Are you suffering from abdominal pain, cramps and constant bowel movements? Unpleasant sensations in the intestinal area can ruin all plans, so we use various medications to relieve abdominal discomfort. But these measures only allow you to temporarily get rid of the symptoms of a serious disease, which return again and again. What if these symptoms have a single cause - irritable bowel syndrome? What this disease is, what its symptoms are and how to cure it, we will tell you in this article.
What is irritable bowel syndrome?
This is a disorder of the intestines and discomfort in the abdomen during bowel movements. The syndrome itself is not a disease, but rather a set of symptoms that often occur for an unknown reason. Unfortunately, such a disorder can significantly reduce a person’s quality of life, forcing him to remain in an uncomfortable state: digestion is disrupted, metabolic processes in the body worsen, and the saturation of the human body with nutrients decreases.
Irritable bowel syndrome is a very common occurrence among people aged 25 to 40 years. Statistics show that at least once in their life, every third person has experienced the unpleasant symptoms of irritable bowel syndrome.
Self-medication in this case can be very dangerous to health. The fact is that the syndrome is treated comprehensively and under the close attention of the attending physician. The consequence of self-medication can be intestinal obstruction and numerous chronic gastrointestinal diseases. With the first signs of irritable bowel syndrome, you should contact a therapist, who will refer you to a more specialized specialist - a gastroenterologist. The diagnosis is usually made only after excluding tumors and inflammatory changes in the intestines.
The intestines are where food is digested and nutrients are obtained by the body. When food enters the intestines, it moves along the intestines. This process of advancement is achieved through the work of smooth muscle cells within the intestinal walls. The cells alternately contract and relax. But when IBS (irritable bowel syndrome) appears, cell function is disrupted. Food begins to pass through the intestines either too quickly or too slowly. The result is discomfort and constipation or diarrhea.
Symptoms and treatment
Are you worried about frequent constipation or diarrhea?
Do you have any complaints about bloating, general weakness, fatigue, or insomnia? It could be irritable bowel syndrome. This is one of the most common diseases in gastroenterology. On average, about 15-20% of the adult population of the planet suffers from irritable bowel syndrome. However, many patients with symptoms of this pathology do not seek medical help. Because of this, they can manifest themselves over a long period of time, often throughout life. Although irritable bowel syndrome itself does not pose an immediate threat to life, it significantly reduces the quality of life and can cause serious unpleasant complications. It has been found that women suffer from irritable bowel syndrome twice as often as the stronger sex. The disease mainly affects adults. In approximately half of patients it appears before the age of 35.
Symptoms of irritable bowel syndrome
- nausea and gag reflex;
- flatulence with copious release of gases;
- abdominal pain or cramps;
- constant bloating;
- stool disorders - constipation or diarrhea;
- pain in the lower abdomen;
- sleep disturbance;
- increased heart rate;
- increased fatigue;
- long digestion of food;
- the appearance of mucus in the stool;
- false urge to defecate;
- loss of appetite.
Also, the disease is often accompanied by symptoms that, at first glance, are not characteristic of intestinal pathologies: headaches, discomfort in the spine and muscles, weight loss and abdominal swelling. All these symptoms are not constant, they can disappear and reappear over time. Unpleasant sensations most often appear after each meal, and then become less pronounced.
Disease prevention
Preventing irritable bowel syndrome is much easier and cheaper than treating it. Reconsider your lifestyle. Reduce the consumption of fatty, fried, smoked, spicy foods to a minimum, stop smoking and frequent alcohol consumption. Try to have breakfast, lunch and dinner at the same time, avoid snacking on the go. Follow a daily routine. Don't neglect physical activity, including walking and abdominal exercises. Positive attitudes will help reduce the level of anxiety; in difficult cases, consultations with a psychologist or psychotherapist.
Reasons for the development of the pathological phenomenon
- Nutrition. Eating fried, salty, sweet and fatty foods, as well as alcohol-containing drinks, has a negative effect on digestion. In addition, modern people constantly snack on the run. Which also negatively affects intestinal function.
- Hormonal disbalance. More often, this reason is typical for women during periods of life such as pregnancy, breastfeeding, menopause, and the menstrual cycle. As for the menstrual cycle, during this period the amount of chemicals changes, and the problem begins to manifest itself more clearly.
- Impaired intestinal motility. If motor skills work in an accelerated mode, this leads to stomach upset and diarrhea. On the contrary, slow bowel movements can cause constipation. As a result, pain leads to a sharp contraction of muscles.
- Emotional stress: stress, depression, anxiety, fatigue.
- Past diseases of the gastrointestinal tract. Infections that cause gastrointestinal diseases can subsequently affect the functioning of the entire intestine.
Non-pharmacological therapy
In combination with drug treatment of the disease, additional methods and techniques are recommended that speed up the healing process:
- physical activity within acceptable limits (for example, yoga). If you are overweight, it is also necessary to use programs to reduce your body mass index;
- dietary nutrition that excludes the use of poorly digestible substances, but includes foods enriched with soluble dietary fiber. In addition, it is necessary to exclude the use of products that cause gas formation;
- psychological consultations, stress management training programs.
Diagnosis of irritable bowel syndrome
If you have all the symptoms of the disease listed above, consult a physician. He will conduct an initial examination and refer you to a gastroenterologist. The purpose of primary diagnosis is to exclude the presence of other life-threatening diseases: tumors, inflammatory processes, growths, infectious diseases.
When visiting a doctor, you need to provide a complete medical history, report the presence and frequency of symptoms, and talk about the presence of chronic diseases. After examination and palpation (feeling), the specialist will refer you for laboratory tests, including:
- General blood analysis. The analysis allows you to determine whether an inflammatory process is present in the body, as well as to determine possible anemia.
- General urine analysis. Determines the presence or absence of blood and parasites in the patient’s body, which allows us to talk about the development of a number of intestinal diseases other than irritable bowel syndrome.
- Blood test for celiac disease. A specific blood test that allows you to identify a disease of the digestive system (celiac disease), in which the intestines cease to properly digest incoming food, which is accompanied by diarrhea.
- Colonoscopy. This is an examination of the colon from the inside using a special device (colonoscope).
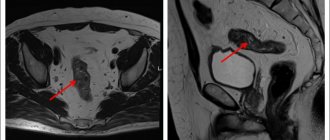
- Magnetic resonance imaging of the pelvis and abdomen. This is a non-invasive examination method that allows you to study the structure and condition of the organs and tissue of the pelvis in men and women using magnetic waves.
After all the studies have been carried out and all other intestinal diseases have been excluded, the doctor begins treatment and prescribes complex therapy, based on the patient’s medical history.
Treatment of pain in the intestines on the right and left lower abdomen
To determine the cause of severe pain in the intestines on the left and right side of the lower abdomen, the patient should visit a doctor. After the initial examination and consultation, the patient will be sent for testing. A general analysis of blood, urine and feces will show the internal indicators of the body and demonstrate the presence of any abnormalities in the systems of the human body.
For clearer results, the patient is referred for a bacteriological examination of stool, colonoscopy and endoscopic examination. After receiving the test results, the attending physician prescribes treatment for the patient. A medical expert prescribes medication, homeopathic or surgical intervention in advanced cases.
If necessary, to obtain information about the condition of the internal organs, the doctor refers the patient to undergo a computed tomography or ultrasound scan. These diagnostic tests are not recommended for pregnant women, nursing mothers, and children under sixteen years of age. Health care professionals do not recommend these procedures for certain groups of the population. The use of radiation and contrast fluid can negatively affect healthy organs.
To make an appointment for a consultation or examination at the private clinic “KDS Clinic”, leave a request on the website and managers will contact you as soon as possible.
Treatment of irritable bowel syndrome
Therapy for IBS should be carried out comprehensively in several stages. The treatment regimen depends on the individual characteristics of the body, the degree and time of the pathology. Most often, drug therapy is prescribed, which is supplemented by a special diet. In the absence of comprehensive treatment, symptoms will reappear from time to time.
The medications that the doctor prescribes for the treatment of IBS not only eliminate painful symptoms, but also improve the condition of the digestive system, and also prevent relapses and complications. When treating diarrhea syndrome, medications with antimicrobial properties are prescribed. They relieve irritation of intestinal tissues, stop excess flatulence and restore normal intestinal function.
When treating IBS with constipation, the use of natural medicines is indicated that eliminate difficulties with defecation, have a gentle effect on inflamed intestinal tissue and free it from feces. May be in the form of chewable tablets or rectal suppositories.
If the appearance of IBS is associated with neurological disorders, antidepressants are prescribed - they normalize the functioning of the nervous system and improve the psycho-emotional state.
To relieve pain, painkillers and antispasmodics are used - they relax muscle fibers and tissues that are in hypertonicity.
Diet for irritable bowel syndrome
The diet for IBS depends on what symptoms accompany the pathology. If you experience frequent constipation, you should exclude dry, salty foods from your diet. For diarrhea, avoid liquid foods, vegetables, and fruits.
If you suffer from flatulence, you should limit dairy products, nuts, and beans. If there is severe pain in the intestines, fatty, salty, and heavy foods are not allowed.
At the Medunion clinic you can undergo a full examination and treatment of irritable bowel syndrome. We employ practicing doctors with over 10 years of experience. In the diagnostic room you can take all tests and undergo hardware examination in a comfortable environment. For our clients there is a special offer “doctor at home”. If you are unable to visit our medical center yourself, a doctor will come to you and conduct an examination at home.
Take care of your health and make an appointment with a multidisciplinary medical center directly on our website.
Drug therapy
The following drugs are used in the treatment of irritable bowel syndrome:
- peppermint oil – used to reduce the severity of symptoms;
- antispasmodics - hyoscine, drotaverine and other drugs that have proven effective in treating this disease;
- antidepressants – can be prescribed as part of complex treatment to reduce the severity of symptoms. Tricyclics or SSRIs are used. As a rule, treatment involves taking the minimum effective dose. The course of admission is from 4 to 12 weeks. If the symptoms of the disease decrease, the duration of the course can be increased by the attending physician;
- probiotics – included in treatment if symptoms such as bloating and diarrhea are present. Monostrains or combination drugs are used that have a beneficial effect on the intestinal microflora;
- Rifaximin - the course of treatment for irritable bowel syndrome is about 4 weeks. The main condition for treatment with rifaximin is the absence of symptoms such as constipation;
- polyethylene glycol preparations - used in the treatment of constipation. Other symptoms are not affected;
- loperamide - reduces the severity of diarrhea. It has no effect on other symptoms.
Treatment with modern medicines
In case of acute enteritis, hospitalization is necessary; in a hospital setting, gastric lavage with a tube and bowel cleansing with laxatives are required. Acute intoxication is treated by drip administration of Ringer's solution, Trisol, and glucose. The intestinal flora is restored with the help of Intestopan, Bifikol, Colibacterin, Enteroseptol.
In case of chronic enteritis, antibacterial agents are not used to avoid dysbacteriosis. The flora is restored with the help of Linex, Bifidumbacterin, Lactobacterin. Panzinorm, Meksaza, Abomin, analogues of Enteroseptol, Intestopan are used. Diarrhea is stopped with drugs such as Imodium, Loperamide.
Acute colitis of infectious origin is treated in a specialized department of the hospital, where patients undergo a course of antibacterial therapy. For other forms of colitis, enveloping drugs (Kaolin), astringents (Bismuth drugs), and enzyme drugs (Bifikol, Colibacterin, Linex) are prescribed.
In chronic colitis, the main focus of therapy is aimed at normalizing the intestinal microflora. The patient is first given the shortest possible short course of antibiotics to destroy pathogenic microorganisms. Then treatment with eubiotics and probiotics occurs.
How the intestines work
The intestine is represented by two main sections: thin and thick. The small intestine begins with the duodenum, then passes into the jejunum and then into the ileum, ending with a special valve - the ileocecal valve, this is the border that separates the small intestine from the large intestine. Next, the large intestine is divided into three sections: the cecum, colon and rectum. The role of the intestines is difficult to overestimate, because it is in it that nutrients are absorbed from food, due to which our body exists. Our intestines also remove toxins, breakdown products, and undigested food.
Good to know
The entire surface of the intestine is populated by living microorganisms, they lead vigorous life activities, multiply, die, and perform a huge number of useful functions. Not only the functioning of the digestive system, but also the health of the entire organism depends on the quantitative and qualitative composition of microflora. An interesting fact is that there are no bacteria in the duodenum; they die due to the acid coming from the stomach, but about 300 varieties of microorganisms “live” freely in the sections of the large intestine, including fungi, protea, protozoa, bifidobacteria and others. Normally, the number of pathogenic microorganisms should not exceed 1% of the total number.
Human intestines: functions
Contrary to popular belief, the intestines are not only involved in the formation of feces. This organ is responsible for immunity and the general condition of the body. The child’s intestines ensure the development of all organs, systems and tissues of the body. Throughout its entire length, the small intestine is intertwined with a large number of blood vessels, due to which nutrients quickly enter the bloodstream through its walls.
It depends on the intestines whether the beneficial flora for absorption will be able to identify vitamins and minerals in the food bolus or not. Dysfunction of the long digestive organ threatens developmental delays, general weakness of the body, and decreased immunity.
The intestines are able to filter pathogenic flora and toxins, preventing them from entering the circulatory system and poisoning the body. At the first manifestations of the presence of a pathogen, a protective function is activated, accelerating peristalsis. Due to this, poisoned food does not linger in the body and leaves the lumen in an unprocessed form through the anus.
The more beneficial microflora in the intestines, the higher the body’s immunity and resistance to pathogens. When the balance of beneficial bacteria is disturbed, the pathogenic flora, having gained quantitative superiority, provokes the development of diseases that cause digestive disorders.
Where is an MRI of the intestine done?
Remote screening using a hardware installation is available in specialized medical institutions that contain diagnostic rooms with high-precision equipment. In St. Petersburg, both state and private organizations, distributed throughout all districts of the city, receive admissions. Before registering for a study, you must make sure that the clinic uses tomographs with a field generation frequency of 1.5 Tesla or more. Only high-field machines guarantee the correct scanning result.
You can find and compare MRI medical centers on the service of the “Unified Recording Center” in St. Petersburg. At the top of the page is the number of the consultation service, whose operators will not only answer your questions in detail, but will also suggest the addresses of conveniently located clinics and make an appointment for your free time. Institutions are distributed by location, ratings, prices for services and technical indicators of equipment, which makes comparison and selection easier. Book the procedure through the portal and receive a special discount from the service.
Functional constipation occurs 1.75–2.65 times more often among women compared to men [12, 25, 33], which is explained by anatomical, physiological and hormonal factors. The length of the colon in women is on average 10 cm longer, with the main difference being in the length of the transverse colon. Apparently, for this reason, the transverse colon in women in 62% of cases sags, reaching the pelvic cavity, more often has a tortuous course, forms additional loops and more “sharp” natural anatomical angles [34]. The normal rate of intestinal transit in women is lower by approximately 14 hours compared to men [5]. This difference is leveled out in postmenopause, which reflects the role of sex hormones in the regulation of intestinal motor activity [32].
Often, the first symptoms of intestinal dysfunction occur with menarche, and subsequently its motor activity varies depending on the phase of the menstrual cycle [29, 38]. Most often in the practice of an obstetrician-gynecologist, intestinal dysfunction is associated with the following conditions: pregnancy, postpartum period; premenstrual syndrome; primary dysmenorrhea; endometriosis, uterine fibroids; inflammatory diseases of the pelvic organs; genital prolapse.
Constipation during pregnancy
Constipation during pregnancy occurs in 25–40% of cases [2, 6, 28], and hormonal factors play a leading role in their occurrence. The level of progesterone, which increases from early pregnancy, has a physiological non-selective relaxing effect not only on the myometrium, but also on the smooth muscles of the gastrointestinal tract, increasing the threshold of excitability of smooth muscles to various stimuli [24]. In parallel with the increase in progesterone levels during pregnancy, there is a decrease in the concentration of motilin, a gastrointestinal hormone that regulates gastrointestinal motility [39]. The result of these changes is a decrease in the contractile activity of the gallbladder [18, 19], and insufficient flow of bile into the duodenum makes an additional contribution to the development of constipation in pregnant women. At the same time, an increase in the level of relaxin ensures the necessary relaxation of the smooth muscle cells of the blood vessels and uterus and, at the same time, the smooth muscles of the intestines through the activation of nitric oxide synthesis [4, 31].
Estrogens also contribute to disruption of intestinal motor function. Recent studies have shown the involvement of estrogens in increasing water absorption in the colon as a result of passive transport following sodium ions with the participation of the colonocyte apical membrane transporter protein NHE3 [1]. Expression of NHE3 protein in the proximal colon increases with increasing gestational age [7], concomitant with a significant increase in the density of estrogen receptor type β (ERβ). The result of these processes is a decrease in volume and compaction of feces, which have an insufficient stimulating effect on the mechanoreceptors of the colon, and as a result, a slowdown in intestinal transit.
Other causes of intestinal dysfunction during pregnancy include lifestyle factors: changing the diet with a decrease in the amount of dietary fiber, reducing daily fluid intake, sometimes recommended for preeclampsia, and limiting physical activity. Some medications prescribed during pregnancy can inhibit intestinal motor function (iron, magnesium, antispasmodic and β-mimetic drugs, progestins) [23]. The presence of prolonged constipation during pregnancy adversely affects the composition of the intestinal microflora, the permeability of the intestinal barrier and leads to changes in the microbiocenosis of the genital tract and immune status. This, in turn, can cause pregnancy complications, including premature termination.
When examining pregnant women with constipation, one should take into account additional causes of decreased intestinal functional activity, such as subclinical hypothyroidism, calcium deficiency, and gestational diabetes, which can manifest during pregnancy. Constipation in pregnant women is often functional in nature, however, in cases of severe constipation or in the presence of “alarm symptoms” (anemia, unmotivated weight loss, the appearance of blood in the stool, constant intense abdominal pain, fever, leukocytosis, etc.), organic causes should be excluded diseases. In this situation, sigmoidoscopy may be performed in the first and second trimesters of pregnancy.
Radiological diagnostic methods permitted during pregnancy include magnetic resonance imaging without contrast.
The approach to treating constipation in pregnant women does not differ from the generally accepted one and includes two stages. At the first stage, the diet, diet and drinking regimen are corrected with consumption of at least 1.5–2.0 liters of fluid per day. Dosed physical activity is recommended. If possible, doses that may cause constipation should be reduced or discontinued.
At the second stage of treatment, if the above measures are insufficiently effective, drug therapy is prescribed. Medicines used during pregnancy must be safe for the mother and fetus and provide the necessary therapeutic effect in minimal doses. According to the recommendations of the FDA (Food and Drug Administration), in the current range of laxatives, only a limited number of drugs can be considered acceptable for long-term use by pregnant women [20].
Among stimulant laxatives, anthroquinone derivatives (rhubarb, buckthorn preparations) have a teratogenic effect and are absolutely contraindicated during pregnancy. The use of senna and bisacodyl drugs in short courses is not associated with an adverse effect on the fetus, but may be accompanied by colicky abdominal pain and diarrhea, which makes their long-term use undesirable. Castor oil has a pronounced stimulating effect on the contractile activity of the myometrium, and therefore its use in pregnant women is strictly contraindicated [20]. Rectal suppositories with glycerin are popular among women suffering from constipation during pregnancy. But their action is based on an irritating effect and long-term use can lead to the development of inflammatory changes in the rectal mucosa.
A safer method is considered to be laxatives that increase the volume of intestinal contents. The use of dietary fiber significantly increases the frequency of bowel movements in pregnant women suffering from constipation [16]. But eating coarse dietary fiber, such as bran, can contribute to bloating and abdominal pain. Soluble dietary fiber in psyllium adsorbs water, acquires a gel-like viscous structure, is fermented by intestinal microflora and has a mild laxative effect. When using psyllium, there is no need to take additional amounts of water beyond the physiological volume, which is certainly an advantage for pregnant women, especially in the later stages. Macrogol (polyethylene glycol) preparations are inert substances, are practically not absorbed in the intestines and can be used during pregnancy.
Osmotic laxatives increase the volume of feces due to fluid retention in the lumen of the colon. Long-term or frequent use of saline laxatives (magnesium salts, sodium salts) during pregnancy should be avoided due to their adverse effects on electrolyte metabolism. The disaccharide lactulose, which is not absorbed by the intestinal wall, is broken down to form short-chain fatty acids, which increases the osmotic pressure in the intestinal lumen, increases the volume and acidifies the intestinal contents, thereby stimulating its peristalsis. Side effects of lactulose metabolism by intestinal microbiota in some cases include increased gas formation, flatulence, abdominal pain, and diarrhea.
Among laxatives that soften stool, petroleum jelly and glycerin are contraindicated during pregnancy due to impaired absorption of fat-soluble vitamins in the intestines, the risk of postpartum hemorrhage and hemorrhagic complications in the fetus. If episodic constipation occurs or at the initial stage of treatment of chronic constipation, it is possible to use microenemas containing sodium citrate, sodium lauryl sulfoacetate and sorbitol solution.
Constipation in the postpartum period
Constipation often complicates the course of the postpartum period, resulting from muscle weakness of the overstretched anterior abdominal wall and perineum, decreased anal sensitivity, low physical activity, insufficient intake of fluids and dietary fiber, changes in hormonal levels, fear of straining due to the presence of sutures in the perineum, or fear of pain. for hemorrhoids, taking painkillers and antispasmodics.
Among the therapeutic measures, patients are primarily recommended to correct the drinking regime and increase the content of foods rich in dietary fiber in the diet. If these measures are ineffective, laxatives are prescribed. The main requirement for drugs used during lactation is that they cannot pass into breast milk.
In the early postpartum period, stool softening laxatives are considered the drugs of choice, especially for patients with perineal trauma. One of the drugs in this group for topical use is the drug Microlax in the form of a solution in microenemas. The drug is approved for breastfeeding, as well as for children from birth. The positive properties of Microlax are complemented by its rapid action (within 10–15 minutes) and rectal administration. If necessary, re-use of microenemas is allowed. For long-term use in the postpartum period and lactation period, laxatives that increase the volume of feces (psyllium seeds, macrogol), osmotic laxatives (lactulose) are recommended. Stimulant laxatives (bisacodyl, sodium picosulfate) and their metabolites are not found in breast milk, however, their use should be limited to occasional use only [10].
The role of intestinal microbiota disorders in the development of gynecological pathology
To date, there is no consensus on the existence of a relationship between intestinal and vaginal microbiocenosis. At the same time, publications have appeared in the literature indicating the possible role of the colon as a reservoir of certain strains that colonize the vagina [35]. In a study by N.A. El Aila et al. Using the cultural method and genotyping, a certain similarity of vaginal and rectal microflora was demonstrated in terms of not only species composition, but also strain identity between vaginal and rectal isolates. The same authors showed a significant correlation between the qualitative and quantitative characteristics of strains of vaginal and rectal lactobacilli: Lactobacillus crispatus (p < 0.0001), L. jensenii (p < 0.0001), L. gasseri (p = 0.005), L. iners (p = 0.003), as well as pathogenic strains of Atopobium vaginae (p = 0.002) [9]. Oral administration of complex probiotic preparations containing several strains of Lactobacillus spp. with a high adhesive ability to the vaginal and intestinal epithelium, isolated from the vaginal microcenosis of healthy women, led to the normalization of the microscopic picture of vaginal smears and pH with their initial disturbances [35].
The role of intestinal microflora is not limited to influencing the vaginal microbiota. Microorganisms that populate the gastrointestinal tract take part in various metabolic processes, including the metabolism of sex hormones. The second phase of estrogen detoxification in the liver consists of their binding to glucuronic acid, which facilitates the excretion of hormones with bile into the intestines and then out of the body along with feces. However, some intestinal bacteria in the colon, mainly pathogenic, contain the enzyme β-glucuronidase, which cleaves the bond between excreted estrogen and glucuronic acid, after which the estrogens are reabsorbed by the intestinal wall and enterohepatic circulation. There is an opinion that an increase in β-glucuronidase activity and the associated estrogen imbalance may be associated with an increased risk of developing certain cancers, including breast cancer. In patients with uterine fibroids and breast cancer, there is a significant increase in the average number of Enterobacteriaceae, bacteroides, clostridia, and anaerobic lactobacilli compared with healthy women of the same age. The activity of β-glucuronidase increases on the background of a diet rich in fats and poor in plant fibers; it can be reduced by normalizing the composition of the intestinal microflora and using a lot of plant fiber and probiotic cultures of Lactobacillus spp in the diet. and Bifidobacterium spp., in both food products and probiotics.
Estrogens also influence the properties of the intestinal microbiota. In postmenopause, against the background of estrogen deficiency, changes in the composition and quantity of the microflora of the gastrointestinal tract are noted. Along with a decrease in the total number and diversity of Lactobacillus spp. [26] the content of clostridia, enterobacteria and such potential pathogens as Acinetobacter calcoaceticus, Enterobacter aerogenes, Clostridium freundii increases. This can be either a result of changes in the hormonal profile or an age-related weakening of immune homeostasis, a slowdown in intestinal motility and a decrease in the activity of digestive processes. In turn, a violation of the composition of the intestinal microflora entails changes not only in digestion processes, but also in a number of metabolic processes, absorption of micronutrients and pharmacokinetics of drugs.
One of the most serious problems associated with the onset of menopause is osteoporosis. A decrease in bone mineral density in this period of life is due to estrogen deficiency, lack of vitamin D and calcium. The concentration of calcium in the blood depends not only on its content in the diet, but also on bioavailability, including that determined by absorption in the intestines. In addition to vitamin D, a number of factors influence calcium absorption in the intestine. The absorption process is facilitated by caseinophosphopeptides, casein proteolysis products, some organic acids and fermentable prebiotic carbohydrates. Several mechanisms have been proposed for the positive effect of prebiotics (inulin, oligofructose, etc.) on mineral absorption. The acidic metabolites formed as a result of fermentation of prebiotics by intestinal microflora reduce the intestinal pH and destroy the calcium-phosphate-magnesium complex, while increasing the intraluminal concentration of ionized calcium and ensuring its passive absorption. In addition, short-chain fatty acids formed during the fermentation of prebiotics bind to calcium, forming calcium-hydrogen complexes and facilitating their passage through the enterocyte membrane. Disruption of the intestinal microflora of menopausal patients and a lack of fermentable fiber in the diet may be an additional risk factor for calcium metabolism disorders, even with calcium supplementation.
Intestinal microflora is also involved in the metabolism of phytoestrogens, which are widely used to correct menopausal disorders. The most active phytoestrogens - soy isoflavones - are present in food products in the inactive form of P-glycosides. In the intestine, under the influence of normal microflora, P-glycosides undergo hydrolysis and further metabolism, resulting in the formation of active estrogen-like substances: genistein, daidzein and glycitein. When intestinal microbiocenosis is disturbed, which often accompanies menopause, the intensity of hydrolysis of P-glycosides in the intestine decreases, which weakens the therapeutic effect, causing insufficient effectiveness of the use of phytoestrogens.
The role of intestinal microflora in the metabolism of bile acids and cholesterol is well known. In the colon, microorganisms metabolize cholesterol to form products that regulate cholesterol biosynthesis in the liver (propionate acetate).
On the other hand, intestinal bacteria are capable of deconjugation and hydroxylation of primary bile acids entering the intestine with bile to form secondary bile acids (deoxycholic acid). With normocenosis and a normal pH value, secondary bile acids are excreted from the intestine along with feces. However, with intestinal dysbiosis, accompanied by an increase in intraluminal pH, deoxycholic acid is ionized, which facilitates its absorption and enterohepatic circulation.
In the liver, high concentrations of deoxycholic acid, in turn, stimulate cholesterol biosynthesis. In addition, an increase in the content of hydrophobic deoxycholic acid in bile causes a change in the physicochemical properties of bile with a decrease in the solubility of cholesterol and, in total, -
with an increase in its production in the liver, it increases the risk of formation of cholesterol gallstones. The listed changes in metabolic disorders of cholesterol and bile acids under the influence of altered intestinal microbiota are of great importance for women of menopausal age, making an additional contribution to the risk of developing dyslipidemia, diseases of the cardiovascular system and cholelithiasis.
Gynecological practice
The relationship of gynecological diseases with intestinal diseases is determined by common pathogenetic factors, including hormonal influences and environmental influences, including dietary habits.
The significant difference in the prevalence of Crohn's disease and ulcerative colitis in developing and industrialized countries argues in favor of the dependence of the development of these diseases on the ratio of dietary fiber and easily digestible carbohydrates in the diet. Similar nutritional features underlie some gynecological pathological conditions, in particular those associated with metabolic disorders and endocrine homeostasis.
Dietary fiber provides a substrate for the growth of healthy microflora and is converted into short-chain fatty acids (particularly butyrate) in the intestine. Butyrate is an essential nutrient for colonocytes, ω-3 fatty acids are precursors for the anti-inflammatory leukotrienes-3 and -5, while ω-6 fatty acids are involved in the formation of the pro-inflammatory leukotrienes-4 and -6. Exogenous antioxidants, such as carotenoids, vitamins C and E, protect colonocytes from oxidative stress, but they perform a similar role during ovulation, protecting the ovaries from the damaging effects of excess free radicals. Low intake of antioxidants and an unfavorable ratio of ω-3 and ω-6 fatty acids are an important causative factor in the pathogenesis of Crohn's disease and, probably, ulcerative colitis, while simultaneously providing an increased risk of disorders of ovulatory function of the ovaries and infertility.
Gynecological diseases of the reproductive period of women's lives are often associated with IBS.
In Europe and North America, IBS in women is 1.5–2.0 times more common than in other regions. Regardless of the region, female gender is an independent risk factor for the development of post-infectious IBS. Interestingly, the gender specificity of IBS suggests a predominance of constipation and flatulence in women. Another characteristic feature is the connection of symptoms with the menstrual cycle - their intensification in the premenstrual period and during menstruation. This indicates the dependence of the disease on hormonal fluctuations [13, 14]. During pregnancy, with high but stable hormone concentrations, IBS symptoms decrease. On the other hand, women over 40 years of age experience a decrease in the incidence of IBS, and postmenopausal women experience a decrease in severity or (in some cases) even complete disappearance of symptoms. Suppression of cyclic fluctuations in sex hormones when taking combined oral contraceptives may reduce the severity of abdominal symptoms of IBS.
Among the hormonal “provocateurs” of IBS, estrogens are most often indicated, playing a significant role in the perception of pain. Estradiol is known to increase nociceptor activity through the expression of nerve growth factor (NGF) [8]. At the same time, a sharp drop in estradiol levels during ovulation and before menstruation reduces the pain sensitivity threshold [15]. This effect is realized in the central nervous system by reducing the number of μ-opioid receptors, reducing the serotonergic postsynaptic response and enhancing the stress response through corticotropin-releasing hormone signaling pathways. In the intestine, through regulation of 5-HT3-serotonin receptor expression, a fall in estrogen estradiol levels is associated with pronociceptive and prokinetic effects. On the other hand, the pro-inflammatory effects of estrogens determine the development of local immune disorders in predisposed individuals (imbalance of cytokines, increase in the number of mast cells in the intestinal mucosa). In addition to the central nervous system, estrogens regulate stress-dependent motor and secretory responses at the intestinal level through peripheral corticotropin-releasing hormone signaling pathways.
Treatment of IBS is one of the pressing problems of gastroenterology. The complex and not fully understood pathogenesis of the disease [21] and the variety of clinical manifestations determine a wide range of pharmaceuticals prescribed for the treatment of IBS [27]: selective myotropic antispasmodics, laxatives, intestinal antiseptics, antidiarrheal drugs, pro- and prebiotics, serotonin agonists and antagonists. receptors, psychotropic drugs (tranquilizers, antidepressants).
Some studies examine the positive effect of combined oral contraceptives in a prolonged mode and GnRH agonists on the course of IBS [22, 13], especially in women with dependence of the severity of symptoms on the phase of the menstrual cycle. At the same time, hormonal drugs, while reducing the severity of pain and flatulence, are not always effective against constipation and can themselves provoke its occurrence or worsening. In these cases, to treat constipation, it is advisable to prescribe courses of osmotic or stool volume-increasing laxatives. The disadvantages of these drugs include a delayed effect. In this regard, at the initial stage of treatment, it is recommended to use Microlax microenemas, which allows you to achieve bowel movement from the first day of treatment. The absence of side effects such as flatulence and abdominal pain when using Microlax is certainly an advantage in the treatment of IBS with a predominance of constipation.
Gynecological diseases dependent on hormonal fluctuations include premenstrual syndrome, dysmenorrhea and endometriosis. Each of these diseases has a characteristic clinical picture and should be treated by a gynecologist. Complaints of constipation in such patients are considered in the context of differential diagnosis, since they can equally serve as manifestations of gynecological pathology (for example, intestinal damage in retrocervical endometriosis, a variant of the autonomic reaction in dysmenorrhea or premenstrual syndrome) or a symptom of intestinal disease, including IBS . The difficulty of differential diagnosis is aggravated by the frequent combination of IBS with these diseases, and sometimes the root cause of the symptoms remains unrecognized. It is extremely difficult to differentiate the manifestations of IBS and chronic pelvic pain syndrome. According to some data, chronic pelvic pain occurs in 14% of cases in patients with IBS. At the same time, in patients with chronic pelvic pain syndrome, symptoms of IBS may be present in 29–79% of cases [21].
Intestinal dysfunction in the form of flatulence and frequent loose stools often accompany idiopathic dysmenorrhea. The formation of painful menstruation in idiopathic dysmenorrhea is based on local hyperestrogenism and excessive production of prostaglandins E2 and F2a, which are powerful stimulators of myometrial contractile activity. The effects of prostaglandins on intestinal function include disruption of transepithelial ion transport, stimulation of mucus production into the intestinal lumen and bicarbonate secretion, as well as increased motor activity [36], which explains the combination of dysmenorrhea with these intestinal symptoms and justifies the management tactics of such patients. Reducing the concentration of prostaglandins during menstruation, which can be achieved with the help of non-steroidal anti-inflammatory drugs or hormonal progestin-containing therapy, including combined oral contraceptives, can relieve not only the symptoms of dysmenorrhea, but also the associated intestinal dysfunction.
Genital prolapse
In postmenopause, one of the pressing problems associated with intestinal dysfunction (constipation) is the failure of the pelvic floor muscles. A decrease in estrogen levels leads to dystrophic changes in the ligamentous and muscular apparatus of the pelvic floor, and an additional factor is provided by perineal injuries received during childbirth. Obstruction during defecation is created by widening the anorectal angle, weakening of the muscles involved in defecation, and a more vertical orientation of the rectum. Weakness of the pelvic floor muscles is often combined with a rectocele, which is a prolapse of the anterior wall of the rectum or the posterior wall of the vagina into its lumen. This anatomical defect is associated with superior, inferior or lateral tears and central hyperextension of the rectovaginal fascia below the musculoskeletal muscles [24].
Clinical signs of rectocele: a feeling of incomplete emptying of the rectum, a feeling of “obstruction” during defecation. Pressing your finger on the perineum facilitates bowel movements. Bimanual examination of patients with rectocele reveals a defect in the anterior wall of the rectum. X-ray examination (defecography) reveals pelvic floor insufficiency, diagnosed by a descent of the perineum by more than 4 cm [11, 17]. A rectocele is considered clinically significant if its size is more than 3 cm. Ultrasound is an informative method for studying patients with impaired pelvic floor function. With rectocele, sonographic signs of deformation and saccular protrusion of the anterior wall of the rectum are determined when viewed in a longitudinal projection.
Treatment includes conservative and surgical stages. At the stage of conservative treatment, correction of diet and drinking regime, the use of stimulant and osmotic laxatives, physiotherapy, gymnastics to strengthen the pelvic floor muscles, and water procedures are used. However, in a number of cases, the effect of these measures is incomplete and with age, as dystrophic changes in the ligamentous and muscular apparatus of the pelvis progress, the only effective method of treatment becomes surgical correction of genital prolapse [3], which consists of plastic surgery of the pelvic floor and vaginal muscles transvaginally or perineally -anal access.
Conclusion
Intestinal dysfunction in women is an interdisciplinary problem. To optimize further management tactics at the stage of collecting an anamnesis, patients with signs of functional intestinal disorders should not only pay attention to gastroenterological symptoms, but also identify a possible connection with the menstrual cycle, reproductive status and gynecological pathology. If a connection between symptoms and the menstrual cycle or chronic pelvic pain is detected, consultation with a gynecologist is recommended. Contacting a gynecologist is necessary in all cases when a gastroenterologist is monitoring postmenopausal women.
Main causes of intestinal diseases
- predisposition can be inherited;
- unbalanced diet;
- low-quality products;
- increased psycho-emotional stress;
- living in places with poor ecology;
- work in hazardous production;
- intestinal infections;
- taking strong medications;
- deficiency of vitamins, micro and macroelements;
- deviations from the physiological norm of body weight, both thinness and overweight;
- presence of bad habits;
- physical inactivity.
The main reasons, as you can see listed above, depend on lifestyle and can be corrected, with the exception of heredity.
9 out of 10 people on the planet have problems with the digestive tract, expressed in one form or another. For example, today every fifth patient examined is diagnosed with IBS, and the female half suffers 4 times more often, and the bulk of patients are people over 30 years of age.