Breathing is a process without which a person cannot exist. Anyone who cares about their health should know where a person’s lungs are, how they function and what structure they have. The organ is vital because it supplies the entire body with oxygen.
Where are the lungs located?
The lungs are located on either side of the heart and fill the chest. Each lung of an adult weighs a little more than 400 g
.
The right lung is slightly heavier than the left, since the latter has to share space in the chest with the heart. The lungs are protected by the rib cage
. Between her ribs there are small muscles involved in the breathing process.
Check your lungs
If you smoke, be sure to check your lungs with a simple test. Try blowing out a candle at a distance of a meter.
Beneath the lungs is
the diaphragm
, a dome-shaped muscle formation that separates the chest from the abdominal cavity and is also involved in breathing.
Lungs
Lung structure
The lungs are paired organs located in the chest cavity. They consist of lobes: the right lung contains three lobes, the left - two. Lung tissue consists of bubbles - alveoli, in which a vital process occurs - gas exchange between blood and atmospheric air.
The lung is covered with a membrane - the pleura, which passes from the surface of the lungs to the inner walls of the chest. A pleural cavity is formed between the two layers of the pleura, the pressure in which is lower than atmospheric (it is called negative pressure), which is of fundamental importance for the act of inhalation and exhalation.
Gas exchange in the lungs and tissues
The air moves along the airways and finally reaches the smallest structure of the lung - the pulmonary vesicle, or alveoli. The wall of the alveoli is intertwined with a dense network of capillaries - vessels with a thin wall through which gases diffuse: carbon dioxide leaves the blood into the alveoli, and oxygen enters the blood from the alveoli.
Oxygen dissolved in the blood reaches the internal organs and tissues of the body through the blood vessels. I note that moving through the blood, gases form compounds with hemoglobin in red blood cells:
- Oxygen (O2) - oxyhemoglobin
- Carbon dioxide (CO2) - carbhemoglobin
- Carbon monoxide (CO) - carboxyhemoglobin
The combination of hemoglobin with carbon monoxide is much more stable than the others: carbon monoxide easily wins the competition with oxygen and takes its place. This explains the severe consequences of carbon monoxide poisoning, which quickly accumulates during a fire in a confined space.
As the blood gives up carbon dioxide and takes in oxygen, it turns from venous blood (poor in oxygen) into arterial blood. In tissues, the reverse process occurs: cells need oxygen necessary for tissue respiration, and carbon dioxide, a byproduct of metabolism, requires removal from the cell into the blood.
I often ask students, “What moves the gas, what causes, for example, oxygen to move first from the alveoli to the blood, and in the tissues from the blood to the cells?” Remember that this driving force is the difference in partial pressure of gases.
The partial pressure of a gas is that part of the total volume of gas that falls on the share of this gas. I do not recommend that you memorize the table above, but it is quite good for understanding.
Note that the partial pressure of oxygen in the alveoli is 100-110, and in the venous blood of the capillary that encircles the wall of the alveoli, the oxygen pressure is 40. Thus, oxygen rushes from an area of higher pressure to an area of lower pressure - from the alveoli into the blood.
The ongoing movements of gases can be easily recorded by measuring the concentration of gases in the air inhaled and exhaled by a person. You probably won't need much of this information, but I encourage you to remember that the ambient air contains 21% oxygen and 0.03% carbon dioxide - this is important information.
The liquid covering the walls of the alveoli - surfactant - is important in the transport of gases. Initially, oxygen dissolves in the surfactant and only then diffuses through the capillary wall, entering the blood. Surfactant also prevents the walls of the alveoli from sticking together (collapsing) during exhalation.
Vital capacity of the lungs
One of the physiologically important indicators is vital capacity (VC). Vital capacity is the maximum amount of air that a person can exhale after the deepest breath.
This indicator is very variable; the average vital capacity of an adult is about 3500 cm3. In athletes, vital capacity is 1000-1500 cm3 more, and in swimmers it can reach 6500 cm3. The greater the vital capacity, the more air enters the lungs and oxygen enters the circulatory system, which is very important for tissue cells during sports.
Vital vital capacity is easily measured using a special device - a spirometer (from the Latin spirare - to breathe).
Mechanism of pulmonary respiration
Between the outer surface of the lung and the walls of the chest there is a pleural cavity, which plays a vital role in the process of inhalation and exhalation, and also reduces friction of the lungs during breathing movements.
The pressure in the pleural cavity is always 5-7 mm lower. rt. Art. atmospheric pressure, so the lungs are constantly in an expanded state, fastened through the pleura to the walls of the chest cavity.
Imagine: the lung is pulled up to the pleura, which is attached to the chest. And the chest constantly makes breathing movements, expanding and contracting, thus the lung follows the respiratory movements of the chest.
It remains to figure out how these respiratory movements occur? The reason for this is the contraction and relaxation of the intercostal muscles, as a result of which the chest rises and falls, respectively. Now we will discuss in detail the mechanism of inhalation and exhalation.
When inhaling, the external intercostal muscles contract, while the ribs rise, and the sternum moves forward - the chest expands in the anteroposterior and frontal (to the sides) directions. The diaphragm is a respiratory muscle; during inhalation it contracts and moves down: the chest expands in the vertical direction.
When you exhale, the internal intercostal muscles contract, the ribs lower, the sternum moves back - the chest narrows in the anteroposterior and frontal (to the sides) directions. During exhalation, the diaphragm relaxes and rises: the chest narrows in the vertical direction. Thanks to these movements, inhalation and exhalation are carried out.
Can we take control of our breathing? Easily. But we don’t always control it even during the day, let alone at night. The breathing process is controlled by the respiratory center located in the medulla oblongata of the brain. The respiratory center is automatic - periodically impulses themselves flow to the respiratory muscles, for example, during sleep.
The composition of the blood greatly affects the intensity of breathing. Numerous experiments have shown that an increase in CO2 concentration stimulates the respiratory center. This can explain the increase in breathing during physical activity, for example, running, when CO2 is actively formed in the muscle cells of the legs and enters the blood, breathing becomes more frequent reflexively.
The reflex regulation of breathing is most clearly demonstrated by the experiment with cross circulation, in which the circulatory systems of two dogs are connected. When the trachea is compressed, the first dog stops breathing, and carbon dioxide stops being removed from the blood - its concentration in the blood increases, which leads to shortness of breath (rapid breathing) in the second dog.
Pneumothorax
Normally, the pressure in the pleural cavity is negative, which stretches the lungs. However, with injuries to the chest, the integrity of the pleural cavity may be disrupted: in this case, the pressure in the cavity becomes equal to atmospheric pressure.
Violation of the integrity of the pleural cavity is called pneumothorax (from the ancient Greek πνεῦμα - blow, air and θώραξ - chest). When pneumothorax occurs, the lungs collapse and cease to participate in breathing.
Mountain and decompression sickness
Climbers and mountain hikers (especially beginners) often experience altitude sickness. This condition occurs due to the fact that when rising to a height, the partial pressure of oxygen drops, and its concentration in the blood does not meet the body's needs - it is lower than it should be.
At first, mountain sickness manifests itself as euphoria (unreasonable joy) and increased heart rate. If the conquest of mountain peaks continues, then these symptoms are gradually joined by apathy (a state of indifference), muscle weakness, cramps and headache.
What to do, you ask? It is necessary to immediately stop further ascent, and if symptoms worsen, begin descent. It is best to prevent altitude sickness by following the rule - do not increase the altitude of your overnight stay by more than 300-600 meters.
Caisson disease occurs in divers and is associated with an increase in the partial pressure of a gas - nitrogen, which occurs when diving under water. There is a pattern: the deeper the diver descends, the more nitrogen becomes dissolved in the blood. What is the danger of nitrogen dissolving in the blood?
With a sharp, rapid rise, the solubility of nitrogen in the blood decreases, and the blood literally boils. Just imagine, real gas bubbles appear in the vessels! They can clog the vessels of the lungs, heart, and other internal organs, as a result of which blood circulation stops, and the consequences can be very sad, even fatal.
How to prevent decompression sickness? You can use helium gas in the breathing mixture instead of nitrogen, which does not lead to such consequences. It is also necessary to adhere to the rule of gradual ascent, with stops, and avoid sudden ascent.
© Bellevich Yuri Sergeevich 2018-2021
This article was written by Yuri Sergeevich Bellevich and is his intellectual property. Copying, distribution (including by copying to other sites and resources on the Internet) or any other use of information and objects without the prior consent of the copyright holder is punishable by law. To obtain article materials and permission to use them, please contact Yuri Bellevich
.
How does breathing happen?
Before birth, the baby receives oxygen directly from its mother's blood, so its lungs are filled with fluid and do not work. At the moment of birth, the baby takes his first breath, and from that moment his lungs work without rest. The respiratory center of the brain constantly receives signals about how much oxygen the body requires at any given moment. For example, if a person is sleeping, he needs much less oxygen than when he is running for the bus. The brain sends messages along nerves to the breathing muscles, which help regulate the amount of air entering the lungs. As soon as this signal is received, the diaphragm expands and the muscles stretch the chest outward and upward. This maximizes the volume that the lungs can occupy in the chest. When you exhale, the diaphragm and intercostal muscles relax, reducing the volume of the chest. Due to this, air is pushed out of the lungs.
Human lungs: brief characteristics of the organ
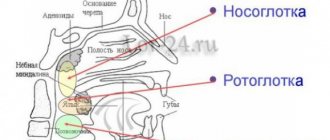
The functioning of the brain, the release of energy, and the breakdown of useful substances with the help of oxygen directly depend on the functioning of the respiratory system. The respiratory organs include the nose, mouth, larynx, trachea, and bronchi, which are part of the lungs.
The lung is one of the paired, most voluminous human organs. In a healthy state, it is pink-red in color, the structure is soft, spongy.
The average volume of the organ is 3 liters, but 450-500 ml is enough for inhalation and exhalation. In people who are actively involved in swimming, the lung volume reaches 5 liters.
For a deep breath, about two liters of atmospheric air are used. With such breathing patterns, a reserve remains in the organ, thanks to which the level of oxygen in the alveoli is maintained at the required level.
In the tissues of each lung, venous and arterial blood constantly moves, and lymphatic vessels are present. It also contains nerve cells that are closely connected with blood vessels and bronchi.
In the first month of pregnancy, the rudiments of the main organ of the respiratory system are already formed in the fetus, and by the fifth month its constituent elements are designated. The organ continues to grow until the age of 25, as the growing organism constantly needs oxygen.
How does oxygen get into the blood?
Through the thin walls of the alveoli, oxygen enters the blood vessels. Here it is picked up by “transport” - hemoglobin
, which is contained in red blood cells. At the same time, carbon dioxide enters the opposite direction - into the alveoli - from the blood, which is removed from the body when exhaling. Oxygenated blood is sent from the lungs to the left side of the heart, from where it is distributed throughout the body through arteries. As soon as the oxygen in the blood is used up, the blood flows through the veins to the right side of the heart and from there back to the lungs.
What does CT1, CT2, CT3, CT4 mean for COVID-19 viral pneumonia?
So that doctors can objectively assess the extent of lung damage, weigh risks and respond to challenges, a unified standard for classifying viral pneumonia by severity was adopted, where:
CT-0— no signs of viral pneumonia;
CT-1 - mild form of pneumonia with areas of “ground glass”, the severity of pathological changes is less than 25%;
CT-2 - moderate pneumonia, 25-50% of the lungs are affected;
CT-3 - moderate pneumonia, 50-75% of the lungs are affected;
KT-4 is a severe form of pneumonia, affecting >75% of the lungs.
The percentage of destruction of lung tissue is determined by tomograms. The radiologist evaluates each of the five lobes of the lungs on a five-point scale.* If signs of pneumonia are not detected, then the value corresponds to 0; A score of 1 indicates 5% lung damage, and so on.
* According to the “Temporary Methodological Recommendations” of the Ministry of Health of the Russian Federation dated October 2021, the adopted and described above scoring system for assessing pulmonary segments and lobes has been abolished. The objectivity of the assessment is supported by software and medical expertise.
In other words, the abbreviation CT1, CT2, CT3 or CT4, which the radiologist writes in the conclusion, indicates the volume of non-functional lung tissue in combination with other signs characteristic of a particular stage. This is an empirical visual scale adopted by radiologists.
This scale for visual assessment of the lungs based on the results of computed tomography (or MSCT) was developed only during the pandemic of a new coronavirus infection. It was introduced by specialists from the US Center for Diagnostics and Telemedicine, having studied CT studies of 13,003 people who made up the main sample.
It is noteworthy that the rate of transition of pneumonia to the next, more complicated degree depends not only on the age of the patient (the older, the faster), but also on the current stage of the disease. Namely, if SARS-CoV-2 viral pneumonia was detected in a patient at the first stage (CT1), then preventing the transition to the next one (CT2) will be easier, at least because a relatively small number of virions require more time to spread throughout the lungs and provoke a more extensive inflammatory process. While the transition from CT3 to CT4 occurs very quickly, and then the patient’s life is at risk. Analyzing the already mentioned group of patients, scientists from the USA came to the conclusion that when moving to the next group, the risk of death from coronavirus increased by approximately 38%.
The percentage of involvement of the parenchyma (damage itself) of the lungs in the reports is usually indicated approximately, so the range of values can be quite wide, but this is not the main indicator. When determining the severity of pneumonia, other signs of pneumonia are taken into account:
1) The presence of “ground glass” on CT scans, their localization, consolidation. “Ground glass” are light areas of the lungs on tomograms that indicate foci of infiltration. Dense fabric does not transmit x-rays. “Ground glass” is the main sign of lung lesions on CT. Their prevalence and consolidation correspond to the severe stages of pneumonia KT3 and KT4.
2) Thickening of the interlobular space of the lungs or “cobblestone sign” - lung tissue on CT scans has an external visual resemblance to paving stones. Corresponds to the severe stage of pneumonia KT4.
3) Symptom of “reverse halo” or “rim” - on tomograms it looks like light rings. These are areas of compaction around the source of infection. Considered a sign of organizing pneumonia.
4) Reticular changes - thin lines of pathologically altered pulmonary interstitium, forming a network.
If the conclusion indicates “polysegmental pneumonia,” this means that signs of the inflammatory process were found in both lungs, in several segments.
What else do the lungs do?
Every day, the lungs of an adult person pump about ten thousand liters of air
.
Consequences of smoking
Chronic obstructive pulmonary disease (COPD) is rightfully considered the most obvious consequence of smoking. Moreover, it is incurable. Find out how to prevent the disease.
With each breath, not only oxygen enters them, but also dust, germs and other foreign objects.
Therefore, the lungs also perform the function of physical and chemical defense against unwanted objects from the air. On the walls of the bronchi there are tiny villi that trap dust and germs
. In the walls of the airways, special cells produce mucus that helps clean and lubricate these villi. Contaminated mucus is removed through the bronchi to the outside and coughed up.
What to do for lung health?
One of the best ways to ensure lung health is to avoid exposure to tobacco smoke, because at least 70 of the 7,000 chemicals in tobacco smoke damage lung cells. According to the Mayo Clinic, tobacco users have the highest risk of developing lung cancer. Moreover, scientists recently discovered that cigarette addiction increases the risk of CoVID-19 disease. The more a person smokes, the higher the risk. But there is good news - as Livescience writes, if a person quits smoking, the lungs can recover from most of the damage.
Rush University Medical Center also suggests practicing breathing exercises and exercising regularly to keep your lungs healthy. Today, in the midst of the novel coronavirus pandemic, the best thing you can do for your own health is to quit smoking and follow the recommendations of the World Health Organization. Read about how to avoid getting infected with CoVID-19 in our special material.