic symptom of chronic thyroiditis of the thyroid gland in women.
Help to make a diagnosis:
- Laboratory tests - a symptom of Hashimoto's thyroiditis is an increase in the level of T3 and T4 when inflammation has just begun, and later their production decreases, but the amount of TSH in the blood increases.
- The appearance in the blood of specific antibodies to thyroid cells.
- Ultrasound.
- Scintigraphy (if necessary, as an additional examination).
Treatment of a chronic inflammatory process of the autoimmune type is aimed at normalizing the functioning of the gland and treating hypothyroidism. Hormonal therapy is used for this. The dosage is individual in each case. Proper selection of medications restores the normal quality of life of patients or significantly slows down the rate of progression of the disease.
Reasons for development
Euthyroidism can be considered one of the most insidious diseases of the thyroid gland. It cannot be diagnosed immediately, hormone levels are always normal, and more dangerous diseases have already begun to develop.
The main causes of thyroid euthyroidism include the following:
- processes in the body associated with improper functioning of the immune system;
- unfavorable environment;
- heredity;
- thyroid diseases associated with the inflammatory process.
Acute thyroiditis
Develops against the background of infection by bacteria or viruses. Often a complication from ENT infections: sinusitis, tonsillitis and others. The causative agent of purulent inflammation can be any infectious bacterium, but mainly these are such common microorganisms as streptococci, Klebsiella, and enterobacteria.
Acute inflammation of a non-purulent nature can appear after bruises of the neck in the area of the thyroid gland following radiation therapy.
Symptoms of acute thyroiditis of the thyroid gland:
- Swelling of the neck.
- Increased temperature up to fever.
- Sore throat that gets worse when swallowing or moving your neck.
- Change in voice - hoarseness and wheezing appear due to compression of the vocal cords.
- A general weakened state, when fatigue appears even after minor physical exertion. Active movements are accompanied by rapid heartbeat and weakness.
- Tissue abscess in advanced form.
A characteristic feature of this type of thyroiditis is the rapid increase in the intensity of symptoms.
The following will help confirm the diagnosis:
- Tests - assessment of the amount of thyroid hormones (in acute cases, their production will be normal), ESR, leukocytes in the blood.
- Ultrasound of the thyroid gland is used as an additional examination in a number of cases.
- A puncture from the affected area is necessary if an abscess has developed or a course of antibiotics has not helped. The analysis will show the type of pathogens and their sensitivity to a particular group of antibiotics.
Acute inflammation is treated with antibiotics. If there is an abscess, the affected part must be removed surgically to avoid complications.
Diagnostics
First, the doctor examines the patient, asks him about his complaints and the course of the disease. Then he begins to examine the area where the thyroid gland is located and palpate. He can find that its size is increased or decreased, as well as detect nodules, compactions or softening of tissue. Manifestations of thyroiditis are not specific. To establish the shape and type of flow, laboratory and instrumental studies should be carried out.
To establish this diagnosis, examinations are carried out according to the following program:
- In acute thyroiditis: in the results of a general blood test, a picture of inflammation is observed: increased ESR, neutrophilic leukocytosis. In subacute thyroiditis: increased ESR and lymphocytosis.
- It is necessary to examine the level of thyroid hormones: TSH, free T3, T4.
- The level of thyroglobulin and the presence of antibodies to thyroperoxidase and antibodies to TG are determined.
- Ultrasound of the thyroid gland examines the tissue structure. A structural disorder, the presence of foci of inflammation are detected, and the size of the organ is determined.
- Scintigraphy clarifies the size of the lesions.
A biopsy of the thyroid gland followed by microscopic examination of cellular structures allows an accurate diagnosis to be made for autoimmune forms of the disease.
Subacute thyroiditis
The causes of this type of thyroiditis are a specific reaction to infections: measles, mumps, influenza and ARVI. The virus destroys the follicles of the gland, destroys the integrity of their membranes, and the hormones that enter the blood lead to the appearance of specific symptoms. Usually, from the moment of recovery until noticeable signs of problems with the thyroid gland appear, several weeks (or even months) pass.
The disease is often called de Quervain's thyroiditis or giant cell granulomatous thyroiditis.
In women, symptoms of thyroiditis and the disease itself are 5-6 times more common. The disease may begin with symptoms that resemble hyperthyroidism with increased levels of thyroid hormones:
- Rapid heartbeat.
- Body tremors (usually hands).
- Nervousness, irritability.
- Increased sweating.
- Lose weight without changes in diet and exercise.
- Digestive and stool disorders.
- Increased pressure.
- Muscle weakness and soreness, joint pain.
- Loss of appetite.
- Sleep disorders.
- Headache attacks.
There are also typical external manifestations associated with an enlarged gland:
- Enlarged goiter on the neck, swelling, redness of the skin.
- Sharp pain in the thyroid area when pressing on it or bending the neck.
- Feeling of a “lump” in the throat, difficulty swallowing.
The acute stage lasts 1-2 months.
To make a diagnosis the following are used:
- Blood test - characteristic results: the level of hormones T3 and T4 is higher than normal, and TSH is lower. Significantly higher than the ESR norm.
- Ultrasound - to identify the number of affected areas and assess blood circulation in them.
- Scintigraphy - assessment of the absorption of iodine radioisotopes by the gland and biopsy.
In many cases, the inflammation goes away on its own. This is based on the fact that excess hormones reduce the activity of the hypothalamus and the production of its hormone thyrotropin. This is a hormone that regulates the functioning of the thyroid gland, which means that its decrease in the body leads to a decrease in the activity of the thyroid gland. This process of self-regulation will take about two months (although relapses are possible), and therapy during this time is aimed at reducing pain and discomfort in the patient. Nonsteroidal anti-inflammatory drugs will help; in severe cases, corticosteroids or beta blockers. Your doctor may also prescribe hormone replacement therapy. Recipes, dosage, frequency and duration of administration are individual.
Symptoms
People are often surprised by the diagnosis of euthyroidism. Only ultrasound and some additional studies show that they have this disease. However, there are a number of symptoms that are an indicator that there is something wrong with the thyroid gland, even if the hormone test is normal.
These symptoms include:
- excessive, sometimes groundless nervousness;
- fast fatiguability;
- small swelling in the neck area;
- sometimes there is difficulty swallowing, a lump is felt in the throat;
- upon palpation, the doctor may detect small nodular formations in the neck area; They are mostly painless, and only occasionally do patients complain of discomfort, for example, when the neck is compressed by a clothing collar.
Chronic thyroiditis
Another name for this form of inflammation is Riedel's thyroiditis. This is the least studied type of disease.
Among its main causes, systemic immune malfunctions are suspected, which increase the activity of plasma cells. This causes the gland cells to die, leaving fibrous areas. The likelihood of getting the disease is higher in people with Graves' disease or endemic goiter (even in the past).
Symptoms of chronic thyroiditis of the thyroid gland will rarely be noticeable at the very beginning of the disease. Because of this, time is wasted when conservative therapy is effective. As the disease progresses, the patient experiences symptoms that resemble cancer. They are caused by the rapid growth of the organ:
- "Lump in the throat.
- Difficulty breathing, suffocation.
- Long cough, hoarseness in the voice.
There is no pain when pressing on the gland.
To diagnose Riedel's thyroiditis, the following are used:
- A blood test - which is characterized by the following indicators: there are anti-TPO antibodies, the TSH level is elevated in 30% of cases, and in the remaining 70% - hormonal levels are normal.
- Cytological examination of tissues from puncture. It helps to distinguish cancer from fibrous inflammation without malignancy of the tumor.
Examinations such as ultrasound diagnostics and even MRI are not very informative with Riedel's thyroiditis.
Therapy is aimed at preventing complications. If the tumor is too large and puts pressure on neighboring organs, it is partially (or completely) removed surgically. After surgery, hormone replacement therapy, drugs that suppress fibrosis in tissues, and drugs for autoimmune processes are carried out. At the initial stage, such conservative therapy often does not help - the tumor grows too quickly, so it is difficult to avoid surgery.
Treatment
In mild forms with normal thyroid function, they are limited to regular monitoring by an endocrinologist.
Treatment of acute thyroiditis is carried out with antibacterial drugs, taking into account sensitivity. Antihistamines (Loratadine, Clemastine and others) are used and detoxification therapy is carried out. In the presence of a formed abscess, surgical treatment is used. The disease acute thyroiditis is quite rare, but untimely diagnosis and improper treatment of this disease is very dangerous, because can lead to the spread of a purulent focus into the mediastinum and, unfortunately, lead to death.
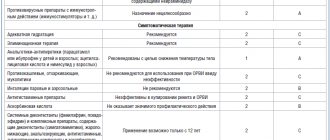
When treating subacute thyroiditis, glucocorticoid drugs are prescribed; severe disease requires hospitalization in a specialized endocrinology department. For severe pain, painkillers are recommended. In case of development of transient thyrotoxicosis, thyreostatics and adrenergic blockers are prescribed.
Treatment of chronic autoimmune thyroiditis depends on the stage of the disease, on the function of the thyroid gland, on the presence of structural changes and the volume of the thyroid gland. At different stages of the disease, thyreostatic drugs, iodine preparations, and thyroid hormones are prescribed. In case of severe compression of adjacent organs with disruption of their function, surgical treatment is performed. The choice of treatment method remains with the doctor; independent treatment is not acceptable, because may lead to unpredictable consequences.
You should seek help from an endocrinologist and strictly follow all his prescriptions.
Prevention of thyroiditis
A healthy lifestyle with:
- Sufficient intake of vitamins and minerals.
- Treatment of acute respiratory viral infections and infections, especially in the nasopharynx, other ENT organs and the oral cavity.
The prevention, diagnosis and treatment of these diseases is carried out by an endocrinologist, in some cases with the help of an immunologist.
You can undergo high-quality examinations in an express format at a medical clinic. Pre-registration is possible online or by calling the clinic.
At the Kutuzov Treatment and Diagnostic Center, you can undergo a full examination using high-precision equipment and determine the cause of the pathology. Modern treatment methods and unique proprietary developments allow our specialists to achieve excellent results. We value your time and offer doctor visits by appointment. Come to our center to undergo a thorough examination and receive an individual treatment plan for the identified pathology in comfortable conditions and at a convenient time. In addition, the doctor will give comprehensive recommendations on preventive measures that will help avoid the development of pathology in the future.
Diet and other aspects of nutrition
If it has been established that the cause of euthyroidism is hidden in iodine deficiency, then you can try to cope with the problem with the help of diet.
The menu should include products such as:
- Sea fish: hake, pollock, haddock, capelin, cod.
- Shrimps.
- Squid.
- Feijoa.
- Sea kale.
- Persimmon.
- Liver.
- Spinach.
- Eggs.
Most iodine can be obtained from fish, algae and seafood.
When a person develops obesity against the background of euthyroidism, it is necessary to adjust the diet so that it contributes to weight loss.
The following foods and drinks are excluded from the menu:
- Flour dishes.
- Fatty food.
- Smoked meats.
- Fast food.
- Alcohol.
- Confectionery and other sweets.
A person should eat food that is a source of fiber. Salads should be prepared from fresh vegetables. Be sure to supplement the diet with bran, cereals, and nuts. Among the cereals, oatmeal and buckwheat are considered especially healthy.
Nodular goiter is one of the forms of euthyroidism
According to medical statistics, in 4% of the population, when examined by an endocrinologist, small (1-1.5 cm) nodules are found in the neck area. They can be located one at a time (solitarily) or in groups. Most often, the patient pays attention to these formations when they become visually noticeable or when pain begins to be felt when swallowing. This disease is called “nodular goiter”. Euthyroidism of the thyroid gland is the main background of its manifestation, since the thyroid hormones T3, T4, TSH are almost always within acceptable values. If this pathology is detected, the doctor is obliged to prescribe additional examinations to the patient, including ultrasound, radioisotope analysis for thyroid hormones. In some cases, especially with a single node, a puncture biopsy and cytological examination of the sample taken is performed. If a nodular goiter grows too quickly or the patient consults a doctor when the tumor has reached a significant size, the doctor may prescribe an x-ray of the retrosternal area with the introduction of barium into the esophagus for a contrast assessment of the result.