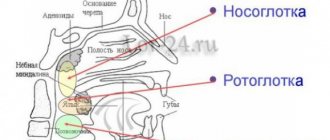
Functions of the leg veins
The veins of the legs have a difficult task - without contractility, they must deliver a mass of blood from the most distant parts of the body to the heart.
This is what predetermined the structure of the network, divided into superficial and deep vessels, connected by a network of perforating ducts. Their walls consist of three layers:
- Intima is the inner layer of endothelium, separated from the middle layer by a thin membrane.
- The medial layer is the middle “layer” of the tube, represented by elastic fibers and a small proportion of muscle fibers. It is this layer that gives them strength and stretchability.
- The outer layer, consisting of connective tissue bordering the membrane that separates the blood tubes from the muscle tissue.
Despite the fact that in the lower extremities the drainage network is represented by tubes of different diameters (from 1.5 to 11 mm), the anatomy of the veins is almost the same. The only difference is the thickness of each layer and the number of valves. For example, the veins of the lower leg have more valves, but their diameter is 2 times smaller than that of the great saphenous vein.
In addition to blood pressure, superficial vessels experience significant stress due to external influences, so the thickness of their middle layer is much greater than that of deep-lying tubes. For example, the walls of the great saphenous vein are 1.3 times thicker and stronger than those of the deep vein.
The main functions of the VNK are:
- Ensuring uninterrupted outflow of blood, in which carbon dioxide and waste products of tissues located within their reach are dissolved.
- Delivery to tissues of hormones, organic compounds (enzymes, amino acids, proteins), vitamins and microelements coming from the intestines.
- Regulation of general blood pressure.
It is the variety of tasks assigned to the VNK that has led to close attention to the condition of the blood vessels. Any deviation in their functionality can cause irreparable harm to health.
Varicose veins on the legs - symptoms and treatment
Taking into account modern treatment methods, the prognosis for varicose veins is favorable. Even in the most seemingly advanced cases, the elimination of varicose veins leads to a rapid improvement in the patient’s condition [8] [11].
However, when planning treatment, it is very important to assess its risks, since any intervention still carries potential adverse events. The direct responsibility of the doctor is to reduce their likelihood as much as possible. Before any manipulation, it is necessary to discuss with the patient all points regarding the intervention and obtain his signature on informed consent.
All adverse events can be divided into risks associated with surgery, including anesthesia, and risks on the part of the patient.
The risks of the operation may be small, for example, inflammation (phlebitis) in “welded” or sclerotic veins, accompanied by compaction in their projection and moderate pain. Areas of skin with reduced sensitivity and hyperpigmentation of the skin may appear. All these phenomena are temporary and, as a rule, pass quickly enough without any consequences [1].
Major complications include deep vein thrombosis, allergic and toxic reactions to anesthetic drugs. They are extremely rare, but for an individual patient who experiences such a complication, the case is 100 percent, even with statistics of 1 case per 10,000 operations.
Prevention of venous thrombosis is primarily based on calculating its risk using the so-called scoring system using the Caprini table. It contains various risk factors that have their own gradation. Taking into account each factor and obtaining a total score determines the degree of risk and, accordingly, its prevention. The main means of preventing venous thromboembolic complications are as follows:
- minimizing the trauma of the operation;
- early activation of the patient;
- compression jersey;
- pharmacological prevention, i.e., prescription of anticoagulants according to indications - blood thinning drugs (low molecular weight heparins or direct oral anticoagulants) [10].
Allergic and toxic reactions to the drug are, unfortunately, very difficult to predict. Testing for allergies to certain drugs does not prevent its occurrence and is not used in world practice. Therefore, it is extremely important to be prepared for the occurrence of these complications in any patient and to be able to provide immediate assistance. For this purpose, special equipment (first aid kits) with all necessary medications are always available in the operating room.
Risks from patients are usually associated with concomitant pathologies, for example, hypertension, coronary heart disease, epilepsy, etc. To prevent attacks of such diseases, a thorough medical history is taken and consultations with specialists are scheduled, who “give the go-ahead” for the operation.
As for the prevention of varicose veins, it simply does not exist, since the main cause of the pathology is still not clear, which could be influenced and thus prevent the occurrence of the disease. This is also associated with fairly frequent relapses of varicose veins after any type of intervention. However, given all the advantages of minimally invasive treatment, this is not a significant problem. Keeping your legs in order is quite simple, the main thing is to contact a phlebologist in time[3][5][6][10].
Deep veins of the lower extremities
Localization of the deep veins of the lower extremities (abbreviated as DVNK) is the thickness of the muscles along the entire length of the legs and thighs. The GVNK include:
- femoral;
- anterior tibial;
- posterior tibial;
- fibula;
- popliteal
The deep ducts are located near the arteries of the same name, and are connected to the superficial ones by a network of perforating vessels. Their walls are highly elastic and resilient. There are numerous valves along the entire length. The thickness of the GVNK ranges from 3 to 10 mm.
In the lower part of the bed, metatarsal vessels flow into the GVNK, from where blood flows through the tibial anterior vein into the popliteal vein. Next, the deep vein of the thigh, which flows into the iliac vessel located in the groin area, is responsible for the drainage of blood. It contains up to 5 valves that support fluid flow in one direction. Part of the blood is “dumped” through a network of perforating tubes into the superficial channels.
The deep-lying network at the level of the lower leg runs virtually parallel to the arterial network, and in the thigh area they are located at a distance from each other.
Phlebology
The anatomy of the venous system of the lower extremities is highly variable. Knowledge of the individual structural features of the human venous system plays a major role in assessing instrumental examination data in choosing the correct treatment method.
In the venous system of the lower extremities, a deep and superficial network is distinguished.
The deep venous network is represented by paired veins accompanying the arteries of the fingers, foot and leg. The anterior and posterior tibial veins merge in the femoropopliteal canal and form the azygos popliteal vein, which passes into the powerful trunk of the femoral vein (v. femoralis). 5-8 perforating veins and the deep vein of the thigh (v. femoralis profunda), which carries blood from the muscles of the back of the thigh, flow into the femoral vein, even before passing into the external iliac vein (v. iliaca externa). The latter, in addition, has direct anastomoses with the external iliac vein (v. iliaca externa), through intermediary veins. In case of occlusion of the femoral vein, part of the femoral vein may flow through the deep vein system into the external iliac vein (v. iliaca externa).
The superficial venous network is located in the subcutaneous tissue above the superficial fascia. It is represented by two saphenous veins - the great saphenous vein (v. saphena magna) and the small saphenous vein (v. saphena parva).
The great saphenous vein (v. saphena magna) starts from the internal marginal vein of the foot and along its entire length receives many subcutaneous branches of the superficial network of the thigh and lower leg. In front of the inner ankle, it rises to the lower leg and, going around the back of the inner condyle of the femur, rises to the oval opening in the groin area. At this level it flows into the femoral vein. The great saphenous vein is considered the longest vein in the body, has 5-10 pairs of valves, and its diameter along its entire length ranges from 3 to 5 mm. In some cases, the great saphenous vein of the thigh and leg can be represented by two or even three trunks. 1-8 tributaries flow into the uppermost section of the great saphenous vein, in the groin area; these are often three branches that do not have much practical significance: the external genital (v. pudenda externa super ficialis), superficial epigastric (v. epigastica superficialis) and the superficial vein surrounding the ilium (v. cirkumflexia ilei superficialis).
The small saphenous vein (v. saphena parva) begins from the external marginal vein of the foot, collecting blood mainly from the sole. Rounding the outer ankle from behind, it rises along the middle of the back surface of the lower leg to the popliteal fossa. Starting from the middle of the leg, the small saphenous vein is located between the layers of the fascia of the leg (N.I. Pirogov’s canal) accompanied by the medial cutaneous nerve of the calf. And therefore, varicose veins of the small saphenous vein are much less common than the large saphenous vein. In 25% of cases, the vein in the popliteal fossa passes through the fascia deep and flows into the popliteal vein. In other cases, the small saphenous vein can rise above the popliteal fossa and flow into the femoral, large saphenous vein, or into the deep vein of the thigh. Therefore, before the operation, the surgeon must know exactly where the small saphenous vein flows into the deep one in order to make a targeted incision directly above the anastomosis. Both saphenous veins widely anastomose with each other by direct and indirect anastomoses and are connected through numerous perforating veins with the deep veins of the leg and thigh. (Fig.1).
Fig.1. Anatomy of the venous system of the lower extremities
Perforating (communicating) veins (vv. perforantes) connect the deep veins with the superficial ones (Fig. 2). Most perforating veins have valves located suprafascially, which allow blood to move from the superficial to the deep veins. There are direct and indirect perforating veins. Direct ones directly connect the main trunks of the superficial and deep veins, indirect ones connect the saphenous veins indirectly, that is, they first flow into the muscular vein, which then flows into the deep vein. Normally they are thin-walled and have a diameter of about 2 mm. If the valves are insufficient, their walls thicken and their diameter increases 2-3 times. Indirect perforating veins predominate. The number of perforating veins on one limb ranges from 20 to 45. In the lower third of the leg, where there are no muscles, direct perforating veins predominate, located along the medial edge of the tibia (Cockett's area). About 50% of the communicating veins of the foot do not have valves, so blood from the foot can flow from deep veins to superficial ones, and vice versa, depending on the functional load and physiological conditions of outflow. In most cases, perforating veins arise from tributaries rather than from the trunk of the great saphenous vein. In 90% of cases, there is incompetence of the perforating veins of the medial surface of the lower third of the leg.
Fig.2. Options for connecting the superficial and deep veins of the lower extremities according to S. Kubik.
1 - skin; 2 - subcutaneous tissue; 3 - superficial fascial leaf; 4 - fibrous bridges; 5 - connective tissue sheath of the saphenous veins; 6 - own fascia of the leg; 7 - saphenous vein; 8 - communicating vein; 9 - direct perforating vein; 10 - indirect perforating vein; 11 - connective tissue sheath of deep vessels; 12 - muscle veins; 13 - deep veins; 14 - deep artery.
Deep veins of the legs
The inferior vena cava system originates from the veins of the fingers, the venous arch of the sole and the dorsum of the foot.
- Diseases of the superficial veins of the lower extremities and treatment methods
From the venous arch of the dorsum of the foot, blood flows into the deep anterior tibial veins (DATIVs).
From the venous arch of the sole, the posterior tibial veins (PTV) and peroneal veins (MPV) are born.
The deep veins of the leg follow with the artery two, rarely four or more; merge before PKV.
PBBV lie in the anterior muscle bed of the leg; through the interosseous membrane they merge into the BBBV.
The internal and external marginal veins of the sole in the calcaneal canal will form two trunks of the BBBV.
ZBBV on n/3 of the leg immediately behind the muscular fascia, then between the flexors and the triceps muscle.
The MBV arises from the posterolateral calcaneus, superiorly between the MBV and the flexor pollicis longus.
On the third third of the leg, the deep veins merge, thus giving rise to the short trunk of the popliteal vein (PCV).
Drainage of the soleus and gastrocnemius muscles into the soleus and gastrocnemius (sural) veins.
- Femoral vein - anatomy, functions and pathologies of the femoral vein
Close to the joint space of the knee joint, the soleus and gastrocnemius veins merge into the PCV.
The SVC lies posterior to the RCA, from its junction with the thigh, called the superficial femoral vein (SFE).
The SMV from its confluence with the deep femoral vein (DFE) is called the common femoral vein (CFV).
The EIVs collect blood from the lower extremities and continue into the external iliac veins (ELVs).
At L5, the iliac vein and internal iliac vein (Iiliac vein) join to form the common iliac vein (CIV).
At L4, the IVCs drain into the inferior vena cava (IVC); The IVC runs to the right of the aorta and has no valves.
Superficial veins of the lower extremities
Superficial VNK are responsible for draining blood from the toes and metatarsal part of the foot, therefore the localization of the superficial veins of the lower extremities is limited to the foot and ankle. The list of blood vessels located along the upper (front) part of the leg includes:
- dorsal digital vessels;
- dorsal arch of the foot;
- medial marginal tube;
- lateral marginal tube.
On the one hand, the superficial VNCs border with the venules of the toes and feet, and on the other, they connect with the large and small saphenous ducts.
- Varicose veins of the lower extremities: stages, causes, symptoms and treatment
On the underside of the foot, the superficial network is represented by plantar digital ducts flowing into the plantar arch. The vessels then connect to the medial and lateral plantar tubes, which empty into the posterior tibial tube.
The diameter of this group of blood ducts ranges from 1.5 to 3 mm. Due to their short length, they have fewer valves, but the walls are quite dense and elastic due to the large number of reticular and collagen fibers, as well as spirally arranged muscle cells.
Superficial VNK are clearly visible under the thin skin of the feet, which is practically devoid of subcutaneous tissue. They look like bluish tracks, and with heavy stress on the legs they can swell and become bulging.
Material and methods
Since the beginning of 2015, MSCT venography was performed on 121 people. Initially, 30 lower extremities were examined in individuals without signs of CVD (control group). The study group included 91 patients (52 women and 39 men aged 32 to 65 years) with CVD with clinical class C0-C6. Class C0—C1 occurred in 15 (16.5%) patients, C2—C3 — in 45 (49.5%). 31 (34%) patients had various trophic skin disorders (C4-C6).
All studies were performed on a 128-slice Philips Ingenuity CT multislice computed tomograph with the Intell Space Portal image processing software package, followed by reconstruction of a volumetric image in 3D mode.
The scanning was carried out in an automatic program mode, which implied sequential non-stop administration of a bolus of contrast agent and saline solution.
Scan mode: collimation 64×0.625; pitch 0.923; kilovoltage 100 kV; mAS 188; reconstruction parameters: axial + cranial orientation.
MSCT venography was performed according to the method we developed. In a clean dressing room or in a study room, the vein of the dorsum of the foot was catheterized using an intravenous catheter G22-G24. The patient was placed on the table on his back. One of two infusion syringes (A) was filled with 50 ml of non-ionic contrast agent (Ultravist). An isotonic sodium chloride solution was drawn into the second infusion syringe (B) at the rate of 1 ml of 0.9% saline per 1 cm of height of the subject. Both infusion syringes were inserted into the auto-injector. Using an infusion line, the injector was connected to an intravenous catheter and the infusion mode was switched on from A to B, with an injection rate of the radiopaque mixture of 4 ml/s.
Computer marking of the scanned limb was carried out, including the pelvis and foot. After preliminary scanning, the scanning area was finally set (the entire lower limb and pelvic area) with a direction from the pelvis to the foot. The scanning time parameters were entered into the program.
A pneumatic cuff was placed over the ankles, the pressure in which was raised to 60 mm Hg, and the administration of a radiopaque mixture began, which, depending on the calculated volume, lasted about 40 s. After completing the administration of the entire volume of contrast and isotonic sodium chloride solution, the pressure in the second cuff placed at the mid-thigh was raised to 60 mmHg, and the patient took a deep breath, held his breath and tensed the muscles of the anterior abdominal wall. From this moment, the first main scan began, the total duration of which was 12-15 s. After this, the patient exhaled and performed five dorsiflexion movements of the foot. After completing the test, the patient returned to the starting position. After 40 s, the second main scan began, after which the study was completed and a three-dimensional image of the limb and veins was reconstructed using automatic Intell Space Portal data processing protocols embedded in the computer.
Vein structure
Their structure has a thinner layer of muscle mass and is less elastic, since the blood pressure in them is several times lower than in the artery.
The veins contain valves that are responsible for the correct direction of blood circulation. Arteries, in turn, do not have valves. This is the main difference between the anatomy of the veins of the lower extremities and the arteries.
Pathologies may be associated with disruption of the functioning of arteries and veins. The walls of blood vessels are modified, which leads to serious disturbances in blood circulation.