The knee joints are distinguished by a particularly thick and dense cartilage lining - after all, nature intended them to withstand the weight of our body and absorb shocks when walking, running and jumping. And although the average person runs much less than his wild ancestors, this does not make it easier for the joints: they suffer from excess body weight, monotonous loads and even the wrong selection of furniture, due to which the legs do not rest, even if we are sitting. Most sports injuries occur in the knee area.
Doctors warn: gonarthritis (or arthritis of the knee joint) increasingly begins at a young age - starting at 30 years old. What are the symptoms and treatment of knee arthritis? How to treat knee arthritis?
General information about the disease
Inflammation and arthritis of the knee joint is one of the most common diseases. This is due to the peculiarities of the structure, functioning and high loads on the knee joint. Depending on the causes, the disease can manifest itself in the form of damage to one joint (monoarthritis) or several (polyarthritis).
There is no separate code for arthritis of the knee joint according to the International Classification of Diseases, 10th revision (ICD-10); general arthritis codes are used - M00 - M14.
Like all other joint inflammatory processes, arthritis of the knee joint is prone to chronicity, and therefore often causes disability.
Prevention
- The most important factor in favorable disease control is control of BMI (body mass index), which reduces the axial load on the joints. You should avoid foods rich in starch and sugar (potatoes, sweets, sweet flour products). 2. It is worth adding more vegetables and fruits: apples, sea buckthorn, rowan, black currants, plums.
- Include fatty fish in your diet: tuna, salmon, cod, sardines, trout, herring.
- Rejection of bad habits.
- Taking vitamins.
- Hardening.
- Maintaining a healthy lifestyle.
- Strengthening the immune system.
- Maintain an active lifestyle (preferably including regular exercise).
Causes of knee arthritis
Gonarthritis develops after an injury, so it mainly affects children, adolescents and young people. Athletes are at risk. After an open injury, an infection can enter the joint cavity, resulting in an acute inflammatory process.
With a closed injury, acute arthritis of the knee joint can also develop. At first, it is aseptic (without the presence of infection) in nature, and then either recovery occurs, or infection from nearby or distant foci (carious teeth, chronic tonsillitis, boils, etc.) occurs and purulent persecution develops.
The causes of arthritis of the knee joint may be associated with any general infection - gonorrhea, tuberculosis, brucellosis, etc. In such cases, the joint inflammatory process has the characteristics of the infection that caused it.
Another cause of arthritis of the knee joint and a damaging factor is an allergy to the patient’s own tissues (autoallergy). In most cases, there is a hereditary predisposition to these diseases, so people who have close relatives suffering from this pathology (rheumatoid arthritis) are at risk.
Toxic-allergic processes include reactive arthritis of the knee, which develops with certain urogenital, intestinal and nasopharyngeal infections. This arthritis of the knee joints also has genetic roots, which is why signs of knee arthritis appear after an infection. The trigger (triggering factor) in this case is infection. People who are sexually promiscuous are at risk.
Symptoms of knee arthritis
Despite the presence of significant differences in the course of different clinical forms, all patients suffering from arthritis of the knee joints have common symptoms.
The first signs of driving
In most cases, the onset of the disease is acute. It begins with an increase in body temperature, general malaise, and headache. At the same time, the soft tissues over the affected joint become inflamed and swollen, the skin turns red, and pain appears.
In some clinical forms of arthritis of the knee joints, the disease initially develops unnoticed, and the course immediately becomes chronic. The pain may be minor at first, but gradually increases. Such pathological processes include tuberculosis.
It is very important to immediately consult a doctor when joint pain first appears: it is much easier to treat any disease at the initial stage.
Obvious symptoms
In acute cases, all symptoms of knee arthritis can increase very quickly. The combination of increasing inflammation, swelling and pain is especially characteristic of acute purulent arthritis and the onset of rheumatoid arthritis.
Severe pain syndrome prevents flexion and extension of the knee - the first signs of impaired mobility appear. In the future, impaired motor function may increase against the background of a decrease in inflammation due to the destruction of cartilage tissue and the proliferation of connective tissue - ankylosis (immobility of the joint) is formed. At first it is connective tissue ankylosis, and then bone.
To prevent the development of ankylosis, you need to seek medical help in a timely manner.
Dangerous symptoms
Not only is pain, swelling and redness above the knee joint indicative of inflammation, but these symptoms are the main
Dangerous signs of knee arthritis include:
- severe fever and general impairment for several days
may indicate the development of a purulent process; you can’t do without the help of a doctor; - moderate knee pain, lameness, decreased muscle volume (one leg is thinner than the other)
- indicates the presence of a chronic inflammatory process characteristic of tuberculosis; - the development of an inflammatory process in the small joints of the hand and foot against the background of arthritis of the knee joint
- signs of rheumatoid gonitis, requiring the help of a rheumatologist.
Complications and possible consequences of arthritis
The likelihood of early complications of arthritis in the form of panarthritis (acute purulent arthritis), phlegmon (diffused purulent inflammation) and other processes is possible mainly with an infectious form of the disease.
Late complications usually include:
- contractures;
- pathological dislocations;
- osteomyelitis (purulent-necrotic process of bone or bone marrow);
- generalized sepsis (inflammation).
Lack of proper treatment for progressive arthritis can lead to loss of self-care and free movement - disability.
How dangerous is the disease?
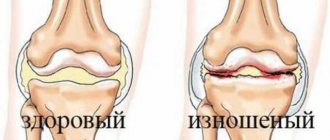
Arthritis of the knee joint is dangerous because it leads to deformation and destruction of the articular surfaces - cartilage and bone tissue. As a result, the function of one of the main joints involved in movement is lost, and the person becomes disabled. The various signs of the disease vary from stage to stage.
Stages of knee arthritis
Any form of arthritis has serious complications, so you should not delay treatment.
See how easily the disease can be cured in 10-12 sessions.
There are 4 stages of disease development with the gradual formation of arthrosis and persistent dysfunction of the joint:
- The initial stage is inflammatory.
Inflammation, swelling, and severe joint pain cause reversible movement disorders. The general condition of the patient is impaired. - Progressive - formation of pannus.
The acute inflammatory process subsides, granulations of loose connective tissue grow in the knee joint, covering the articular surface and destroying the cartilage. Pain during movement is associated with low-grade inflammation and destruction of cartilage tissue. These disorders are also reversible. - Ankylosing - the formation of fibrous ankylosis (immobility of the knee).
The connective tissue becomes dense and fuses with the bone surface, ensuring immobility. The course of the disease has an undulating nature: relapses alternate with remissions. Complete restoration of joint function is problematic. - Deforming - the formation of bone ankylosis and deformation of the knee joint.
In place of the connective tissue, bone grows, the knee is motionless, and it is impossible to restore its function.
Possible complications
Full or partial restoration of joint function is possible at any stage, but if you self-medicate, the consequences can be very sad:
- in acute purulent knee arthritis
- melting of articular tissues, rapid formation of ankylosis, spread of a purulent inflammatory process to surrounding and distant organs and tissues; - in infectious diseases
- a chronic progressive course with the formation of ankylosis, persistent pain and dysfunction of the knee; - in rheumatoid arthritis
- spread of inflammation to small joints with persistent pain, joint deformation and disability.
Methylsulfonylmethane
Methylsulfonylmethane (MSM) is an organosulfur compound. Also known as methylsulfone or dimethylsulfone. Sulfur plays an important role in the formation of connective tissue. This substance is a mild analgesic that reduces pain.
According to a pilot study that involved 50 people with knee osteoarthritis, it was found that when taken at 6000 mg per day, the drug reduced severe symptoms of the disease with minimal side effects. The study was conducted in 2006. Future trials have been conducted numerous times, all of which have shown a reduction in oxidative stress and inflammation through MSM supplementation. It turned out that it protects muscles from various mechanical damage that arise from an active lifestyle.
How do the various clinical forms of knee arthritis occur?
The course of various clinical forms of knee arthritis has its own characteristics.
Acute purulent drive
Symptoms of the disease develop at lightning speed, within a few hours. High fever, chills, muscle pain, headache. The periarticular tissues of the affected knee joint swell, and the skin over it turns red. The pain is very severe, the pain syndrome increases as purulent inflammatory fluid accumulates in the knee.
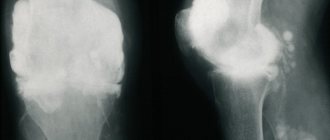
Acute purulent arthritis of the knee joint
A general blood test shows signs of an acute inflammatory process; an x-ray shows narrowing of the joint space, foci of destruction of cartilage and bone tissue. Ultrasound reveals an increase in the volume of inflammatory joint fluid. When a joint is punctured, a cloudy exudate with a putrid odor is removed. Acute purulent arthritis of the knee joint can result in complete recovery or be complicated by deforming arthrosis and disability.
The patient's condition may be serious. The patient requires hospitalization and emergency medical care.
Post-traumatic
Chondroprotectors: what are they, how to choose, how effective are they?
Joint pain at rest
The inflammatory process begins with damage to the inner shell of the joint capsule - synovitis. Slight swelling and tenderness in the knee area limit its movement. All symptoms of post-traumatic arthritis appear within a few hours after the injury. The general condition does not suffer. The course of synovitis is favorable if infection does not occur. Infection from the outside through wounds or through blood flow from distant foci contributes to the development of purulent gonitis. X-rays sometimes show widening of the joint space.
Infectious
Arthritis of the knee joint can develop from a variety of bacterial, fungal, viral and parasitic infections. Each of these diseases has its own characteristics:
- Gonorrheal drives.
It begins acutely 14–21 days after a sexually transmitted infection. Fever appears and the general condition of the patient is disrupted. Usually one knee is affected, it swells, the skin over it turns red, and severe pain appears. In the future, in the absence of adequate treatment, the process can take a chronic course with the rapid formation of deformity and ankylosis and disability. With timely treatment, the outcome is favorable - complete recovery. - Tuberculosis drives.
It begins gradually and has a chronic course with exacerbations and remissions. The pain is minor at first, but gradually increases. Redness and swelling of the periarticular tissues are not pronounced and appear only during an exacerbation, at which time fever may appear. Muscle atrophy (decrease in volume) increases - one leg is thinner than the other, and excess hair growth is observed on the affected limb (hypertrichosis). Movement is limited due to pain. In advanced stages - dislocations and subluxations, breakthroughs of discharge from the articular cavity onto the surface of the skin (fistulas). Gradual complete destruction of the joint and disability.
You should know: even severe infectious gonitis can be treated. In the early stages, they can be cured completely; in the later stages, they can suppress the progression of the pathological process and maintain a normal state. Therefore, seek medical help as soon as possible!
Rheumatoid
The disease is associated with autoimmune reactions (allergy to the patient’s own tissues). Damage to one knee joint in rheumatoid arthritis is rare. More often, polyarthritis develops with gonitis and damage to the small joints of the hand and foot. The disease progresses over a long period of time, in waves, with exacerbations and remissions.
The main sign of rheumatoid gonitis is swelling and redness of the tissue in the knee area and severe debilitating pain. Articular deformity and flexion contracture develop very quickly. Over time, knee stiffness and ankylosis develop.
Systematic correct treatment can stop the progression of rheumatoid gonitis.
Reactive
Reactive arthritis of the knee joint develops within a month after a genitourinary, intestinal or nasopharyngeal infection, mainly in genetically predisposed individuals. The knee swells, the skin over it turns red, and the body temperature rises. Often the course becomes chronic and relapsing. If left untreated, permanent impairment of motor function may occur. But more often the prognosis is favorable - complete recovery occurs.
Juvenile idiopathic
This diagnosis is made if it is impossible to determine the cause of the disease. It occurs mainly in childhood and adolescence in hereditarily predisposed children (more often in girls). The long wave-like course of juvenile arthritis with exacerbations and remissions gradually leads to the formation of ankylosis and early disability.
With timely treatment, it is possible to stop the progression of the process and return the child to normal life.
Psoriatic
Psoriatic arthritis of the knee
Drives with psoriasis can develop in one or both knees. Most often, the first signs of articular damage appear against the background of existing skin manifestations. But sometimes pain in the knee appears several years before the characteristic rashes appear. If characteristic lesions of the end joints of the fingers and nails appear simultaneously, then the diagnosis of psoriatic gonitis is beyond doubt. With a long course of gonitis, persistent ankylosis develops. Interestingly, no pannus is formed.
If symptoms of arthritis of the knee joint appear, treatment is prescribed by a dermatovenerologist together with a rheumatologist.
Gouty
Knee damage due to gout occurs due to the deposition of uric acid salts in the tissues. In the knee area, such a pathology is rare, but can occur acutely with severe pain, significant tissue swelling and redness of the skin. The leg cannot bend due to severe pain. The attack lasts several days, after which it passes without consequences. But with a long course of gout, gradual, persistent impairment of knee function is possible.
Deforming
Long-term chronic recurrent inflammation in the knee leads to the destruction of the cartilage tissue of the articular surfaces. This contributes to constant injury and proliferation of bone tissue. It can grow in the form of spines and marginal growths, deforming the knee and disrupting its function. Arthrosis-arthritis is gradually formed - a combination of inflammatory and degenerative joint processes. Movements in the knee are painful, especially with loads and prolonged standing. The function of the knee joint may be significantly impaired.
Chronic drives
Any form of gonitis can take a chronic course with exacerbations and remissions. This will inevitably lead to impaired joint function. This is why it is so important to promptly seek medical help if knee pain occurs.
Modern drug therapy for rheumatoid arthritis
Rheumatoid arthritis is a disease that has been the focus of attention of rheumatologists around the world for decades. This is due to the great medical and social significance of this disease. Its prevalence reaches 0.5–2% of the total population in industrialized countries [1, 2]. Patients with rheumatoid arthritis experience a decrease in life expectancy compared to the general population by 3–7 years [3]. It is difficult to overestimate the colossal damage caused by this disease to society due to the early disability of patients, which, in the absence of timely active therapy, can occur in the first 5 years from the onset of the disease.
Rheumatoid arthritis is a chronic inflammatory disease of unknown etiology, which is characterized by damage to peripheral synovial joints and periarticular tissues, accompanied by autoimmune disorders and can lead to destruction of articular cartilage and bone, as well as systemic inflammatory changes.
The pathogenesis of the disease is very complex and largely insufficiently studied. Despite this, by now some key points in the development of rheumatoid inflammation are well known, which determine the main methods of therapeutic treatment for it (Fig. 1). The development of chronic inflammation in this case is associated with the activation and proliferation of immunocompetent cells (macrophages, T- and B-lymphocytes), which is accompanied by the release of cellular mediators - cytokines, growth factors, adhesion molecules, as well as the synthesis of autoantibodies (for example, anticitrullinated antibodies) and the formation immune complexes (rheumatoid factors). These processes lead to the formation of new capillary vessels (angiogenesis) and the proliferation of connective tissue in the synovial membrane, to the activation of cyclooxygenase-2 (COX-2) with an increase in the synthesis of prostaglandins and the development of an inflammatory reaction, to the release of proteolytic enzymes, activation of osteoclasts, and as a result - to the destruction of normal joint tissues and the occurrence of deformities.
Treatment of rheumatoid arthritis
Treatment includes:
- drug therapy;
- non-drug therapy methods;
- orthopedic treatment, rehabilitation.
Based on the pathogenesis of the disease, it becomes obvious that it is possible to effectively influence the development of the disease at two levels:
- suppressing excessive activity of the immune system;
- blocking the production of inflammatory mediators, primarily prostaglandins.
Since, in addition to inflammation itself, activation of the immune system is accompanied by many other pathological processes, the effect at the first level is significantly deeper and more effective than at the second. Drug immunosuppression is the mainstay of treatment for rheumatoid arthritis. Immunosuppressive drugs used to treat this disease include disease-modifying anti-inflammatory drugs (DMARDs), biological agents, and glucocorticosteroids. At the second level, non-steroidal anti-inflammatory drugs (NSAIDs) and glucocorticosteroids act.
In general, immunosuppressive therapy is accompanied by a slower development of the clinical effect (in a broad framework - from several days in the case of biological therapy to several months in the case of some DMARDs), which at the same time can be very pronounced (up to the development of clinical remission) and persistent, and is also characterized by inhibition of joint destruction.
Anti-inflammatory therapy itself (NSAIDs) can produce a clinical effect (pain relief, reduction of stiffness) very quickly - within 1-2 hours, however, with the help of such treatment it is almost impossible to completely stop the symptoms of active rheumatoid arthritis and, apparently, it has no effect at all on the development of destructive processes in tissues.
Glucocorticosteroids have both immunosuppressive and direct anti-inflammatory effects, so clinical improvement can develop quickly (within a few hours when administered intravenously or intra-articularly). There is evidence of suppression of the progression of the erosive process in joints during long-term therapy with low doses of glucocorticosteroids and their positive effect on the functional status of the patient. At the same time, it is well known from practice that prescribing only glucocorticosteroids, without other immunosuppressive drugs (DMARDs), rarely provides an opportunity to effectively control the course of the disease.
Non-drug methods of treating rheumatoid arthritis (physiotherapy, balneotherapy, diet therapy, acupuncture, etc.) are additional methods that can slightly improve the patient’s well-being and functional status, but do not relieve symptoms and significantly influence joint destruction.
Orthopedic treatment, including orthotics and surgical correction of joint deformities, as well as rehabilitation measures (physical therapy, etc.) are of particular importance, mainly in the later stages of the disease, to maintain functional ability and improve the patient’s quality of life.
The main goals of treatment for RA are [2, 6]:
- relief of disease symptoms, achievement of clinical remission or at least low disease activity;
- inhibition of the progression of structural changes in joints and corresponding functional disorders;
- improving the quality of life of patients, maintaining their ability to work.
It must be kept in mind that treatment goals may vary significantly depending on the duration of the disease. At an early stage of the disease, i.e., with a disease duration of 6–12 months, achieving clinical remission is a very realistic goal, as well as inhibiting the development of erosions in the joints. With the help of modern methods of active drug therapy, it is possible to achieve remission in 40–50% of patients [4, 5], and the absence of the appearance of new erosions according to radiography [7] and magnetic resonance imaging [8] has also been shown in a significant number of patients with a follow-up duration of 1 -2 years.
With long-term rheumatoid arthritis, especially with insufficiently active therapy in the first years of the disease, achieving complete remission is theoretically also possible, but the likelihood of this is much lower. The same can be said about the possibility of stopping the progression of destruction in joints that have already been significantly destroyed over several years of illness. Therefore, with advanced rheumatoid arthritis, the role of rehabilitation measures and orthopedic surgery increases. In addition, in the later stages of the disease, long-term basic maintenance therapy can be used for secondary prevention of complications of the disease, such as systemic manifestations (vasculitis, etc.), secondary amyloidosis.
Basic therapy for rheumatoid arthritis. DMARDs (synonyms: disease-modifying antirheumatic drugs, slow-acting drugs) are the main component of the treatment of rheumatoid arthritis and, in the absence of contraindications, should be prescribed to every patient with this diagnosis [9]. It is especially important to prescribe DMARDs as quickly as possible (immediately after diagnosis) at an early stage, when there is a limited period of time (several months from the onset of symptoms) to achieve the best long-term results - the so-called “therapeutic window” [10].
Classic DMARDs have the following properties.
- The ability to suppress the activity and proliferation of immunocompetent cells (immunosuppression), as well as the proliferation of synoviocytes and fibroblasts, which is accompanied by a pronounced decrease in the clinical and laboratory activity of RA.
- Persistence of the clinical effect, including its persistence after discontinuation of the drug.
- The ability to delay the development of the erosive process in joints.
- Ability to induce clinical remission.
- Slow development of a clinically significant effect (usually within 1–3 months from the start of treatment).
DMARDs differ significantly in their mechanism of action and features of use. The main parameters characterizing DMARDs are presented in Table 1.
DMARDs can be roughly divided into first-line and second-line drugs. First-line drugs have the best balance of effectiveness (reliably suppress both clinical symptoms and the progression of the erosive process in the joints) and tolerability, and therefore are prescribed to most patients.
First-line DMARDs include the following.
- Methotrexate is the “gold standard” for the treatment of rheumatoid arthritis. Recommended doses of 7.5–25 mg per week are individualized by gradual increases of 2.5 mg every 2–4 weeks until a good clinical response is achieved or intolerance occurs. The drug is given orally (weekly for two consecutive days in 3-4 divided doses every 12 hours). In case of unsatisfactory tolerability of methotrexate when taken orally due to dyspepsia and other complaints associated with the gastrointestinal tract (GIT), the drug can be prescribed parenterally (one IM or IV injection per week).
- Leflunomide (Arava). Standard treatment regimen: 100 mg orally per day for 3 days, then 20 mg/day continuously. If there is a risk of intolerance to the drug (old age, liver disease, etc.), treatment can be started with a dose of 20 mg/day. It is comparable in effectiveness to methotrexate and has slightly better tolerability. There is evidence of higher effectiveness of leflunomide in relation to the quality of life of patients, especially in early rheumatoid arthritis. The cost of treatment with leflunomide is quite high, so it is often prescribed when there are contraindications to the use of methotrexate, its ineffectiveness or intolerance, but it can also be used as the first basic drug.
- Sulfasalazine. In clinical trials, it was not inferior in effectiveness to other DMARDs, but clinical practice shows that sulfasalazine usually provides sufficient control over the course of the disease in cases of moderate and low activity of rheumatoid arthritis.
Second-line DMARDs are used much less frequently due to lower clinical efficacy and/or greater toxicity. They are prescribed, as a rule, when first-line DMARDs are ineffective or intolerable.
DMARDs can cause significant improvement (good clinical response) in approximately 60% of patients. Due to the slow development of the clinical effect, the prescription of DMARDs for periods of less than 6 months is not recommended. The duration of treatment is determined individually; the typical duration of a “course” of treatment with one drug (in case of a satisfactory response to therapy) is 2–3 years or more. Most clinical recommendations suggest indefinite use of maintenance dosages of DMARDs to maintain the achieved improvement.
If monotherapy with any basic drug is insufficiently effective, a combination basic therapy regimen, i.e., a combination of two or three DMARDs, can be chosen. The following combinations have proven themselves to be the most effective:
- methotrexate + leflunomide;
- methotrexate + cyclosporine;
- methotrexate + sulfasalazine;
- methotrexate + sulfasalazine + hydroxychloroquine.
In combination regimens, drugs are usually used in moderate dosages. A number of clinical studies have demonstrated the superiority of combination basic therapy over monotherapy, but the higher effectiveness of combination regimens is not considered strictly proven. Combination DMARDs are associated with a moderate increase in side effects.
Biological drugs in the treatment of rheumatoid arthritis. The term biological drugs (from English biologics) is used in relation to drugs produced using biotechnology and carrying out targeted (“point”) blocking of key moments of inflammation using antibodies or soluble receptors to cytokines, as well as other biologically active molecules. Thus, biological products have nothing to do with “dietary supplements.” Due to the large number of “target molecules” that can potentially suppress immune inflammation, a number of drugs from this group have been developed and several more are undergoing clinical trials.
The main biological drugs registered in the world for the treatment of rheumatoid arthritis include:
- infliximab, adalimumab, etanercept (act on tumor necrosis factor (TNF-α);
- rituximab (acts on CD 20 (B lymphocytes));
- anakinra (acts on interleukin-1);
- abatasept (affects CD 80, CD 86, CD 28).
Biological drugs are characterized by a pronounced clinical effect and reliably proven inhibition of joint destruction. These signs allow biological drugs to be classified as DMARDs. At the same time, a feature of the group is the rapid (often within a few days) development of significant improvement, which combines biological therapy with intensive care methods. A characteristic feature of biological agents is the potentiation of the effect in combination with DMARDs, primarily methotrexate. Due to its high effectiveness in rheumatoid arthritis, including in patients resistant to conventional therapy, biological therapy has now moved to second place (after DMARDs) in the treatment of this disease.
The negative aspects of biological therapy include:
- inhibition of anti-infective and (potentially) anti-tumor immunity;
- the risk of developing allergic reactions and inducing autoimmune syndromes due to the fact that biological drugs are proteins in their chemical structure;
- high cost of treatment.
Biological therapies are indicated if treatment with DMARDs (such as methotrexate) is not adequate due to lack of effectiveness or poor tolerability.
One of the most important target molecules is TNF-a, which has many pro-inflammatory biological effects and contributes to the persistence of the inflammatory process in the synovium, destruction of cartilage and bone tissue through a direct effect on synovial fibroblasts, chondrocytes and osteoclasts. TNF-α blockers are the most widely used biological agents in the world.
A drug from this group, infliximab (Remicade), which is a chimeric monoclonal antibody to TNF-α, has been registered in Russia. The drug is usually prescribed in combination with methotrexate. In patients with insufficient effectiveness of therapy with medium and high doses of methotrexate, infliximab significantly improves the response to treatment and functional indicators, and also leads to a significant inhibition of the progression of joint space narrowing and the development of the erosive process.
The indication for the use of infliximab in combination with methotrexate is the ineffectiveness of one or more DMARDs used at full dose (primarily methotrexate), with the persistence of high inflammatory activity (five or more swollen joints, erythrocyte sedimentation rate (ESR) more than 30 mm/h, C-reactive protein (CRP) more than 20 mg/l). In early rheumatoid arthritis with high inflammatory activity and a rapid increase in structural disorders in the joints, combination therapy with methotrexate and infliximab can be prescribed immediately.
Before prescribing infliximab, a screening examination for tuberculosis (chest x-ray, tuberculin test) is required. Recommended regimen: initial dose of 3 mg/kg of the patient’s body weight intravenously, then 3 mg/kg of body weight after 2, 6 and 8 weeks, then 3 mg/kg of body weight every 8 weeks, if the dose is insufficiently effective may increase up to 10 mg/kg body weight. The duration of treatment is determined individually, usually at least 1 year. After discontinuation of infliximab, maintenance therapy with methotrexate is continued. It should be kept in mind that re-administration of infliximab after completion of treatment with this drug is associated with an increased likelihood of delayed-type hypersensitivity reactions.
The second drug registered in our country for biological therapy is rituximab (Mabthera). The action of rituximab is aimed at suppressing B lymphocytes, which are not only the key cells responsible for the synthesis of autoantibodies, but also perform important regulatory functions in the early stages of immune reactions. The drug has pronounced clinical efficacy, including in patients who do not respond sufficiently to infliximab therapy.
For the treatment of rheumatoid arthritis, the drug is used at a dose of 2000 mg per course (two infusions of 1000 mg, each with an interval of 2 weeks). Rituximab is administered intravenously slowly; infusion in a hospital setting is recommended with the possibility of precise control over the rate of administration. To prevent infusion reactions, it is advisable to pre-administer methylprednisolone 100 mg. If necessary, a second course of rituximab infusions can be performed after 6–12 months.
According to European clinical guidelines, it is advisable to prescribe rituximab in cases of ineffectiveness or impossibility of infliximab therapy. The possibility of using rituximab as the first biological drug is currently the subject of research.
Glucocorticosteroids. Glucocorticosteroids have a multifaceted anti-inflammatory effect due to the blockade of the synthesis of proinflammatory cytokines and prostaglandins, as well as inhibition of proliferation due to their effect on the genetic apparatus of cells. Glucocorticosteroids have a rapid and pronounced dose-dependent effect on the clinical and laboratory manifestations of inflammation. The use of glucocorticosteroids is fraught with the development of undesirable reactions, the frequency of which also increases with increasing doses of the drug (steroid osteoporosis, drug-induced Itsenko-Cushing syndrome, damage to the gastrointestinal mucosa). These drugs alone in most cases cannot provide complete control over the course of rheumatoid arthritis and must be prescribed together with DMARDs.
Glucocorticosteroids for this disease are used systemically and locally. For systemic use, the main method of treatment is the administration of low doses orally (prednisolone - up to 10 mg/day, methylprednisolone - up to 8 mg/day) for a long period with high inflammatory activity, polyarticular lesions, and insufficient effectiveness of DMARDs.
Medium and high doses of glucocorticosteroids orally (15 mg/day or more, usually 30-40 mg/day in terms of prednisolone), as well as pulse therapy with glucocorticosteroids - intravenous administration of high doses of methylprednisolone (250-1000 mg) or dexamethasone (40-1000 mg). 120 mg) can be used to treat severe systemic manifestations of rheumatoid arthritis (effusive serositis, hemolytic anemia, cutaneous vasculitis, fever, etc.), as well as some special forms of the disease. The duration of treatment is determined by the time required to relieve symptoms and is usually 4–6 weeks, after which a gradual stepwise dose reduction is carried out with a transition to treatment with low doses of glucocorticosteroids.
Glucocorticosteroids in medium and high doses, pulse therapy, apparently, do not have an independent effect on the course of rheumatoid arthritis and the development of the erosive process in the joints.
For local therapy, drugs are used in microcrystalline form, prescribed in the form of intra-articular and periarticular injections: betamethasone, triamsinolone, methylprednisolone, hydrocortisone.
Glucocorticosteroids for local use have a pronounced anti-inflammatory effect, mainly at the injection site, and in some cases - a systemic effect. Recommended daily doses are: 7 mg for betamethasone, 40 mg for triamsinolone and methylprednisolone, 125 mg for hydrocortisone. This dose (in total) can be used for intra-articular injection into one large (knee) joint, two medium-sized joints (elbows, ankles, etc.), 4-5 small joints (metacarpophalangeal, etc.), or for periarticular administration of the drug at 3–4 points.
The effect after a single injection usually occurs within 1–3 days and lasts for 2–4 weeks if well tolerated.
In this regard, it is not advisable to prescribe repeated injections of glucocorticosteroids into one joint earlier than after 3-4 weeks. Carrying out a course of several intra-articular injections into the same joint has no therapeutic meaning and is fraught with complications (local osteoporosis, increased destruction of cartilage, osteonecrosis, suppuration). Due to the increased risk of osteonecrosis, intra-articular injection of glucocorticosteroids into the hip joint is generally not recommended.
Glucocorticosteroids for local use are prescribed as an additional method for relieving exacerbations of rheumatoid arthritis and cannot serve as a replacement for systemic therapy.
NSAIDs. The importance of NSAIDs in the treatment of rheumatoid arthritis has decreased significantly in recent years due to the emergence of new effective pathogenetic therapy regimens. The anti-inflammatory effect of NSAIDs is achieved by suppressing the activity of COX, or selectively COX-2, and thereby reducing the synthesis of prostaglandins. Thus, NSAIDs act on the final link of rheumatoid inflammation.
The effect of NSAIDs in rheumatoid arthritis is to reduce the severity of symptoms of the disease (pain, stiffness, swelling of the joints). NSAIDs have an analgesic, anti-inflammatory, and antipyretic effect, but have little effect on laboratory parameters of inflammation. In the vast majority of cases, NSAIDs are not able to significantly change the course of the disease. Their prescription as the only antirheumatic drug for a definite diagnosis of rheumatoid arthritis is currently considered a mistake. However, NSAIDs are the mainstay of symptomatic therapy for this disease and in most cases are prescribed in combination with DMARDs.
Along with the therapeutic effect, all NSAIDs, including selective ones (COX-2 inhibitors), can cause erosive and ulcerative damage to the gastrointestinal tract (primarily its upper parts - “NSAID gastropathy”) with possible complications (bleeding, perforation, etc.), as well as nephrotoxic and other adverse reactions.
The main characteristics that must be considered when prescribing NSAIDs are as follows.
- There are no significant differences between NSAIDs in terms of effectiveness (for most drugs, the effect is proportional to the dose up to the maximum recommended).
- There are significant differences in tolerability between different NSAIDs, especially with regard to gastrointestinal involvement.
- The incidence of adverse effects is usually proportional to the dose of NSAIDs.
- In patients with an increased risk of developing NSAID-associated gastrointestinal lesions, the risk can be reduced by concurrent administration of proton pump blockers and misoprostol.
There is individual sensitivity to various NSAIDs in terms of both effectiveness and tolerability of treatment. Doses of NSAIDs for rheumatoid arthritis correspond to standard doses. The duration of NSAID treatment is determined individually and depends on the patient’s need for symptomatic therapy. If there is a good response to DMARD therapy, the NSAID drug may be discontinued.
The most commonly used NSAIDs for rheumatoid arthritis include:
- diclofenac (50–150 mg/day);
- nimesulide (200–400 mg/day);
- celecoxib (200–400 mg/day);
- meloxicam (7.5–15 mg/day);
- ibuprofen (800–2400 mg/day);
- lornoxicam (8–12 mg/day).
Selective NSAIDs, while not significantly different in effectiveness from non-selective ones, are less likely to cause NSAID gastropathy and serious adverse reactions from the gastrointestinal tract, although they do not exclude the development of these complications. A number of clinical studies have demonstrated an increased likelihood of developing severe vascular pathology (myocardial infarction, stroke) in patients receiving drugs from the coxib group, and therefore the possibility of treatment with celecoxib should be discussed with particular caution in patients with coronary artery disease and other serious cardiovascular pathologies.
Additional drug treatments. As a symptomatic analgesic (or an additional analgesic if NSAIDs are insufficiently effective), paracetamol (acetaminophen) can be used at a dose of 500–1500 mg/day, which has relatively low toxicity. For local symptomatic therapy, NSAIDs are used in the form of gels and ointments, as well as dimethyl sulfoxide in the form of a 30–50% aqueous solution in the form of applications. In the presence of osteoporosis, appropriate treatment with calcium, vitamin D3, bisphosphonates, and calcitonin is indicated.
General principles of management of patients with RA
A patient diagnosed with rheumatoid arthritis should be prescribed a drug from the DMARD group, which, with a good clinical effect, can be used as the only method of therapy [9]. Other medications are used as needed.
The patient should be informed about the nature of his disease, course, prognosis, the need for long-term complex treatment, as well as possible adverse reactions and a treatment monitoring scheme, unfavorable combinations with other drugs (in particular, alcohol), possible activation of foci of chronic infection during treatment , the advisability of temporarily discontinuing immunosuppressive drugs in the event of acute infectious diseases, the need for contraception during treatment.
Therapy for rheumatoid arthritis should be prescribed by a rheumatologist and carried out under his supervision. Treatment with biological drugs can only be carried out under the supervision of a rheumatologist who has sufficient knowledge and experience to carry it out. Therapy is long-term and involves periodic monitoring of disease activity and assessment of response to therapy. A simplified algorithm is presented in Figure 2.
Monitoring disease activity and response to therapy includes assessment of joint status indicators (number of painful and swollen joints, etc.), acute-phase blood parameters (ESR, CRP), assessment of pain and disease activity using a visual analogue scale, assessment of the patient’s functional activity in daily activities with using the Russian version of the Health Questionnaire (HAQ). There are internationally recognized methods for quantifying response to treatment using the DAS (Disease Activity Score) recommended by the European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR) criteria [1]. In addition, the safety of the therapy administered to the patient should be monitored (in accordance with both the formulary and existing clinical guidelines). Due to the fact that the erosive process can develop even with low inflammatory activity, in addition to assessing the activity of the disease and response to therapy, radiography of the joints is mandatory. The progression of destructive changes in the joints is assessed by standard radiography of the hands and feet using the radiological classification of the stages of rheumatoid arthritis, quantitative methods using the Sharp and Larsen indices. In order to monitor the patient’s condition, examinations are recommended to be carried out at certain intervals (Table 2).
Treatment of treatment-resistant RA
It is advisable to consider a patient resistant to treatment if there is ineffectiveness (lack of 20% improvement in the main indicators) of at least two standard DMARDs in sufficiently high doses (methotrexate - 15-20 mg/week, sulfasalazine - 2000 mg/day, leflunomide - 20 mg/day) . Failure can be primary or secondary (occurring after a period of satisfactory response to therapy or when the drug is re-prescribed). There are the following ways to overcome resistance to therapy:
- prescription of biological drugs (infliximab, rituximab);
- prescription of glucocorticosteroids;
- use of combination basic therapy;
- use of second-line DMARDs (cyclosporine, etc.).
From the point of view of long-term results in relation to functional impairment, quality of life and its duration, the optimal treatment strategy for rheumatoid arthritis is long-term treatment with DMARDs with a systematic change in the regimen of their use as needed [11].
Literature
- Clinical recommendations. Rheumatology/ sub. ed. E. L. Nasonova. M.: GEOTAR-Media, 2006. 288 p.
- Emery P., Suarez-Almazor M. Rheumatoid Arthritis // Clin Evid. 2003; 10: 1454–1476.
- Nasonov E. L., Karateev D. E., Chichasova N. V., Chemeris N. A. Modern standards of pharmacotherapy for rheumatoid arthritis // Clinical pharmacology and therapy. 2005. T. 14. No. 1. P. 72–75.
- Balabanova R. M., Karateev D. E., Kashevarov R. Yu., Luchikhina E. L. Leflunomide (Arava) for early rheumatoid arthritis // Scientific and practical rheumatology. 2005. No. 5. pp. 31–34.
- Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Allaart CF et al. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): a randomized, controlled trial // Arthritis Rheum. 2005; v. 52; 11: 3381–90.
- Smolen et al. Therapeutic strategies in early rheumatoid arthritis //Best Practice & Research Clinical Rheumatology. 2005; 19; 1: 163–177.
- Breeveld F.C., Emery P., Keystone E. et al. Infliximab in active early rheumatoid arthritis // Ann Rheum Dis 2004; 63: 149–155.
- Quinn MA, Conaghan PG, O'Connor PJ et al. Very early treatment with infliximab in addition to methotrexate in early, poor-prognosis rheumatoid arthritis reduces magnetic resonance imaging evidence of synovitis and damage, with sustained benefit after infliximab withdrawal: results from a twelve-month randomized, double-blind, placebo-controlled trial // Arthritis Rheum. 2005; 52; 1:27–35.
- American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis. 2002 Update // Arthritis Rheum. 2002; 46: 328–346.
- Quinn MA, Emery P. Window of opportunity in early rheumatoid arthritis: possibility of altering the disease process with early intervention// Clin Exp Rheumatol. 2003; 21; Suppl 31:154–157.
- Karateev D. E. Retrospective assessment of long-term basic therapy in patients with rheumatoid arthritis // Scientific and practical rheumatology. 2003. No. 3. pp. 32–36.
D. E. Karateev , Doctor of Medical Sciences Institute of Rheumatology RAMS, Moscow
Diagnostics
Treatment of knee arthritis is impossible without a preliminary examination and establishment of the etiology (cause) of the disease, since different types of arthritis require different approaches to treatment. As part of the examination, patients may be referred for the following studies:
- laboratory tests of blood, urine, joint fluid
- general clinical, biochemical, immunological, genetic, microbiological; - X-ray of the knee
- bone growths and deformations are identified, the height of the joint space is measured; - MRI of the knee
- changes in soft articular and periarticular tissues are detected; - Ultrasound
– examination of the soft tissues of the knee and determination of the volume of joint fluid; - arthroscopy
– endoscopic examination of the internal articular surface; If necessary, joint fluid is taken for examination.
Sodium hyaluronate
Being a glycosaminoglycan, one of the main components of connective tissues, it plays an important role in the proliferation of cells that determine their division and growth. Most often it can be found in the skin and bones, synovial fluid and intervertebral discs. Hyaluronate is part of the synoval fluid, providing support for knee mobility and reducing friction of the articular surfaces. It is actively used to treat diseases of the musculoskeletal system. It reduces pain and symptoms in general.
According to 2004 statistics, osteoarthritis caused moderate and severe disability in 43.4 million patients. Osteoarthritis of the knee and hip joint ranks 11th out of 291 in the world ranking of evaluated diseases.
Treatment of knee arthritis
Crunching in joints - when to worry
Intra-articular injections of hyaluronic acid
After a complete examination, treatment for knee arthritis is prescribed. It must be comprehensive and individually selected for a specific patient. The complex treatment includes:
- regimen and diet;
- drug therapy;
- non-drug methods for treating knee arthritis;
- folk remedies;
- surgical methods of treatment.
Regime and diet
When exacerbation of gonitis occurs, bed rest with minimal physical activity is applied. In some cases (for example, with purulent gonitis), the joint is immobilized. After the acute inflammation subsides, there is a gradual increase in physical activity. It is also important to regulate sleep and wakefulness patterns.
A special diet is only necessary for gout. Offal, meat of young animals, strong broths, eggs, alcoholic drinks, strong tea and coffee, and chocolate are excluded from the diet.
For other types of arthritis of the knee joint, during the treatment of exacerbations, a nutritious diet is recommended with the exception of foods that cause tissue irritation. These are onions, garlic, radishes, hot seasonings, fried, cooked, canned foods. It is also recommended to limit sweets and confectionery.
Drug therapy
The question of how to treat arthritis of the knee joint is decided by the attending physician. The general condition of the patient, features of the course of joint pathology, the presence of concomitant diseases, individual intolerance to drugs, etc. are taken into account. In this case, the doctor must adhere to common clinical recommendations for the treatment of certain types of gonitis. Prescribed:
- medications from the group of non-steroidal anti-inflammatory drugs (NSAIDs). They relieve symptoms of exacerbation of knee arthritis well: inflammation, swelling and pain, improve the general condition of the patient (Diclofenac, Nise, Miloxicam - in the form of injections, oral tablets or ointments);
- for severe swelling and pain that cannot be relieved by NSAIDs, glucocorticoid hormones are prescribed: a course of oral prednisolone, short courses of intravenous drip infusions of methylprednisolone (pulse therapy) or intra-articular injections of Diprospan;
- reduction of tissue swelling is achieved by the use of antihistamines - Erius, Claritin;
- for reactive arthritis against the background of a urogenital infection, long-term (up to a month) courses of antibacterial therapy are prescribed;
- Antibacterial therapy and washing the knee joints with antiseptic solutions are prescribed for the treatment of purulent arthritis of the knee joint;
- in order to restore cartilage tissue, chondroprotectors are prescribed - Dona, Structum;
- to suppress autoimmune processes, basic drugs are prescribed - Sulfasalazine, Methotrexate, Leflunomide, as well as biological substances or agents (MabThera),
Drugs for the treatment of knee arthritis
Non-drug methods
These treatments for knee arthritis include:
- physiotherapy - at the acute stage of the disease these are electrophoresis procedures with medicinal solutions, then magnetic and laser therapy, mud therapy, etc.;
- physical therapy (physical therapy) with a gradual increase in active physical activity during the period of remission;
- massage – during the period of remission, it allows you to restore blood circulation and stimulate metabolic processes in the knee;
- reflexology - influencing acupuncture points on the body, reflexively associated with the knee area; allows you to relieve pain, swelling, restore biological balance in tissues.
Folk remedies
Folk remedies for the treatment of knee arthritis can only be prescribed by a doctor. You cannot use them on your own, since different arthritis requires the use of different remedies. An infusion of medicinal herbs will be beneficial to one patient, but harmful to another. Most often, doctors use folk remedies to reduce the drug load on the patient’s body and limit the side effects of drugs.
Surgical methods of treatment
The help of a surgeon is required when conservative therapy does not help:
- in the treatment of purulent arthritis of the knee joint, therapeutic arthroscopy is performed with washing the diseased joint with aseptic solutions, constant drainage of the joint;
- in case of severe swelling and severe pain, a synovectomy operation is sometimes performed - removal of the most inflamed part of the synovial membrane;
- in case of deforming arthritis, the appearance of areas of bone tissue growth, in order to increase functionality, arthroplasty is performed - partial removal of bone growths and parts of the bones; in some cases, destroyed bone structures are replaced with implants;
- endoprosthesis replacement is a surgical intervention to replace a destroyed joint with an artificial one.
Surgical treatment of knee arthritis
Approach to treating the disease in our clinic
The Paramita clinic has developed a unified approach to the treatment of knee arthritis. It includes:
- Mandatory preliminary examination of the patient using the latest instrumental methods, including MRI.
- Individual approach to the treatment of each patient.
- Using two opposing approaches to treatment:
- Western
- based on the achievements of modern medicine with high results in the treatment of pathologies of various organs; this is the use of modern medications and treatment regimens, PRP therapy - stimulation of regenerative processes in the joints by administering the patient’s own platelet-rich plasma, diagnostic and therapeutic arthroscopy, etc.; - Eastern
- the traditional approach of doctors from China and Tibet, who consider the human body as a single whole, and the disease as an imbalance in the body; restoring balance leads to the elimination of pathology and overall improvement of the body; courses of acupuncture, moxotherapy, pharmacopuncture, herbal medicine, etc. are prescribed.
More detailed information about treatment methods at the clinic can be found on our website.
This approach to treatment allows the patient to quickly relieve pain, suppress the progression of the disease and restore joint function.
We combine proven techniques of the East and innovative methods of Western medicine.
Read more about our unique method of treating arthritis
Physiotherapy
Phonation
Vibroacoustic therapy involves the transmission of sound microvibration using a special medical device. It creates microvibrations that, with their physical characteristics, are identical to those created by muscle tissue under maximum static physical tension. In short, this therapy is a direct alternative to exercise.
Vitafon.
Phoning Effects:
- Improving lymph flow in the area of influence, which promotes accelerated tissue cleansing, has an anti-inflammatory effect.
- Improves blood flow and, accordingly, nutrition of the treated area.
- Has a beneficial effect on nerve pathways with prolonged exposure.
- Promotes the release of joint lubrication.
Galvanization and electrophoresis
The essence of the procedure is to activate the blood supply to joint tissues in chronic arthritis. Vasodilation occurs in the area of influence, increasing blood supply and improving recovery processes.
Electrophoresis.
UHF therapy
The affected joint is exposed to a continuous or pulsed electric field. For the knees, low-thermal doses are used at a current power of 20-30 W.
The procedure is aimed at reducing swelling, activating regenerative processes in the joint, improving nutrition and blood supply. The method allows you to achieve long-term remission.
Infrared laser therapy
Using a laser applicator, they act on biologically active points located along the lateral surfaces of the joint. The procedure activates blood flow, reduces pain sensitivity, and stimulates healing processes.
Ultrasound therapy
The method optimizes and accelerates the biochemical processes occurring in joint tissues, accelerates healing processes, and reduces swelling.
Hydrogen sulfide and radon baths, peloid therapy, massage, and manual therapy have also proven themselves well.
General clinical recommendations
Patients suffering from gonarthritis are recommended:
- avoid heavy physical activity and heavy lifting;
- lead a healthy lifestyle;
- do therapeutic exercises, swim;
- eat properly regularly;
- do not smoke, do not abuse alcohol;
- regularly carry out anti-relapse treatment courses recommended by your attending physician;
- promptly treat any acute and chronic diseases, foci of infection.
Prevention of knee arthritis
It is especially important for people at risk to follow preventive measures:
- athletes - avoid knee injuries, wear special knee pads;
- persons who have relatives suffering from rheumatoid, reactive, psoriatic, gouty arthritis should be attentive to their health and, if knee pain occurs, immediately seek medical help;
- promptly identify and treat all foci of infection - carious teeth, tonsillitis, sinusitis, etc.
Frequently asked questions about the disease
What is the difference between arthritis and arthrosis of the knee joint?
Arthritis is an inflammatory disease in which the tissues over the joint become red and swollen. Arthrosis is a metabolic disease accompanied by pain and joint deformation.
Best ointment for knee arthritis?
Many patients prefer Voltaren emulgel.
Which doctor treats knee arthritis?
Depends on the clinical form of arthritis. Purulent arthritis is treated by a surgeon, rheumatoid arthritis by a rheumatologist, psoriatic arthritis by a rheumatologist together with a dermatovenerologist.
The knee joint can be affected by any type of arthritis. Treatment of gonarthritis should begin as early as possible, before irreversible changes occur in the joint. But even if this happens, contacting the specialists of the Paramita clinic will relieve you of pain, stop the destruction of the joint and restore the joy of life.
Literature:
- Alekseeva L.A., Chichasova N.V., Mendel O.I. Results of using the drug Arthra for gonarthrosis // Scientific and Practical Rheumatology No. 5, 2005.
- Alekseeva E. I., Zholobova E. S. Reactive arthritis in children // Issues of modern pediatrics. 2003, vol. 2, no. 1, p. 51–56.
- Eid K.A. Injuries to the knee joint in children. Diagnosis and treatment using arthroscopy. Author's abstract. diss. Candidate of Medical Sciences – M. 2003. – 26 pages.
Themes
Arthritis, Joints, Pain, Treatment without surgery Date of publication: 10/20/2020 Date of update: 04/03/2021
Reader rating
Rating: 5 / 5 (1)
Alternative medicine
Alternative treatment will not replace medication. However, many patients tend to claim that, for example, acupuncture or reflexology helps reduce symptoms and side effects while taking medications.
It is important to note that treatment is most successful when the course begins early. Its goal is to reduce pain, support and improve skeletal functionality.
It is worth noting that you should not self-medicate. Contact a specialist, he will select the necessary medications for you according to your condition. He may also refer you to physical therapy.
Please note that walking for an hour or two in the fresh air will help prevent the disease. This is especially important with a sedentary lifestyle and low mobility. Do exercises in the morning; this will not only reduce the risk of illness, but also improve your well-being and give you strength for the whole day.