What is gangrene?
Gangrene is a disease characterized by the death of living human tissue as a result of infectious diseases or impaired blood supply.
Fournier's gangrene, epifascial necrosis or gangrenous form of erysipelas is a variant of gangrene that is a rapidly progressing infection that destroys the tissue of the genital organs and surrounding areas. Without early emergency care, in more than 20% of cases, such gangrene leads to the death of a person, even with subsequent adequate treatment.
The gangrenous form of erysipelas is one of the rare diseases. According to statistics, it occurs with a frequency of 1:7500 of the population. The majority of patients are men over 60 years of age. In women, pathology is observed 5-10 times less often. Isolated cases in children, including newborns, are also recorded [1].
Rehabilitation therapy and rehabilitation
After surgical opening of the phlegmon, ointments, antibiotics and therapeutic techniques are prescribed that help remove residual pus from the wound and quickly cleanse the skin. Among products with herbal ingredients, preference is given to sea buckthorn oil, rosehip extract and Troxevasin ointment. If the wound does not heal for a long time and the skin does not tighten, the patient is prescribed dermoplasty.
Dermoplasty is a skin graft that is performed in case of severe damage to the dermis during trauma and extensive surgery. When removing phlegmon, this operation is prescribed in the case of removal of extensive inflammatory foci in which soft tissue necrosis has begun. In addition to the use of local remedies that promote rapid recovery and healing of the wound, the patient is prescribed conservative treatment methods aimed at restoring the immune system, relieving intoxication and preventing re-inflammation.
Bed rest is mandatory throughout the entire rehabilitation period. The area of the body where surgery was performed should be in a slightly elevated position. If there is pain, painkillers are prescribed and injected into the muscle.
All patients who have undergone surgery to remove cellulitis must take a course of antibiotics. The medications are prescribed by the attending physician depending on the individual characteristics of the patient and the type of virus that provoked the inflammation. If anaerobic cellulitis has been removed, intramuscular injections of anti-gangrenous serum are prescribed. To restore and normalize the acid-base balance, a solution of methenamine is prescribed. To restore tone to the walls of blood vessels, calcium chloride in solution is used.
To relieve the effects of intoxication and restore the functioning of the heart muscle and circulatory system, adonylene and caffeine are prescribed. Patients need to adhere to proper nutrition, it is imperative to exclude fatty and fried foods, and it is not recommended to consume large amounts of flour. Be sure to drink plenty of plain water; fruit compotes and fruit drinks are allowed to restore the immune system. Antibiotics are used until the inflammatory process is completely removed.
Causes
The disease is secondary in nature, developing against the background of inflammatory diseases of the organs and structures of the pelvic region that a person already has. The development is based on a purulent process, blockage of small vessels of the skin and subcutaneous fatty tissue by microthrombi.
Among the pathogens most often identified are: Klebsiella, streptococci, staphylococci, clostridia, bacteroides and corynebacteria, pseudomonads, fungi of the genus Candida. On average, at least 3 pathogens are simultaneously detected in patients [2].
Primary pathologies most often are:
- Acute and chronic urogenital infections.
- Injuries to the perineum and genitals.
- Previous surgical interventions on the pelvic organs, especially those requiring long-term catheterization of the bladder.
- Inflammatory diseases of the rectum and other parts of the intestine.
- Inflammation of the genital organs, including prostatitis, epididymitis, orchitis.
- Purulent infections of the skin and subcutaneous fat in the genital area.
- Cancer of the distal gastrointestinal tract.
- Genital piercing performed without observing the rules of asepsis and antisepsis.
Piercing or tattooing in the genital area can provoke Fournier's gangrene if aseptic rules are not followed in the salon.
Photo: freepik - ru.freepik.com In women, the causes of the development of Fournier’s gangrene are gynecological diseases, complications of pregnancy and childbirth [3]:
- Vulvitis is inflammation of the external genitalia.
- Septic abortion is an abortion that results in infection of the birth canal and uterus.
- Complications after hysterectomy - removal of the uterus.
- Infection of a wound due to a rupture of the perineum during childbirth or episiotomy - a dissection of the perineum and the posterior wall of the vagina.
The development of epifascial necrosis in infancy and childhood is often associated with the following factors [3, 4]:
- Circumcision.
- Strangulated inguinal hernia.
- Insect bites.
- Generalized infection, sepsis.
- Severe burns of the genitals.
Fournier's gangrene itself, despite its infectious origin, does not belong to the category of infectious diseases. However, the theoretical possibility of transmitting the causative agent of the primary pathology (bacteria or fungus) remains, since with the development of gangrene an open wound is formed. Direct contact of discharge from a wound with damaged areas of the skin or mucous membranes can lead to the development of an infectious disease [3].
Risk factors
Often, pathology develops in the presence of diseases or pathological conditions that further reduce the body's resistance to infection. The main risk factors are [3, 4]:
- HIV infection and AIDS.
- Autoimmune diseases, including systemic lupus erythematosus and Crohn's disease.
- Long-term treatment with glucocorticosteroids and immunosuppressants.
- Malignant tumors and their treatment: chemotherapy, radiation therapy carried out in the pelvic organs.
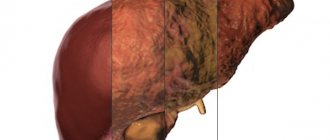
- Liver diseases, cirrhosis.
- Alcohol abuse.
- Severe obesity.
- Elderly age.
Pathogenesis
A certain importance in the pathogenesis of FD is attached to the anatomical features of the external genitalia:
- the epithelial cover is loose;
- the epidermis layer is thinner than on other parts of the skin;
- subcutaneous tissue is poorly developed and is represented by loose adipose tissue;
- in the thickness of the skin there is a significant number of sebaceous and sweat glands;
- There are hair follicles on the skin of the perineum and scrotum.
All of these factors create favorable conditions for the persistence of various microbiological agents. The blood supply to the scrotum is represented by a dense venous and scanty arterial network. With inflammation and edema, conditions are created to slow down venous blood flow, intravascular stasis and thrombophlebitis, which further impairs the blood supply to the organ and leads to ischemia of the affected tissues. The pathological process spreads along the fascia - superficial and deep, causing vascular thrombosis with subsequent gangrene of the skin. Morphologically, a picture of purulent inflammation with areas of necrosis, edema with leukocyte infiltration and the formation of microabscesses is found in the membranes of the scrotum.
Also, predisposing factors are some concomitant diseases: diabetes mellitus, obesity, cirrhosis of the liver, vascular pathology of the pelvic area, malignant tumor, alcoholism, drug addiction, taking glucocorticoids, condition after chemotherapy, nutritional deficiency.
Most often, the causative agents are streptococci, staphylococci, fusobacteria, spirochetes and other associations of anaerobic and aerobic bacteria. Polymicrobial etiology leads to a synergistic interaction of enzymes and toxins and the rapid spread of infection in tissues.
In 2006, at the annual Historical Clinicopathological Conference at the University of Maryland medical school, Dr. Hirschmann suggested that the Jewish king Herod the Great suffered from kidney failure and Fournier's disease in the last years of his life. His conclusions are based on a description of the king’s life made by biographer Josephus based on the memoirs of Nicholas of Damascus 75–100 years after the death of Herod. Herod suffered from fever, itching of the skin of the whole body, abdominal pain, shortness of breath, swelling and cramps in the lower extremities and gangrene of the genitals.
Why is Fournier's gangrene dangerous?
Despite modern approaches to diagnosis and treatment, the availability of high-quality antimicrobial drugs, this pathology still has a high mortality rate due to severe tissue necrosis, the spread of tissue breakdown products and bacterial activity into the systemic bloodstream, followed by multiple organ failure.
There are also a number of long-term complications for people who have had Fournier's gangrene. These include [6]:
- Chronic pain in the area of affected organs and structures.
- Deformation of the genital organs.
- Loss of sensitivity of the skin of the genital organs and pain during erection.
- Temporary stool incontinence.
All of the above factors lead to sexual dysfunction. Also, after surgical treatment, in the presence of extensive scars, patients experience psychological and physical discomfort and a general decrease in quality of life.
Complications of cellulitis
Purulent-necrotic phlegmon of the leg in the process of cleansing the wound surface and forming granulations.
The main ones are:
- gangrene,
- sepsis,
- thrombosis of arteries and veins of the lower extremities, mesenteric vessels,
- abscesses of the liver, kidneys, spleen, respiratory organs, lungs, brain,
- thromboembolism of small and large branches of the pulmonary artery,
- multiple organ failure.
Purulent-necrotic phlegmon of the back
With a progressive disease, pus accumulates in the deeper layers of the skin, causing the development of inflammation of the surrounding tissues, affecting the blood and lymphatic vessels and nerves.
Cellulitis of the posterior thigh
Symptoms
The initial stages of development and clinical signs of Fournier's gangrene can vary from an almost asymptomatic debut to a rapid, lightning-fast course with pronounced local manifestations.
The leading symptoms of the disease most often are:
- Redness, pain and swelling of tissue in the genital area. Most often they are the first manifestations of the disease.
- Reddish-purple or blue-gray spots on the skin of the genitals, perineum, pubic and anal areas, followed by black areas of necrosis.
- A pungent putrid odor that occurs as the affected tissues decompose.
- Crepitation is a characteristic crunching sound that occurs when tissue is pressed in the area of necrosis.
- Purulent discharge from the genitals, formed wounds.
The disease is also accompanied by a general intoxication syndrome, which includes the following symptoms:
- Increased body temperature above 38°C.
- Cardiopalmus.
- General weakness, malaise.
- Headache.
Stages of the disease
Fournier's gangrene in its development goes through 4 successive stages:
Signs and symptoms of the disease in the prodromal stage
It is almost impossible to diagnose Fournier's gangrene in the prodrome stage. Patients report discomfort, fever and weakness. They associate their condition with diseases such as prostate adenoma, hemorrhoids, hematoma or scrotal boil and are in no hurry to seek medical help. The duration of the prodromal stage is 1–12 days.
Signs and symptoms of the disease in the early stages
The early or pre-gangrenous stage of Fournier’s gangrene develops rapidly and lasts from the first 10–12 hours to 4–5 days. This period is characterized by the predominance of aerobic flora in the lesions.
Initially, the superficial fascia of the scrotum and perineum is affected. The inflammation is characterized by diffuse necrotizing fasciitis. Further, at a speed of 2 - 3 cm/hour, the pathological process spreads along the fascial sheaths to neighboring areas - the thighs, the anterior abdominal wall and buttocks. Swelling and erythema of the scrotum and penis appear. Somewhat later, intense pain appears in the area of the entrance gate. Necrosis spreads from the depths of the tissue outward. Later (in the late stage), necrotizing cellulitis and dermatitis develop.
The pain syndrome is pronounced. Its intensity is incommensurate with the affected area and is not controlled by conventional analgesics. Pain extends beyond the anogenital zone.
The swelling increases quickly. The penis and scrotum increase significantly in size. The swelling reaches its maximum size on days 2–3 of illness.
During the first 12–14 hours, the skin of the external genitalia becomes bronze in color. In half of the cases, the skin of the scrotum acquires a “woody” density; with the same frequency, bullae (bubbles) form on the skin, which quickly undergo necrosis and burst, releasing a secretion of a serous-hemorrhagic nature and an unpleasant odor.
Fournier's gangrene in the early stages should be distinguished from a number of skin, venereological, surgical and infectious diseases. Reliable differential diagnostic signs are:
- Severe pain with an intensity incommensurate with the affected area, which is not relieved by conventional analgesics.
- Rapid, despite the treatment, progressive course with the subsequent development of infectious-toxic shock.
Rice. 6. Edema, erythema and emerging zone of necrosis (indicated by an arrow) with Fournier’s gangrene.
Signs and symptoms of advanced disease
The late stage of Fournier's gangrene develops rapidly and lasts from over 12 - 14 hours to 4 - 12 days. This period is characterized by the predominance of anaerobic flora in the lesions, which is characterized by intense gas formation, which is manifested by symptoms of crepitus. Subcutaneous emphysema develops.
The patient's condition progressively worsens, symptoms of sepsis appear and increase, even despite intensive antibiotic therapy. Patients are worried about headache, high body temperature, repeated frequent chills, shortness of breath and palpitations. Infectious-toxic shock develops quickly.
The development of necrosis is indicated by the appearance of dark blue or black spots on the skin of the scrotum or penis. Visible areas of necrosis are much smaller than areas of necrosis of the fascia and subcutaneous fat tissue (the “iceberg” phenomenon). Subcutaneous emphysema and necrosis are absolute indications for surgical intervention - revision of affected areas and sanitary necrectomy.
Due to the destruction of nerve endings, the intensity of the pain syndrome decreases.
Swelling of the scrotum and penis in some cases causes difficulty urinating and even acute urinary retention.
Swelling and gas formation in a closed tissue space worsen the already impaired blood circulation, which contributes to the progression of purulent-necrotic processes. A secondary infection occurs. The pathological process involves the tissues of the perineum, inner thighs and pelvic organs.
On days 7–8 of the disease, a line of demarcation appears around areas of necrosis. The process of rejection of the dead areas of the scrotum begins, which is accompanied by the formation of a large amount of dirty gray color with a fetid odor of purulent discharge and gas bubbles. On days 10–12, the rejection process ends. The testicles turn out to be naked, have a bright red color and appear to be suspended on the spermatic cords. The testicles and spermatic cords, as a result of separate blood supply, remain unaffected by the pathological process.
Rice. 7 and 8. Advanced stage of Fournier’s gangrene. Appearance of the genital organs. In the photo on the left is necrosis of the penis, on the right is the scrotum.
Reparative stage
If the outcome of Fournier’s gangrene is favorable, which is extremely rare, the reparative stage begins on days 12–14 of the disease. The patient’s well-being begins to improve: chills and pain disappear, body temperature and blood cellular parameters normalize. Tissues undergo regeneration and granulation tissue develops. With deep damage, scars form, leading to deformation of the genitals. The duration of the repair stage varies and depends on a number of factors, generally ranging from 2 – 3 weeks to several months. 30% of patients require constant care after discharge from the hospital, 50% require reconstructive plastic surgery.
With an unfavorable outcome of Fournier's gangrene, which occurs much more often, there is a progressive deterioration in the patient's condition from the very beginning of the disease. Toxic encephalopathy, oliguria and sepsis develop.
Diagnostics
In most cases, the diagnosis of Fournier's gangrene is made based on the symptoms present. However, in the early stages of development, laboratory tests and hardware imaging methods are also necessary to identify the type of infection, study the risks and predict complications.
Laboratory diagnostics
Involves routine tests (complete blood count, urinalysis), a number of biochemical blood parameters (creatinine, electrolyte composition, glucose, etc.), and assessment of blood clotting.
Also, in order to identify the causative agent of the infectious process, bacterial culture of blood and urine is performed [5] followed by an antibiogram. The latter consists of determining the sensitivity of identified microorganisms or fungi to the main groups of antimicrobial drugs, which makes it possible to select the most effective medications for treatment.
Hardware research methods
MRI is one of the methods for diagnosing gangrene.
Photo: US Navy photo / DVIDS The purpose of their implementation is to determine the volume of affected tissues and the involvement of adjacent organs and anatomical structures in the pathological process. Depending on the situation, [5] can be used:
- X-ray of the pelvic organs.
- Ultrasound echography.
- Computer (CT) and magnetic resonance imaging (MRI).
Forms of inflammation
With the development of phlegmon, the inflammatory process goes through several stages of formation. The initial stage is serous. With serous phlegmon, fluid—exudate—forms and accumulates under the skin, and leukocytes penetrate into the cells of the adipose tissue. Fatty tissue takes the form of jelly, completely saturated with exudate. There is a gradual spread of inflammation to healthy areas of soft tissue. If treatment is not carried out at this stage, the phlegmon passes into the next stage, putrefactive or purulent. It depends on what type of pathogenic microflora led to inflammation.
The purulent form provokes histolysis (in which the tissues melt and fill with pus). Due to histolysis, fluid begins to accumulate and may be greenish, cloudy white or yellow. The purulent type of neoplasm can lead to ulcers and fistulas. Without timely treatment, inflammation of purulent masses spreads to healthy tissue, cartilage and bones. At this stage of development of the inflammatory process, the muscles become loose, completely surrounded by pus, and appear gray and dirty. There is no internal bleeding.
The putrefactive form of phlegmon is characterized by rapid infection of soft tissues, which begin to deteriorate, and an unpleasant odor emanates from them. The tissues become brownish or greenish, their consistency is slippery and loose. With further development of phlegmon, soft tissues turn into a solid liquid mass. The main symptom of the putrefactive form of inflammation is severe intoxication of the body with a rapid deterioration in the patient’s condition.
Necrotic phlegmon is the death of destroyed soft tissues that are completely affected by purulent masses. If the tissues do not melt on their own, the body begins to reject them. At this stage of development of phlegmon, the inflammatory process begins to localize, multiple foci of abscess are formed, which can be opened independently. If there is too much accumulation of purulent masses that are deep under the skin, it is necessary to surgically open them and install drainage.
Anaerobic is the most severe stage of phlegmon, in which purulent masses infect adjacent healthy tissues, leading to their death, and gas is released. The fabrics have a fetid odor and are dark gray in color. If you press on the phlegmon, you can hear a crunch with which gas bubbles burst. The skin surrounding the source of inflammation becomes soft and loose, there is no redness.
Possible complications
Cellulitis is an extremely dangerous condition of the body, which without proper treatment can lead to severe intoxication and death of large areas of soft tissue. Chronic phlegmon is characterized by the absence of pronounced symptoms. The slow growth of pathogenic microflora allows the body to fight inflammation. During an exacerbation, a thickening occurs under the skin caused by the accumulation of infiltrate, which becomes woody. The skin around the inflammation becomes bluish.
The development of phlegmon on the lymph nodes is especially dangerous. This condition is fraught with the development of blood clots and sepsis. If the inflammatory process has not been completely treated and a small amount of pus remains on the soft tissues, a repeated purulent abscess may occur. Cellulitis that occurs on the face can lead to purulent meningitis.
cellulitis of the century
With further development of phlegmon, during which healthy tissues are affected, purulent arthritis, pleurisy, and osteomyelitis may occur. The most severe complication is the development of purulent arteritis, in which inflammation of the walls of large blood vessels - arteries - occurs, as a result of which the vessel begins to stratify and disintegrate. This pathological process can lead to severe internal bleeding.
Treatment
The treatment of epifascial necrosis is based on urgent surgical debridement of all necrotic tissue and high doses of broad-spectrum antibiotics. If necessary, they are supplemented by intravenous administration of plasma substitutes, blood transfusions and other emergency measures.
Broad-spectrum antibiotics
Antibacterial therapy begins from the moment of diagnosis. When choosing a treatment regimen, we are guided by the need to cover as many infectious agents as possible: bacteria, pathogenic fungi and protozoa.
The most commonly used is classical triple therapy, including cephalosporins (ceftriaxone, cefatoxime) or third-generation aminoglycosides (amikacin), as well as penicillin and metronidazole. Carbapenems (meropenem) may also be prescribed [5].
Local treatment
Locally, the necrosis zone can be treated with antiseptic solutions (sodium hypochloride, hydrogen peroxide) as well as enzymatic preparations (lyophilized collagenase) [8]. This treatment is aimed at preventing the spread of necrosis and additional infection of the affected tissues.
Hyperbaric oxygen therapy
Hyperbaric oxygen therapy involves placing the patient in an environment with increased atmospheric pressure while inhaling 100% oxygen (Fig. 1). This treatment enhances the immune response in the area of necrosis, prevents breakdown products from entering the systemic circulation and enhances the effect of some antibiotics from the cephalosporin and aminoglycoside groups [9].
Figure 1. Hyperbaric oxygen therapy. Source: Cleveland Clinic Martin Health / YouTube
Surgery
With Fournier's gangrene, removal of all dead tissue as quickly as possible is indicated. As a rule, wound sanitation is carried out in several stages. If the pathological process spreads to the scrotum, the testicles are also removed, but this rarely happens.
In cases of severe damage to the perineum and anal sphincter with concomitant fecal incontinence, colostomy is indicated, although this is associated with additional risks for the patient [7]. Colostomy is a surgical procedure in which an opening is created in the anterior abdominal wall to drain stool from the small intestine. Special rectal catheters can also be used (Fig. 2).
Figure 2. Rectal drainage device, Flexi-weal Fecal Management System. Source: ResearchGate (Creative Commons Attribution 3.0 Unported)
In order to correct the cosmetic defect, patients in the future undergo plastic surgery with skin grafting, reconstruction of the penis and scrotum [10].
The publication
In 1764, the German physician Baurienne described a case of fulminant gangrene of the scrotum in a 14-year-old boy after injury. In Russian literature, FD was first described in 1862 by the Russian surgeon P. Dobychin. And in 1865, the Russian anatomist and surgeon Ilya Buyalsky published a report on the successful treatment of a patient with gangrene of the scrotum with complete exposure of the testicles and spermatic cords.
Later, many doctors mentioned FD due to injury. Only in 1883, the Parisian dermatovenerologist Jean Alfred Fournier observed four cases of this disease and for the first time described it as an independent nosological form - “spontaneous fundurant gangrene of the scrotum” (“gangrene foudrayante de la verge”), i.e. idiopathic.
The modern definition of FD implies acute necrosis of the tissues of the penis and scrotum, less commonly the genital organs of women, caused by the spread of anaerobic infection from the urinary tract or pararectal area.
Jean Alfred Fournier (1832–1914) headed the Hospital. St. Louis (Paris) from 1860 to 1902. In addition to his clinical activities, he lectured at the medical faculty of the University of Paris. In 1883, at a lecture, he cited cases of genital gangrene in young healthy men. Fournier assigned a large role to injury as a predisposing factor to the development of the disease.
Prognosis and prevention
Fournier's gangrene is often fatal. It is estimated that this is from 20 to 30% of cases. The most common causes of death are: spread of infection into the bloodstream (sepsis), kidney failure or multiple organ failure. More than 50% of surviving patients continue to have severe pain in the affected area in the future.
Prevention involves early diagnosis and treatment of diseases that could potentially lead to the development of gangrenous changes, as well as appropriate therapy for immunodeficiency conditions.
Basic tips include the following actions and recommendations:
- Correction of body weight in obesity.
- Comprehensive treatment and control of blood glucose levels for diabetes mellitus in combination with regular examination of the genitals.
- Quitting drinking alcohol and smoking.
- Minor wounds, damage to the skin and genitals should be treated with antiseptic solutions and kept dry and clean until healing. If serious injuries occur, seek immediate medical attention.
Clinical case
In 2012, in the journal Case Reports in Emergency Medicine, Dr. Jason Hayner and his colleagues described the case of a surprisingly unlucky 29-year-old man. He presented to the emergency department with a two-day history of fever, vomiting, and diffuse myalgias. When taking his medical history, he admitted that he was also bothered by swelling and pain in the scrotal area, and said that he often masturbates with soap as a lubricant, and therefore his penis and scrotum often turn red. On examination, the patient has severe redness and swelling of the penis and scrotum, covered with a foul-smelling scab. The patient denied any injuries or chronic diseases of the genitourinary system. The symptoms have been increasing for the last three days, after masturbation. In the emergency room, swelling and redness of the scrotum were detected, spreading to the pubic symphysis; body temperature was 40.0 °C, blood pressure was 87/50 mm Hg. Art., heart rate - 124 beats per minute, respiratory rate - 24 per minute, saturation 100% without oxygen support.
Treatment was carried out in the intensive care unit. Saline infusion, clindamycin and ampicillin + sulbactam, immunoglobulin (IVIG) intravenously. White blood cell counts were 12,000/mm3. The patient also underwent cysto- and anoscopy to exclude gangrenous lesions and the source of infection. The patient underwent three debridement necrectomies on the penis and scrotum and subsequent skin grafts. Blood cultures isolated Staphylococcus aureus and Streptococcus pyogenes. After 22 days, the patient was discharged home in satisfactory condition.
The case is unique in that frequent masturbation is extremely rarely complicated, especially by Fournier's disease.
Sources
- Fournier Gangrene. National Organization for Rare Disorders, 2020.
- Thwaini, A et al. “Fournier's gangrene and its emergency management.” Postgraduate medical journal vol. 82.970 (2006): 516-9.
- Daniel Pendick "Everything You Should Know About Fournier's Gangrene"; Healthline, 2021.
- What Is Fournier's Gangrene? WebMD, 2021.
- M. N. Mallikarjuna, Abhishek Vijayakumar, Vijayraj S. Patil, B. S. Shivswamy, “Fournier's Gangrene: Current Practices,” International Scholarly Research Notices, vol. 2012, Article ID 942437, 8 pages, 2012.
- Theiss M, Hofmockel G, Eckert P, Frohmüller H. “Cosmetic and functional long-term outcome after surgery of Fournier gangrene.” Urologe A. 1996 Jul;35(4):338-41. German.
- H. Yanar, K. Taviloglu, C. Ertekin et al., “Fournier's gangrene: risk factors and strategies for management,” World Journal of Surgery, vol. 30, no. 9, pp. 1750–1754, 2006.
- R. Asci, S. Sarikaya, R. Buyukalpelli, A. F. Yilmaz, and S. Yildiz, “Fournier's gangrene: risk assessment and enzymatic debridement with lyophilized collagenase application,” European Urology, vol. 34, no. 5, pp. 411–418, 1998.
- M. Capelli-Schellpfeffer and G. S. Gerber, “The use of hyperbaric oxygen in urology,” Journal of Urology, vol. 162, no. 3, pp. 647–654, 1999.
- S. Parkash and V. Gajendran, “Surgical reconstruction of the sequelae of penile and scrotal gangrene: a plea for simplicity,” British Journal of Plastic Surgery, vol. 37, no. 3, pp. 354–357, 1984.