Structure
The tricuspid valve, according to the scientific literature, is also called tricuspid. When the heart moves, all processes occur synchronously. If a blockage occurs in one of the departments, a minor temporary one, the body immediately senses that the condition changes significantly. The state of health immediately worsens, it becomes difficult to breathe and it is impossible to move.
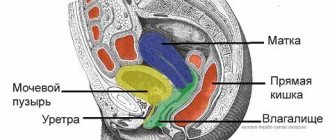
The tricuspid valve is located on the left side of the sternum. It is part of the pumping system for pumping blood. It is a kind of cap that opens under the pressure of ejected blood. Closing occurs due to the reverse forces of the liquid automatically due to pressure on the surface of the valves.
Incomplete closure of the tricuspid valve occurs due to relaxation of the heart muscle, when it is no longer able to function normally. Due to a violation of the redistribution of internal pressures, tissues begin to break down, which as a result threatens the formation of heart disease. Some diseases become provocateurs of such pathology.
Work of the organ
The tricuspid valve is part of the human circulatory system. A huge amount of blood flows from the outlets of the heart to the aorta, passing through all the arteries and capillaries, it exchanges oxygen with the cells and receives carbon dioxide. At the same time, it becomes saturated with decay products from processed beneficial microelements and becomes dark in color. This blood is called venous.
Next, redistribution occurs to the right region of the heart, further movement occurs through all arteries of the lung, for oxygen enrichment. The tricuspid valve is not the only one that has the ability to block reverse flow. This is necessary to separate the working together: left, right ventricles and atria.
Blood fills the left region of the heart, then from the atrium it flows into the ventricle. After this, circulation occurs in the systemic circulation. Venous blood returns to the right atrium, then to the right ventricle and exits into the pulmonary circulation. After oxygen saturation, the systemic cycle is repeated again through the left atrium and ventricle.
Prosthetics of the tricuspid valve, along with plastic surgery, is one of the surgical treatment options, which is used when it is impossible to preserve the valve due to gross changes in the leaflets and subvalvular apparatus. In recent years, in the domestic literature [1, 2], there has been a small number of studies devoted to the study of long-term results of tricuspid valve replacement. In this regard, we decided to present our experience on this problem. According to various authors [4-7, 10], tricuspid valve replacement has a high level of complications, and mortality remains within 20%.
Material and methods
From 2000 to 2009, 218 tricuspid valve replacement surgeries were performed in our center. In this work, data from 186 patients were analyzed. The main characteristics of the patients are presented in Table. 1
.
Systolic pressure in the pulmonary artery, according to sounding of the right side of the heart, in half of the patients exceeded 40 mm Hg.
Most patients were admitted for treatment with severe heart failure, with a mean NYHA functional class of 3.5 ± 0.7. 51% of patients already had persistent atrial fibrillation. Almost all patients had cardiomegaly due to the right side of the heart. 94 (51%) patients had undergone valve correction in the past, of which 67 (36%) had previously undergone closed mitral commissurotomy or mitral valve replacement. 27 (15%) patients had previously undergone intervention on the tricuspid valve, of which 13 (7%) had a recurrence of tricuspid insufficiency after previously performed repair, and 14 (8%) required re-replacement of the tricuspid valve due to degeneration of the bioprosthesis. All operations were performed according to standard methods. Cardiopulmonary bypass was performed through bicaval cannulation and cannulation of the ascending aorta. Until 2005, operations were performed under conditions of moderate hypothermia (32 °C); subsequently, under normothermia conditions. Cold blood cardioplegia was used in the majority of patients; pharmacocold cardioplegia with Custodiol solution was used in 9 (4.8%). The duration of artificial circulation and the time of aortic clamping were 118.9±48.8 and 93.8±41.8 minutes, respectively.
Isolated tricuspid valve replacement was performed in 43.5% of patients, the rest underwent two-valve (32.8%) and three-valve (23.7%) corrections. Moreover, the majority underwent mitral-tricuspid (52 cases) and mitral-aortic-tricuspid replacement - 41 (50%). Tricuspid valve replacement with a mechanical prosthesis Meding-2 was performed in 19 patients. Until 2006, KemKor xenoprostheses were mainly used (82 cases), since 2006, as a rule, Pericor pericardial prostheses began to be implanted (68); 9 patients were implanted with Perimount prostheses (Carpentier-Edwards Inc.), 8 with Bio-Lab prostheses.
results
In 37.6% of cases, patients required prolonged (more than 24 hours) artificial ventilation, in 38.7% - a long (more than 48 hours) stay in the intensive care unit, in 72% - inotropic support of varying duration. In the early postoperative period, 24.4% of patients suffered various complications. The most common complications were third degree atrioventricular block (9.1%), pericardial effusion (4.8%), infectious complications (4.9%) and postoperative bleeding (3.8%). Neurological disorders were recorded in 1.6% of patients. Mortality rate was 13.4%. The main causes of death were progressive cardiovascular failure (7%) and multiple organ failure (2.8%). Other causes include gastrointestinal bleeding (1.2%), acute respiratory failure, acute cerebrovascular accident, postoperative bleeding and generalized peritonitis (0.6% each). Prognostic factors associated with mortality were rheumatic genesis of tricuspid disease ( p
=0.017) and initial NYHA functional class (
p
=0.03).
Long-term results were studied in 126 patients over a period of 13 to 130 months (median - 43 months). The dynamics of the main echocardiographic parameters are presented in table. 2
.
After surgery, the size of the right parts of the heart decreased in patients (from 71.7±17.2 to 60.0±10.6 mm, p
<0.001) and right ventricular size (from 38.7±7.0 to 34.7±6.2 mm,
p
<0.001).
The functional class of heart failure decreased significantly (from 3.5 to 2.4, p
<0.001).
The need for implantation of a permanent pacemaker arose in 32.7% of those observed. 41.8% continued to require diuretics, most of them were patients with multivalve repair. On mechanical prostheses, in contrast to biological ones, a more pronounced peak gradient was observed (11.1 ± 4.8 mm Hg versus 8.1 ± 3.8 mm Hg, p
= 0.006).
Dysfunction of bioprostheses was detected in 8.2% of patients in the period from 50 to 117 months after surgery (median - 71 months). Thrombosis of the mechanical prosthesis was detected in 10.5% of patients (median follow-up period: 16 months). The need for tricuspid valve replacement occurred in 13.5% of patients. Mortality in the long-term period was 12.7%. In the majority of patients (81.3%), the causes of death were related to cardiac pathology. The figure
shows the actuarial curve for 10-year survival, which was 87.3% (95% CI 81.5–93.1) at 10 years.
Figure 1. Actuarial 10-year survival curve after tricuspid valve replacement.
Discussion
Our study included a heterogeneous group of patients who required tricuspid valve replacement. The rheumatic genesis of the defect predominated. The choice to replace rather than repair the valve was, as a rule, dictated not so much by the etiological essence of the defect as by the severity of organic changes in the valve. These were patients with heart failure of functional class III-IV. Patients with rheumatism had the highest number of two- and three-valve corrections. The severity of the initial condition of the patients was also evidenced by the fact that more than ⅓ of the patients needed prolonged artificial ventilation and a long stay in the intensive care unit. Implantation of a permanent pacemaker was required in 32.7% of patients due to acute postoperative third-degree block or the development in the long-term period of high-grade atrioventricular block and sick sinus syndrome. Thus, in total, various complications were observed in 57.1% of patients. Some authors [8] cite a lower frequency of need for pacemaker implantation. Other authors [4, 6, 7] present approximately similar data. Moreover, F. Filsoufi et al. [5] when treating 81 patients, certain complications were observed in all cases.
Among the factors associated with mortality, our study noted rheumatic origin of tricuspid valve disease, which is likely explained by several factors. Firstly, this is a long course of the disease and, as a result, more severe heart failure. Secondly, the frequent combination of rheumatic tricuspid disease with mitral or aortic disease and, accordingly, the combined nature of the operation. Despite this, our observation showed an improvement in echocardiographic parameters and a decrease in the severity of heart failure, which in most patients corresponded to NYHA functional class II.
The initial severity of heart failure is also a predictor of poor surgical outcome. Similar data are presented by Y. Topilsky et al. [9].
R.M. Muratov et al. [3] noted an earlier occurrence of dysfunction of bioprostheses when the subvalvular apparatus of the tricuspid valve was preserved.
Our study did not reveal such a pattern. We also found no differences in the need for reprosthetics between different types of bioprostheses ( p
=0.37). There is no complete agreement among surgeons regarding the priority in choosing the type of prosthesis. A number of researchers [11-13] do not note the advantages of bioprostheses over mechanical ones in the tricuspid position.
In other studies [1, 4, 14], on the contrary, it is recommended to use bioprostheses in the tricuspid position.
Our study has a number of limitations and limitations. First, this is a retrospective study, and it is not possible to draw any conclusions regarding the superiority of biological or mechanical prostheses. Secondly, the presented population is heterogeneous in terms of the etiology of the defect, which also has a great impact on long-term results. Thirdly, long-term results could not be studied in all patients.
conclusions
1. Patients undergoing tricuspid valve replacement constitute a high-risk group.
2. Prosthetics of the tricuspid valve in case of its organic changes is the optimal method of surgical treatment, although it is accompanied by an increased level of mortality and complications.
3. The development of dysfunction (thrombosis) of mechanical prostheses in the tricuspid position occurs at an earlier time in comparison with biological prostheses, which requires further study of the long-term results of the use of mechanical prostheses.
Valve functions
Since the left and right parts of the heart work synchronously, it is necessary to stop the return flow between the departments in a timely manner. After all, blood pumping occurs cyclically: there is a moment of fluid accumulation in the ventricle, followed by a powerful release of blood into the aorta. The valve system operates correctly:
- Located in the left region of the heart is called the mitral.
- Triscupidal.
- Valve in the artery of the lungs.
- Aortic, as a fuse for the largest system.
Doctors use the term regurgitation to describe the phenomenon of blood flowing backwards through the valves. To prevent this from happening, the listed blockers must be processed in a timely manner according to the following rules:
- The mitral valve is open only at the moment of pumping blood from the left atrium to the corresponding ventricle. It closes when accumulated fluid is released into the aorta. The valve structure has two leaflets.
- The tricuspid aortic valve closes the passage between the right atrium and the corresponding ventricle. Works similar to the mitral. The building has three doors.
- Pulmonary refers to the area between the pulmonary trunk and the right ventricle. Serves to block the reverse flow at the moment of relaxation of the heart muscle.
- The aortic is located in the outflow canal of the left ventricle. It blocks the reverse flow of blood from the aorta at the moment the heart muscle relaxes. Consists of three semilunar valves.
Methods of treating diseases
The tricuspid heart valve (located between the right atrium and the ventricle) is treated depending on the degree and stage of its damage, how extensively the pathological processes develop, and the area of their localization. During the period of therapy, it is important to strictly follow all the doctor’s recommendations, without exception, since the disease is life-threatening for the patient.
Drug therapy for damage to the tricuspid heart valve involves the use of the following drugs:
| Group of drugs | Name | Application |
| Diuretics | Britomar, Hydrochlorothiazide | Medicines reduce congestion in the patient’s body and remove excess fluid. The tablets are taken orally, regardless of food, and washed down with plenty of water. Adult patients are prescribed 10-20 mg once a day. If necessary, the dosage is increased to 20-40 mg. |
| Potassium preparations | Panangin, Asparkam | The drugs prevent the accumulation of excess fluid in the patient’s body. The medicine is taken orally 1-2 tablets 3 times a day after meals. The minimum course of therapy lasts 2-3 weeks. In severe situations, the medicine is administered intravenously through a drip. |
| Venous dilators | Corvaton, Nitrosorbide | The drugs reduce the load on the heart and help it accumulate a certain amount of blood. It is recommended to take the tablets at regular intervals and wash down 0.5 tbsp. water. Adult patients are prescribed 1 tablet 1-2 times a day. |
| Anticoagulants | Warfarex, Warfarin | The standard dosage of the drug is 5 mg 1-2 times a day. It is preferable to take the medicine before or after a meal. The course of therapy lasts 6-12 months. |
| Cardiac glycosides | Digoxin, Corglicon | The drugs help eliminate arrhythmia. The medicine should be taken before or after meals. Swallow the tablets whole and take them with plenty of liquid. Take the first dose in a volume of 0.5-1 mg, then every 6 hours at 0.25-0.75 mg for 2-3 days. The maintenance dosage is 0.125-0.5 mg 1-2 times a day. |
| Beta blockers | Diltiazem, Carvedilol | Medicines reduce the contraction of the left ventricle. Adult patients are prescribed 1 tablet 1-2 times a day. The drug is swallowed whole and washed down with a small amount of water. |
During specially selected therapy, patients should also follow the strict recommendations of the attending physician:
- Completely give up bad habits (alcohol, cigarettes).
- Always dress appropriately for the weather to prevent hypothermia or overheating.
- Avoid emotional situations, nervous tension, and severe stress.
- Follow a specially selected diet to reduce the load on a diseased heart.
- Reduce the intensity of physical activity.
Compliance with these recommendations will help not only achieve a positive result in treatment, but also prevent the occurrence of serious complications.
Development of heart defects
Tricuspid valve insufficiency leads to the formation of regurgitation of blood or its reverse flow from the atrium to the ventricle. This occurs at the moment of systole (output of the right ventricle). Relaxed valves bend under blood pressure.
This condition can occur due to mechanical blockage of the aorta. More often than not, patients acquire the disease during their lifetime. But there are examples of congenital heart defects.
Recommendations
- "Anatomy of the tricuspid valve." e-echocardiography.com
. Received 2018-03-30. - Richard Van Prag: Anatomy of the Heart in A.C. Chang et al.: Pediatric Cardiac Intensive Care, Philadelphia, 1998.
- Healthline Editorial Team. "Right atrioventricular valve (tricuspid valve)." Health line
. - Reynertson, Sandra I.; Kundur, Ramesh; Mullen, J. Martin; Costanzo, Maria Rosa; McKiernan, Thomas L.; Louis, Eric K. (1999-08-03). "Asymmetry of right ventricular enlargement in response to tricuspid regurgitation." Circulation
.
100
(5):465–467. Doi:10.1161/01.CIR.100.5.465. ISSN 0009-7322. PMID 10430758. - "Enlarged heart - symptoms and causes." Mayo Clinic
. Received 2018-03-30. - Demin A.A., Drobysheva V.P., Welter O.Yu. (2000). "[Infective endocarditis in intravenous drug abusers]." Clinical medicine
(in Russian).
78
(8): 47–51. PMID 11019526. - Bhutani J, Dev V, Leong SV, Soor GS, Thangarupan M, Borger MA. (2006). "Infective endocarditis of the tricuspid valve." Journal of Cardiac Surgery
.
21
(6): 603–4. Doi:10.1111/j.1540-8191.2006.00313.x. PMID 17073968. - ^ a b
Mitchell R. S., Kumar V., Robbins S. L., Abbas A. K., Fausto N. (2007).
Robbins Basic Pathology
(8th ed.). Saunders/Elsevier. pp. 406–8. ISBN 1-4160-2973-7. - Tricuspid Valve Disease Mount Sinai Hospital, New York
- University Circle Inc. Archived 2008-06-17 on the Wayback Machine
Forms of pathologies
Valve malfunction occurs for the following reasons:
- Lack of essential microelements in the body, on which the density and elasticity of the tissues that form the valve plates depends.
- Impaired functionality of the tricuspid valve may occur due to a malfunction of neighboring parts of the heart.
Due to stagnation of blood in the body, the tricuspid heart valve does not close completely. May render a person incapacitated. Hypertrophied walls of the atrium are formed due to dilatation (expansion) of the right ventricle. This results in stagnant processes in the arteries and veins.
Pathology can be detected by internal sensations and by the swelling of a vein in the neck at the moment of pushing blood out of the heart. Venous pressure usually increases. The liver is significantly enlarged.
Diseases
In patients in good health, the heart valve apparatus functions clearly and stably. When changes occur, the heart valves are subject to the following pathologies:
- narrowing of the valve snorts;
- reverse blood flow;
- a combination of both anomalies.
Due to the fact that the functions of the semilunar and atrioventricular snorts are carried out at different periods of time, narrowing and insufficiency manifest themselves in different ways.
Narrowing of the semilunar valves leads to the formation of murmurs. Atrioventricular narrowing manifests itself as a murmur in the bicuspid and 3-cuspid snort. Insufficiency in the first category is caused by diastole noise and is called aortic and pulmonary.
A disease such as insufficiency causes pathological changes in which the blood flow begins to return, despite the closure of the valve. Thus, the organ begins to work under increased stress and this is a stimulus for the development of diseases.
Causes and symptoms
Among the established causes of weakening of the tricuspid valve are the following:
- Carcinoid syndrome.
- Consequences of developed rheumatism.
- With endocarditis of infectious origin.
- Mechanical damage to the papillary muscles or rupture of the chordae.
- Consequence of myocarditis.
- After cardiomyopathy.
- A consequence of severe conditions of thyrotoxicosis.
Congenital pathologies often occur together with other abnormalities in the structure of the heart. Tricuspid valve stenosis can lead to chest retraction, which the doctor detects by palpation. Also, when listening to the heartbeat, significant noise appears during systole (the ejection of blood from the ventricle).
However, murmurs can only be detected in acute failure. Less severe symptoms are often ignored. For an accurate diagnosis, instrumental examination using devices is required.
Diagnostic methods
Systolic murmur during inspiration is important for diagnosis. This indicates tricuspid valve insufficiency. However, it should be remembered that this phenomenon is not permanent and may disappear completely for some time. To confirm the preliminary diagnosis, an electrocardiogram is taken.
In the resulting pathology graph one observes:
- deviation of the electrical axis to the right;
- an increase in the size of the P wave (in the area of the second and third chest leads).
Radiography may also be used. The image shows dilatation of the ventricle or atrium. Deviations are also noticeable in echocardiography images, where abnormal movements of the heart septa are established. When analyzing the patient’s condition, the following points are taken into account:
- Type of noise and area of its manifestation.
- The size of the heart, it is often enlarged.
- The presence of stagnation in the blood circulation.
- The magnitude of venous pressure.
- Liver size.
- Condition of the chest.
- Right atrial pressure.
conclusions
The basis of prevention for tricuspid valve pathology is timely examination and treatment. Drug therapy can be effective only in the early stages. If valvular dysfunction is detected late, surgical intervention is indicated. As a rule, the life expectancy of a patient with tricuspid stenosis is no more than 20 years, with insufficiency - 25-30. Currently, successful implantation, plastic surgery, correction or prosthetic valve replacement is carried out surgically, which makes it possible to prevent dangerous complications, death and prolong the patient’s life.
Physical pathologies
A narrowing of the valve opening is called stenosis. This phenomenon occurs under the influence of rheumatism, congenital defects, as well as prolonged mechanical exposure. As a result of the disease, pressure on the walls of the heart increases. The atrium enlarges. Congestion begins in the circulatory system.
To treat mild cases of pathology, preventive measures are carried out. Starting from the second degree of severity, surgical intervention is already recommended. The valve is processed with a scalpel, as a result it is often necessary to sew the plates together or leave only two instead of three. According to statistics, about 14% of patients do not survive the operation.
But even after successful treatment, the patient already becomes disabled. It is necessary to avoid physical activity and undergo periodic examinations to exclude further progression of the pathology.