Rectal fistula, or chronic paraproctitis, is a chronic purulent inflammation of the peri-rectal tissue associated with the penetration of infection from the rectum. Rectal fistulas are one of the most common causes of fecal incontinence. The search for safe and effective treatments for this disease continues to this day.
What treatment methods do we use:
- Excision of a fistula using the radio wave method using the Surgitron apparatus
- Closing the fistula with a biological prosthesis “Anal Fistula Plug”
- Innovative microsurgical LIFT method - without damaging the anal sphincter
- Operations with primary sphincter plastic surgery for fistulas with fecal incontinence
To make an appointment with a proctologist in Kyiv and Donetsk, call
(067) 753-03-03 and or online
Our practice in surgery of rectal fistulas is one of the most extensive in Ukraine. To date, experience has been accumulated in about 500 operations for chronic paraproctitis. Our results - only 2.8% of relapses of the disease and not a single case of fecal incontinence - are at the level of leading clinics in Europe and the USA. We have the first published experience in Ukraine of the newest LIFT operation, which allows for reliable and low-traumatic elimination of rectal fistulas and preserving the function of the anal sphincter.
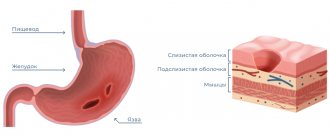
WHAT DOES A RECTAL FISTULA LOOK LIKE?
Externally, a rectal fistula looks like a small hole in the skin in the perineum or anus - this is the so-called external opening of the fistula. There may be thickening and redness of the skin around it. The fistulous tract (canal in inflamed tissues) begins in the rectum with an internal opening and ends on the skin. The fistula can pass superficially (only under the rectal mucosa), or spread through the muscles of the anal sphincter (transsphincteric and extrasphincteric fistulas). Such fistulas are especially dangerous and complex; they can have a tortuous, branched course, purulent accumulations in the tissues, and be accompanied by fecal incontinence.
To make it easier to understand information about fistulas, look at the article on the structure of the rectum.
What happens if the fistula is not treated?
If the fistula is not treated, then nothing good will end. The tooth will need to be removed, and what’s more, the bone surrounding the tooth suffers greatly, and the vestibular cortical plate suffers. When the tooth is not treated, when the cause of the fistula is not dealt with, the cortical plate is quite destroyed. Large cavities are formed in the bone, as exudate is formed, all this rots and the bone decomposes, softens and becomes infected, lyses, and exits through the fistulous tract.
Therefore, in addition to, as I said earlier, there is a fairly strong load on the body, since a fistula is a constant open source of infection in the oral cavity.
SYMPTOMS OF RECTAL FISTULA
Characteristic signs of a rectal fistula are pain in the anus , mucous, sanguineous and purulent discharge (the patient often has to wear a pad), itching in the anus . During the period of exacerbation of the disease, the pain intensifies, and the body temperature may rise. With rectal fistulas, a frequent outcome is relapse (repetition) of acute paraproctitis - if the patient does not receive special treatment. Some patients with fistulas are operated on for acute paraproctitis many times until the connection between the rectum and surrounding tissues is eliminated with radical surgery in a specialized proctology clinic.
Anesthesia
For surgical interventions in the perineal area, regional anesthesia is currently used. It includes subarachnoid (spinal) anesthesia at the lumbosacral level, which allows you to block the transmission of sensory and painful nerve impulses to the lower part of the body, including the anorectal area. In this case, the motor function of the lower extremities is not lost. Subarachnoid anesthesia is a fairly safe method and has a low risk of complications from the heart, respiratory system and nervous system. During the operation, for maximum comfort, the patient is conscious or in a state of medicated sleep (sedation). General anesthesia in anorectal surgery is used in individual cases at the discretion of the anesthesiologist-resuscitator.
DIAGNOSIS OF RECTAL FISTULA
The diagnosis of rectal fistula is easy to make - most often the doctor simply needs to examine and digitally examine the rectum. To clarify the details, it is always necessary to examine the rectum using a special device - sigmoidoscopy, anoscopy . During the examination, the doctor also examines the course of the fistula canal using a probe , and injects a special dye into the fistula to detect its internal opening. In cases of complex rectal fistulas, additional examinations are often necessary - ultrasound, magnetic resonance imaging (MRI).
For the first time in Donetsk, we are widely introducing magnetic resonance imaging into practice in the refined diagnosis of complex fistulas. This highly informative study allows you to literally “plot the route” along which the surgeon will work during the operation, being able to completely remove all fistulous tracts and avoid damage to important structures of the rectum.
Treatment methods for paraproctitis
Complete cure is only possible through surgery. Physical therapy, antibiotics, and ointments are used in preparation for or after surgery. Drug therapy can also relieve symptoms and speed recovery. Main recommended pharmacological groups:
- painkillers;
- systemic antibiotics;
- healing ointments.
A course of physiotherapy may include ultraviolet irradiation and electrophoresis.
SM-Clinic specialists diagnose and treat complex pathologies. To make a diagnosis, the doctor collects the patient’s complaints, medical history and objective examination. To clarify the diagnosis and carry out differential diagnosis, additional instrumental studies are performed, such as anoscopy and sigmoidoscopy. These studies are carried out after cleansing the intestines by performing cleansing enemas and taking laxatives.
TREATMENT OF RECTAL FISTULA
Treatment of rectal fistula is surgical only . Non-surgical treatment of fistulas with the help of a special biological glue has not been justified, since it results in up to 90% of relapses.
Surgery for rectal fistula is a complex surgical task that can only be successfully solved in a specialized hospital that has a wide variety of methods and modern equipment.
A huge number of different surgical operations have been proposed to eliminate rectal fistulas. All of them are fundamentally aimed at achieving two goals - complete elimination of the fistula , its internal and external openings, and preservation of the function of fecal retention . The most common and successful technique is Gabriel's operation , or fistulotomy - when the fistula is widely dissected along its entire length, and a wound is formed in the shape of a triangle, with its apex facing the rectum. Such a wound remains open and gradually heals from the inside out. To prevent its edges from sticking together and the fistula from forming again, regular medical supervision and dressings are needed. Currently, we perform this operation using a special device - "Surgitron" - a radio wave scalpel, this significantly reduces postoperative pain and shortens the wound healing time.
Another popular method is plastic surgery to close the fistula using a rectal tissue flap . It is performed mainly for complex fistulas. Modern foreign studies show too high a percentage of relapses (recurrences of the disease) during such operations, which forces them to limit their use. We practically abandoned this method several years ago.
About 5 years ago, modern microsurgical techniques appeared, such as the LIFT operation (ligation of a fistula in the intersphincteric space) , which makes it possible to guarantee the preservation of the function of the anal sphincter and reliably eliminate the fistula - its long-term results are very encouraging, although they are under study. To perform this operation, one very small (no more than 1-2 cm) incision is made on the outside of the anus, through which, with the help of special instruments, it is possible to isolate, cross and sew up the fistula tract at its very beginning, in the area where the anal glands are located. This eliminates the primary source of infection. The muscles of the anus remain unaffected.
In 2010, for the first time in Ukraine, we performed and published the results of LIFT operations ; we made reports at the III Congress of Coloproctologists of Central and Eastern Europe, as well as at a meeting of the Association of Surgeons of the Donetsk Region. To date, we have experience of more than 30 such interventions - all patients are completely cured and have no problems with fecal continence.
For particularly complex rectal fistulas, with a high risk of developing fecal incontinence, a revolutionary method is successfully used - closing the fistula using a special biological collagen “plug” - the so-called Anal Fistula Plug obturator, manufactured in the USA. This “plug” has the shape of a thin and long flexible cone, and is made of special collagen fibers. The collagen fibers of the obturator stimulate the rapid growth of its own connective tissue, which is necessary for the healing of the fistula. During surgery, the Anal Fistula Plug is inserted through the internal opening of the fistula and secured with sutures. Swelling, the plug tightly blocks the lumen of the fistula, and in a few weeks it completely grows with the body’s own tissues. After some time, it is no longer possible to detect the fibers of the obturator itself.
Now treatment of rectal fistula in Donetsk has become available to you using the latest world developments introduced by us. Remember that chronic paraproctitis is one of the most serious diseases of the rectum, which, if not treated in a timely manner, leaves behind severe complications such as fecal incontinence. Don't put off visiting your doctor. If you have questions, ask them in the box below:
Symptoms and manifestations of pathology
Pararectal fistula symptoms are pronounced, the clinical picture is characterized by wave-like symptoms, alternating stages of exacerbation and remission. Depending on the stage, the symptoms of the disease are as follows:
- the presence of a wound (fistula tract) in the perianal area;
- rectal discharge (purulent, serous-purulent, sanguineous), noticeable on underwear;
- unpleasant odor of discharge;
- hyperemia of the skin around the anus, itching, burning;
- dull pain in the rectum, intensifying during bowel movements and receding after defecation due to the outflow of purulent exudate;
- a significant increase in pain during exacerbation (the appearance of an abscess in the perirectal tissue) - in the pelvis, rectum, lower abdomen, especially during bowel movements, walking, coughing;
- disturbances of urination and fecal excretion;
- temperature increase;
- signs of intoxication;
- headache;
- weakness, decreased motor activity.
After opening the fistula, remission occurs, but the wound does not heal, since the inflammatory process does not stop, the formation and outflow of exudate continues, as a result of which the patient’s sleep is disturbed, loss of performance, and disorder of sexual functions and nervous system occur.
With the development of a transphincteric fistula, the following symptoms are observed during a hardware examination of the patient:
- deformation of the anal canal;
- dysfunction of the sphincter;
- scarring of the sphincter muscles;
- disruption of the process of defecation up to fecal incontinence.
Despite the severity of the clinical picture, an incomprehensible shyness keeps some patients from turning to professional doctors. Self-medication is carried out with local drugs, although in case of perirectal fistula, treatment without surgery does not give a lasting effect and can lead to serious complications.
Relapses of the disease
As mentioned above, complex forms of fistulas, as well as repeated cases of the disease, localization of the fistula, the presence of leaks, cavities, additional fistula tracts are risk factors for the development of relapses in the future. Previous inflammatory diseases of the anorectal area and surgical interventions contribute to the growth of connective scar tissue. Such tissue is more susceptible to various traumatic factors and infections. Recurrent forms of rectal fistula are quite difficult for surgical treatment and require maximum attention from a surgeon.
Successful treatment of rectal fistulas generally depends on many factors. Many years of experience of a coloproctologist, proctologist or surgeon, a specialized hospital with the ability to use modern diagnostic and treatment methods, as well as the patient’s full understanding of the seriousness of his disease and following the recommendations of the attending physician are the main things for the effective and safe treatment of rectal fistulas.
Ask a Question
Causes of a fistula on the gums in an adult
A fistula is formed due to an infectious purulent process in the dental canal. Pathology can occur for the following reasons:
- Deep caries and untimely treatment;
- Newly emerging periodontitis and periostitis with the formation of pus;
- Chronic periodontitis, damage to the walls of the tooth root;
- Cystic formations;
- Oncology;
- Pulpitis, damage to the tooth root;
- Granuloma.
Fistula also occurs after tooth extraction. This is a common pathology that occurs as a result of infection in the wound.
A fistula after dental treatment can form, for example, due to infection as a result of errors in the treatment of caries. Improper filling of a tooth can also lead to the development of pathology. In this case, a tooth root fistula is formed when pus, having passed through the dental canal, breaks into the surrounding tissue. The most common fistula of the upper and front teeth occurs.
Alcohol, smoking, stress, exacerbations of chronic diseases, abuse of carbohydrates, lack of nutrition, chronic diseases - all these factors increase the root causes of the disease.
How dangerous is a fistula? Consequences
The fistula itself does not pose a danger, since through it the pus is removed from the source of infection, and accordingly, the degree of tissue damage is reduced. But the presence of a fistula indicates that the process is serious, and various types of complications may arise, such as:
- Loss of teeth in the affected area;
- Attachment of a secondary infection - inflammation of the lymph nodes, ears;
- Sinusitis;
- Sinusitis;
- Damage to bone tissue;
- Sepsis as a result of infection entering the general circulatory system;
- The appearance of cystic formations at the roots of the tooth;
- Heart complications, bacterial endocarditis.
Sometimes it happens that the pus drains almost completely, the fistula heals, and the patient thinks that everything is gone. But in fact, the source of inflammation has not been eliminated, so relapse of the disease is inevitable. Repeated abscesses and fistulas are more difficult to treat.
Postoperative care
In the postoperative period, all patients must undergo local and general anesthesia. Local anesthesia includes ointments and suppositories, which can locally reduce the severity of pain. Tablets, capsules, intravenous drugs are classified as general anesthesia. If the pain is significant, potent drugs (narcotic analgesics) are also used in a hospital setting. Your doctor will tell you the regimen for using painkillers, methods of administration, and specific names of drugs.
The average hospital stay is 1-5 days. It depends on the extent of the operation, the presence of complications and some other individual characteristics. During the postoperative period, you will undergo daily dressing changes and monitoring of wound healing. Antibacterial therapy is not indicated for all patients, but only if there are indications determined by the doctor. Mandatory wound care includes washing it with a stream of water at room temperature 3-4 times a day. This facilitates mechanical cleaning and will reduce the risk of infectious complications. The doctor will also show you how to properly perform dressings so that you can do them yourself at home.
Prevention of fistulas
The main measure for preventing fistulas is maintaining oral hygiene. It is necessary to undergo an annual examination by a dentist and, if necessary, begin treatment for caries and periodontitis in order to prevent the development of chronic diseases.
It is also advisable to be treated by experienced, qualified dentists, since poor-quality services can also lead to the formation of a fistula. After the intervention, you need to monitor your well-being to prevent the development of a fistula.
Is treatment possible at home?
A fistula can only be treated in a clinic. But if it is impossible to urgently visit the dentist, for example, the pain occurred at night, it is recommended to rinse the mouth with the following means:
- infusion of chamomile;
- infusion of oak bark (dry raw materials can be purchased at a pharmacy);
- if there is purulent discharge, the mouth should be rinsed with a solution of salt and soda or antibacterial agents.
The described measures help relieve pain, but do not eliminate the cause of the disease. Therefore, in any case, you need to see a dentist.