If a person ignores even the pronounced symptoms of gonarthrosis, then after a few months or years he is diagnosed with this pathology of the knee joint, grade 3 of severity. It is characterized by constant pain, aggravated by walking, and significant limitation of mobility. At the initial stage of therapy, conservative methods are used. As a rule, they are ineffective. Therefore, orthopedists immediately offer patients surgical treatment - endoprosthetics.
Features of grade 3 knee joint gonarthrosis
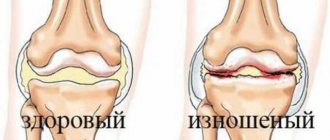
Gonarthrosis is a degenerative-dystrophic pathology that affects the knee joints. With grade 3 disease, clinical manifestations reach their maximum, including due to the development of complications. Most often, gonarthrosis is detected in women after the onset of natural menopause. But very young people often suffer from it, subjecting their knee joints to excessive stress. Stage 3 pathology is characterized by almost complete destruction of the cartilaginous layer of the knee, severe deformation of the femur and tibia.
Main symptoms
There are not many of them. The degree of manifestation directly depends on the age and stage of the disease.
- Crunching, creaking, clicking in the joint when moving.
- Pain in the knee and surrounding tissues when moving.
- Pain at rest.
- Muscle weakness and limited movement.
- Increase in joint size.
- Loss of fertility.
At the initial stage, the disease manifests itself as mild but noticeable pain and joint stiffness in the morning. The discomfort goes away as soon as the patient leaves. During the day, clicking in the knees and weakness in the limbs are observed.
Development mechanism
Initially, gonarthrosis affects hyaline cartilage. It becomes thinner, thicker, and less smooth. When sliding, the cartilage lining the bone surfaces now “clings” to each other, which further accelerates their destruction. The joint capsule gradually degenerates, and the synovial fluid thickens. Due to lack of nutrients, cartilage disappears from a large surface of the bones. Increasing loads leads to their deformation and pressing into each other. Multiple bone growths (osteophytes) are formed, constantly injuring soft tissues and synovial membranes.
Causes of health problems
Grade 3 gonarthrosis can be primary or secondary. In the latter case, its development is provoked by previous injuries (intra-articular fractures, dislocations, ruptures of kneecaps, ligaments, tendons) or pathologies already present in the body:
- rheumatoid, reactive, gouty, psoriatic arthritis;
- scleroderma, systemic lupus erythematosus;
- endocrine, metabolic diseases, including diabetes mellitus, hypothyroidism.
Primary gonarthrosis usually occurs against the background of natural aging of the body as a result of a slowdown in recovery processes. The prerequisites for it are increased stress, obesity, and a sedentary lifestyle.
Symptoms of pathology
Grade 3 gonarthrosis is characterized by constant pain that occurs both during the day and at night. Often, not only flexion at the knee joint is limited, but also extension. A person cannot fully straighten his leg, which pathologically changes his gait and posture. He shifts his weight to the healthy limb, limps, and leans in the direction opposite to the affected joint. In some cases, the legs become bent and hallux valgus or varus deformity occurs. The patient's movement is often only possible with the help of a cane, walker, or crutches.
Disability
In order to determine whether a person needs to be given a disability, one must first diagnose what stage the disease is at.
A person is recognized as able to work in the following cases:
- if the changes are minor or moderate;
- the disease is accompanied by various disorders of static-dynamic functions, but the course of gonarthrosis is slowly progressive.
Disability of the third group is given to people in the following cases:
- if a moderate impairment of motor function is diagnosed;
- if a person performs work that involves significant physical activity;
- if a person is forced to constantly be on his feet;
- if there is a pronounced violation of the static-dynamic function.
There are certain situations in which patients with gonarthrosis will be sent to undergo a disability commission:
- if the progression of the disease lasts for three years or longer, with exacerbations occurring at least three times during the year;
- if the patient underwent surgery to treat arthrosis of the knee joint, as a result this significantly affected his ability to work;
- in case of violation of the musculoskeletal function of a limb, if this process is pronounced.
During the commission, the patient's medical history is studied. The person’s complaints must be taken into account and the clinical picture is assessed. The patient must show how able he is to work. Disability of the second and third groups is confirmed once a year, and the first group must be confirmed once every two years.
Diagnosis of the disease
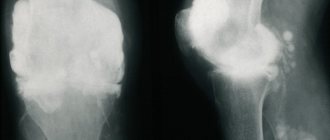
The diagnosis is made based on medical history, patient complaints, and external examination. With grade 3 gonarthrosis, the knee is deformed and enlarged. Synovitis often accompanying the pathology leads to its smoothing due to the formation of inflammatory edema. Of the instrumental studies, the most informative are radiography and MRI. According to indications, arthroscopy is performed - examination of the internal surfaces of the joint.
How to treat grade 3 knee gonarthrosis
Conservative treatment of grade 3 gonarthrosis is aimed at eliminating pain, muscle spasms, and stiffness. An integrated approach to therapy helps prevent the involvement of healthy tissues and joints in the destructive and degenerative process. Patients are recommended to reduce the load on the affected joint by using semi-rigid elastic knee pads. During the treatment period, you are allowed to move only with a cane or crutches.
Drug therapy
Despite the fact that it is impossible to eliminate severe deformations of bone and cartilage structures with the help of medications, they are necessarily used in the treatment of grade 3 gonarthrosis. The use of drugs can eliminate the symptoms of the disease and slow down its progression.
Glucocorticosteroids
Glucocorticosteroids are synthetic analogues of hormones produced by the adrenal glands. The drugs have a powerful analgesic and anti-inflammatory effect, therefore they are used to relieve acute pain. In the treatment of gonarthrosis, intra-articular or periarticular administration of glucocorticosteroids is practiced - Methylprednisolone, Dexamethasone, Triamcinolone, Diprospan. Hormonal agents are often combined with the anesthetics Novocaine and Lidocaine.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs are the first choice drugs in the symptomatic treatment of grade 3 gonarthrosis. They quickly eliminate pain, reduce elevated local temperature, and relieve inflammation during relapses of synovitis. NSAIDs are used in the form of solutions for intramuscular administration (Movalis, Xefocam), tablets (Nimesulide, Diclofenac), ointments and gels (Voltaren, Fastum). Systemic drugs are combined with proton pump inhibitors to prevent ulceration of the gastric mucosa.
Chondroprotectors
This is the name of drugs in various dosage forms intended for the partial restoration of cartilage tissue. In case of grade 3 gonarthrosis, they are not used for this purpose due to the complete destruction of the cartilaginous layer of the knee. Chondroprotectors are used to improve metabolism in the joint and prevent further bone deformation. As they accumulate in articular structures, they also have a pronounced analgesic effect. Most often, Alflutop, Chondroguard, Structum, Teraflex, Artra, Dona are included in therapeutic regimens.
Muscle relaxants
In response to pain and pinched nerve endings, muscle spasms may occur. By restricting mobility, the body tries to solve problems. But more often, an increase in the tone of skeletal muscles leads to even greater compression of the nerves and increased pain. In such cases, patients are prescribed muscle relaxants Sirdalud, Baklosan, Mydocalm. First, the drugs are used in the form of injection solutions, and then the result is secured by taking tablets.
Surgical intervention
For grade 3 gonarthrosis, orthopedists immediately offer patients surgical treatment so as not to waste time on futile drug therapy. The most popular endoprosthetics is the replacement of the knee joint with an artificial implant. The operation is performed under general anesthesia or epidural anesthesia, after which long-term (3-4 months) rehabilitation begins. Endoprosthetics is the only treatment method for gonarthrosis that allows the patient to lead an active lifestyle.
Knee arthroscopy
Arthroscopy is an endoscopic operation using miniature surgical instruments. They are introduced into the cavity of the knee joint through several punctures of the skin and underlying soft tissue. The progress of the operation is monitored on the monitor screen, the image to which is transmitted from a video camera built into the endoscopic device. The surgeon performs partial resection of bone tissue, plastic surgery of ligaments and tendons, and removal of cartilage particles moving freely in the articular cavity. But arthroscopy can only improve knee function for a short time.
Corrective osteotomy
Corrective osteotomy is a surgical operation aimed at eliminating joint deformity through an artificial fracture. Dissection of the tibia and femur with further comparison of fragments at a certain angle contributes to the correct distribution of loads. To stabilize during movement, at the final stage of osteotomy, the leg is fixed with special metal structures.
Arthrodesis
Arthrodesis is artificial ankylosis, immobilization of a joint in a functionally advantageous position. The surgeon performs fusion of the kneecap, tibia and femur. After surgery, the knee loses the ability to bend and straighten. But the patient remains able to move independently using a cane or walker.
Arthroplasty
Arthroplasty is an operation aimed at restoring the size, shape and conformity of joint surfaces to each other. First, the surgeon disconnects the adhesive that immobilizes the knee. Then he excises the osteophytes, restores the shape of the articular surfaces, and installs an insulating autoplastic (from fascia, skin, adipose tissue) or alloplastic (from acrylate, stainless metals) spacer between them.
PRP therapy in orthopedics
PRP therapy is the introduction of autologous plasma with an increased concentration of platelets into the cavity of the knee joint. The therapeutic effect of the procedure is due to the presence of growth factors in the patient’s own plasma. These bioactive substances have a stimulating effect on cell division, intercellular metabolism, and hyaluronate synthesis, which promotes accelerated restoration of the soft tissue structures of the knee joint.
Physiotherapy
At the stage of exacerbation of grade 3 gonarthrosis, patients are shown electrophoresis or ultraphonophoresis with glucocorticosteroids, anesthetics, and B vitamins. After eliminating severe pain, laser therapy, magnetic therapy, shock wave therapy, and UHF therapy are performed. The main goal of physiotherapy is to reduce the severity of symptoms and increase the body’s sensitivity to the effects of pharmacological drugs.
Massage and manual therapy
Sessions of classical, vacuum, acupressure help strengthen the muscles of the leg affected by gonarthrosis. Blood circulation in the joint improves, the removal of tissue breakdown products from it is accelerated, and destructive processes are inhibited. Unlike a massage therapist, who treats only weakened or spasming muscles, a chiropractor works on joint structures. The result is an increase in the distance between them, eliminating compression of blood vessels and sensitive nerve endings.
Exercise therapy complex
Daily physical therapy exercises can reduce the dose of systemic medications. This occurs by strengthening the muscle frame of the knee and improving the blood supply to its structures with nutrients. A set of exercises is compiled by a physical therapy doctor individually for each patient, taking into account age, severity of symptoms, and degree of immobility of the knee joint.
| Physical therapy exercises for grade 3 gonarthrosis | ||
| Lying on your back | Sitting on a chair | In a standing position with support on the back of a chair |
| Alternately pulling the bent right and left knees to the chest | Alternating lifts of first straight and then bent legs | Abduction of first straight, then bent legs to the right and left |
| Simulation of cycling | Leg extensions holding them at the top for a few seconds | Alternately raising straight legs as high as possible |
| Crossing straight legs (“scissors”) | Rotation of the feet first in one direction, then in the other direction | Smooth rolls from toe to heel and back |
Diet therapy
For overweight patients, orthopedists recommend losing weight to reduce the load on all joints of the legs. It is necessary to exclude from the daily menu foods high in fat and simple carbohydrates - confectionery and sausages, fatty meats, smoked meats, semi-finished products, and baked goods. The basis of the diet should be clear broths, puree soups, fresh or stewed vegetables, baked chicken, beef, rabbit, cheeses, cottage cheese, dried fruits.
Application of traditional medicine
Medicines prepared according to traditional medicine recipes are not used in the treatment of grade 3 gonarthrosis due to ineffectiveness. It is possible to use herbal teas with St. John's wort, valerian, motherwort to improve the quality of sleep.
General information
Currently, diseases of large joints of degenerative-dystrophic origin occur in about 10% of the world's population. At the same time, this pathology more often “affects” the knee joint. Gonarthrosis (in the literature there are synonyms for this disease - osteoarthrosis, arthrosis deformans, degenerative arthritis, osteoarthritis/hypertrophic arthritis of the knee joint) is a polyetiological degenerative-dystrophic disease characterized by damage/destruction of articular cartilage, subchondral layer of bone and adjacent periarticular tissues: muscles, ligaments , menisci and synovium (Fig. below).
The disease is accompanied by deformation of cartilage/bone formations, the formation of osteophytes and gradual defiguration of the knee joint and limb. It manifests itself clinically as pain/restriction of movement in the joint. ICD-10 code: M17.
In the structure of the knee joint, the medial/lateral side of the tibiofemoral (tibiofemoral) section and the patellofemoral (patellofemoral) section are distinguished. The tibiofemoral region is most susceptible to the effects of osteoarthritis, its medial side (affected in 75% of patients), and the lateral side of the tibiofemoral region in 26% of patients. While the patellofemoral region in patients is affected in 48% of cases. Osteoarthritis of the patellofemoral joint is common mainly in people over 55 years of age. However, in this case, damage to the patellofemoral part of the knee joint is accompanied by a several times higher risk of disability compared to damage to the tibiofemoral part.
According to various authors, deforming osteoarthritis of the knee joint occurs in 10-15% of the population, while symptomatic gonarthrosis in persons under 40 years of age occurs in 5% of the population; after the age of 45 years – in 18%, and after 60 years – in 42.8%. The predominance of the disease among females is characteristic. In recent years, there has been a clear trend towards rejuvenation of gonarthrosis, especially among people of working age leading an active lifestyle and athletes. In practice, predominantly bilateral gonarthrosis occurs, i.e., combined left-sided/right-sided gonarthrosis and does not depend on the factor of the dominant/non-dominant limb. Idiopathic left-sided gonarthrosis and right-sided gonarthrosis (according to ICD-10: M17.0) occur in patients in approximately equal proportions.
Gonarthrosis, as a rule, is accompanied by a pronounced decrease in the level of physical activity, which contributes to an increase in body weight and the risk of developing heart disease. Many patients with persistent dystrophic changes in the joints lose the ability to carry out elementary/simple movements. Anticipation/fear of pain, joint hypermobility/contracture make it difficult to walk, sit down, turn in bed, or get out of a chair/bed.
At the same time, the rapid progression of gonarthrosis is accompanied by a significant risk of temporary/permanent disability, and late diagnosis and lack of timely treatment can lead to disability and a significant decrease in quality of life. Accordingly, the problem of effective treatment of gonarthrosis has both medical, social and economic significance.
Rehabilitation after surgical treatment
At the initial stage of rehabilitation, patients are prescribed antibiotics, anticoagulants, and hepatoprotectors to prevent postoperative complications. 2-3 days after installation of the endoprosthesis, you are allowed to stand up and walk around the ward and hospital corridor on crutches. Daily physical therapy exercises under the guidance of a rehabilitation physician are required. After endoprosthetics, patients are advised to undergo sanatorium-resort treatment to accelerate the restoration of joint function. Applications with ozokerite and paraffin, mud, mineral waters, hydrogen sulfide, radon, and pearl baths are used.
Consequences and prognosis
The course of grade 3 gonarthrosis is complicated by spontaneous hemarthrosis, the development of secondary reactive synovitis, and external subluxations of the patella. But the most serious consequence is ankylosis. The joint space is completely fused and the knee is immobilized. This leads to disability of the patient due to the inability to move independently. This development of events can only be avoided by knee replacement.
List of sources
- Loginov S.I., Solodilov R.O. The influence of gonarthrosis on the kinematics of the knee joint. Bulletin of Siberian Medicine. 2016;15(3):70-78.
- Kashevarova NG, Alekseeva LI, Anikin SG, et al. Osteoarthritis of the knee joints: risk factors for the progression of joint disease in a five-year prospective disease. Materials of the III Eurasian Congress of Rheumatologists, (Minsk, Republic of Belarus, May 26-27, 2021). Issues of organization and informatization of healthcare. 2021.
- Kosareva M.A., Mikhailov I.N., Tishkov N.V. Modern principles and approaches to the treatment of gonarthrosis // Modern problems of science and education. – 2021. – No. 6.
- Bagirova G.G. Osteoarthrosis: epidemiology, clinic, diagnosis, treatment / Bagirova G.G., Meiko O.Yu. - M., 2005. - 224 p.
- Badokin V.V. Main symptom-modifying slow-acting drugs in the treatment of osteoarthritis // Breast Cancer. 2011. No. 12. pp. 72–79.