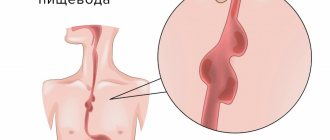
1.Structure of the esophagus
Esophagus
- a muscular tube connecting the throat (pharynx) to the stomach. The length of the esophagus is about 20 centimeters, and its inner surface is a pink mucous membrane. There is a part of the esophagus called the upper esophageal sphincter (UES). This is a group of muscles at the top of the esophagus that work during breathing, eating, belching and vomiting. A person can consciously control this muscle group. The upper esophageal sphincter muscle also holds food and secretions that may come from the windpipe.
The lower esophageal sphincter (LES) is a group of muscles at the lower end of the esophagus where it connects to the stomach. When the lower esophageal sphincter is closed, it prevents acid and stomach contents from moving back out of the stomach. The muscles of the LES are not subject to conscious control.
Diseases of the esophagus
, in fact, not so little. Some of them are quite serious, some do not require complex and long-term treatment. Depending on the severity of the disease, it may be treated by gastroenterologists or thoracic surgeons, who perform operations on the esophagus when necessary for treatment.
A must read! Help with treatment and hospitalization!
The first symptoms of esophageal cancer
The first symptoms of esophageal cancer may not be alarming
Disruption of the normal patency of the esophagus can be caused not only by the presence of a cancerous tumor, but also by the occurrence of perifocal inflammation or spasm of the esophagus. At the initial stage, the first symptom is dysphagia, which occurs due to insufficient chewing of food.
The patient may feel an imaginary sticking of food to the walls of the esophagus, or some retention at some level of the esophagus. Most often, these unpleasant sensations are eliminated by a sip of water, but after a while even thoroughly chewed food stops passing, which is why the patient is forced to take exclusively liquid or semi-liquid food.
Sometimes, after prolonged dysphagia, a period of improvement in esophageal conduction may occur, which may be caused by the onset of tumor disintegration. Before the onset of dysphagia, there may be sensations of a foreign body in the esophagus, a feeling of scratching in the chest area, and painful sensations that are observed when swallowing food.
2. The most common diseases of the esophagus
- Heartburn
. Heartburn occurs when the lower esophageal sphincter does not close completely. As a result, the acidic contents of the stomach enter the esophagus. This is called reflux. This reflux may cause heartburn, coughing, or hoarseness, or cause no symptoms at all. - Gastroesophageal reflux disease (GERD)
. If reflux occurs frequently or is accompanied by unpleasant symptoms, it is called GERD. - Esophagitis
. Esophagitis is inflammation of the esophagus. Esophagitis can be associated with irritation of the esophagus, either as a result of reflux or infection. - Barrett's esophagus
. Regular reflux of stomach acid causes irritation of the esophagus, which can result in changes in the structure of its lower part. In very rare cases, Barrett's esophagus progresses to esophageal cancer. - Esophageal ulcer
. With an esophageal ulcer, erosions form in the mucous membrane of the esophagus. This is often the cause of chronic reflux. - Esophageal strictures, or narrowing of the esophagus
. Chronic irritation from reflux is a common cause of esophageal strictures. - Achalasia of the esophagus
. Achalasia is a rare condition in which the lower esophageal sphincter does not relax. Difficulty swallowing and regurgitation of food are the most common symptoms of the disease. - Esophageal carcinoma
. Esophageal cancer is a serious disease, which, however, is not so common. Risk factors for the development of esophageal cancer are smoking, alcoholism and chronic reflux. - Mallory-Weiss syndrome, or gastroesophageal rupture-hemorrhagic syndrome
, occurs when tears occur in the surface of the esophagus due to frequent vomiting. Such ruptures are accompanied by internal bleeding and subsequent vomiting of blood. - Varicose veins of the esophagus
. In people with cirrhosis, the veins in the esophagus may become enlarged and protruding. These veins can cause life-threatening bleeding. - Ring-shaped formations in the lower parts of the esophagus
. This is a benign collection of tissue in the form of a ring around the lower end of the esophagus. Typically, these rings do not cause any symptoms, but in some cases they can cause difficulty swallowing. - A collection of tissue at the top of the esophagus
. A disease that develops in a similar way to ring-shaped formations in the lower part of the esophagus, which also usually does not cause unpleasant symptoms. - Plummer-Vinson syndrome
. This is a disease of the esophagus accompanied by chronic iron deficiency anemia, ring-shaped formations in the upper part of the esophagus and difficulty swallowing. Iron therapy and expansion of esophageal tissue are the main methods of treating the disease.
Visit our Gastroenterology page
Pathology of the stomach and esophagus on ultrasound
Types of pathological changes in the stomach on ultrasound
Despite the difficulties of visualizing the stomach on ultrasound, due to the presence of a cavity in the organ, the accumulation of gases and the constantly changing shape due to peristalsis, the sonography method allows one to obtain fairly extensive and high-quality information about the condition of the stomach, on the basis of which various pathologies are identified.
Ultrasound signs of gastric pathology are the following:
- Changing the shape of an organ;
- Changes in the diameter of the stomach lumen;
- Changing wall thickness;
- The presence of irregularities on the inner or outer surface of the stomach wall;
- The presence of bulges on the wall of the stomach;
- Lack of peristalsis;
- Presence of antiperistalsis.
The main sign of stomach pathology is thickening of its walls and expansion/narrowing of the lumen of the organ. Thickening of the walls of the stomach with a characteristic uneven echogenicity, when the outer part of the wall is hypoechoic compared to the hyperechoic inner part, is called a symptom of damage to a hollow organ. Currently, in the world medical literature, the terms “target”, “lesion halo”, “pseudo-kidney”, “bull’s eye”, “pathological type of cockade” are also used as synonyms for the term “symptom of lesion of a hollow organ”. All of the above terms refer to the same pathological condition of the stomach, and therefore can be used as equivalent. However, in the countries of the former USSR, the most commonly used term is “symptom of an affected hollow organ,” which we will also use. Thus, thickening of the stomach wall, as a symptom of an affected hollow organ, can be diffuse and limited. With diffuse thickening, ultrasound shows an increase in wall thickness along its entire length. And with limited thickening, the wall of the stomach turns out to be thicker than normal only in a certain limited area. Unfortunately, the two main pathological signs of stomach diseases detected by ultrasound, namely the symptom of the affected hollow organ and the expansion/narrowing of the organ lumen, are nonspecific. This means that these pathological signs are inherent in many diseases, as a result of which it is impossible to accurately diagnose using ultrasound data alone. In order to correctly diagnose a person’s existing stomach disease and choose one of the many pathologies that are characterized by a symptom of an affected hollow organ or a change in the lumen of the organ, it is necessary, in addition to the ultrasound results, to also evaluate the clinical symptoms that worry the patient. Only a combination of pathological changes on ultrasound with clinical symptoms will help make the correct diagnosis. Below, for general orientation in the problem, we will provide a table in which we will indicate which diseases of the stomach are characterized by the presence of symptoms on ultrasound of the affected hollow organ and changes in the lumen of the organ.
| Diseases characterized by an ultrasound symptom of an affected hollow organ with diffuse wall thickening | Diseases characterized by an ultrasound symptom of an affected hollow organ with limited wall thickening | Diseases that are characterized by narrowing or widening of the lumen of the stomach cavity on ultrasound |
| Swelling of the stomach wall | Pyloric stenosis | Scar stricture |
| Chronic gastritis type B | Ulceration of carcinoma | Inflammatory stenosis |
| Ménétrier's disease | Stomach ulcer | Tumor-induced stenosis |
| Infiltrative carcinoma | Varicose veins | Impaired evacuation of gastric contents |
| Malignant lymphoma | Gastric carcinoma | |
| Malignant lymphoma of the stomach | ||
| Initial stage of malignant tumor | ||
| Benign tumors (leiomyoma, neuroma, stromal tumors) |
Swelling of the stomach wall can be observed in acute pancreatitis, nephrotic syndrome, congestive heart failure, as well as protein deficiency in the body. Pyloric stenosis can be congenital or acquired due to inflammation, ulcers or tumors.
Ultrasound picture for various diseases of the stomach
Currently, there are six main pathological processes of the stomach that can be accurately diagnosed using ultrasound - these are erosive and ulcerative lesions, polyps, pyloric stenosis, duodenogastric reflux, malignant tumors and malformations. Below we present the characteristic features of the ultrasound picture for the six different above-mentioned pathologies of the stomach, as well as damage to the organ.
Ultrasound picture of the developmental defect “pyloric stenosis”
With congenital pyloric stenosis, a baby develops persistent vomiting of gastric contents at 2–4 weeks of life. Ultrasound shows a pronounced symptom of the affected hollow organ, namely: sharp thickening of the walls in the antrum, narrowing of the walls in the central part and the general appearance of the stomach as an “hourglass”, as well as the presence of contents in the stomach more than 24 hours after ingestion. Ultrasound picture of the developmental defect “duplication of the stomach”
Using ultrasound, it is possible to establish a doubling of the stomach only by performing a water-siphon test so that both cavities are filled with water and the doctor can clearly see them. A diverticulum is an area of protrusion of the wall of the organ. Such diverticula can be single or multiple; on ultrasound they are visible only during a water-siphon test, when their lumen is filled with water and makes them visible. A diverticulum filled with water is an anechoic formation of any shape, bulging away from the wall of the stomach and connected to its cavity by a thin leg. Damage to the stomach usually occurs due to mechanical impacts on the area where the organ is located, for example, from blows to the stomach, a fall from a height onto the stomach etc. Such damage to the stomach can manifest itself as bruises, tears and ruptures of the walls of the organ. Less commonly, there are injuries caused by chemical substances, the picture of which on ultrasound is different from mechanical injuries. Gastric contusion is characterized by limited weakly echogenic thickening or bulging of the wall in the area of damage. The bruise is better visible when performing a water-siphon test than on an empty stomach. A rupture of the stomach wall is characterized by an uneven contour of the walls and their interruption in the area of \u200b\u200bthe rupture. When performing a water-siphon test, a rupture is easily diagnosed, since an ultrasound immediately shows the place where water leaks into the abdominal cavity. Chemical damage to the stomach wall is characterized by its thickening, doubling of the contour (an echo-negative stripe on the outside, and an echo-positive stripe on the inside). If, as a result of the damage, a cicatricial narrowing of the stomach cavity has developed, then an ultrasound will reveal fluid and food debris taken more than 14 hours ago. A gastric ulcer on an ultrasound looks like a hyperechoic thickening of the wall with its deformation and narrowing of the lumen. In addition, an excess amount of fluid on an empty stomach is recorded, a symptom of damage to a hollow organ. The following sizes of various parts of the stomach according to ultrasound are characteristic:
- Outer diameter 16 – 22 mm;
- Thickening of the wall of the gastric outlet from 6 to 10 mm;
- The distance between the walls in the thickening area is 7 – 12 mm;
- Image ratio 0.5 – 3.3 mm.
When performing a water-siphon test for a stomach ulcer, the following symptoms are characteristic:
- A clear, uneven contour of the wall in the area of the ulcer with hyperechoic inclusions;
- Uneven thickening of the internal hyperechoic layer of the stomach up to 2 – 4 mm;
- The wall thickness in the area of ulcer or erosion is always more than 5 mm;
- Indistinct layering of the wall in the area of the ulcer;
- Inactive peristalsis.
Ultrasound picture for gastritis
The walls of the stomach are evenly thickened, their echogenicity is uneven, with alternating hypoechoic and hyperechoic areas, more than 40 ml of liquid is detected in the cavity on an empty stomach, the diameter of the pylorus is more than 10 mm, signs of duodenogastric reflux. Stomach peristalsis is sluggish. Menetrier's disease is a giant hypertrophic gastritis, in which the gastric mucosa forms huge folds with polyp-like growths. Ultrasound shows a highly thickened wall with uneven echogenicity. Peristalsis is sluggish. A large amount of liquid and food taken more than 14 hours ago is found in the stomach. A characteristic symptom of damage to a hollow organ is with a thickening of the wall in the area where the polyp is localized to 20–28 mm, a gap between the walls in the area of the thickening of 3–12 mm. There is also an uneven structure of the stomach wall in the area of thickening, the image coefficient in the area of the polyp is 0.9 - 9. The amount of fluid in the stomach on an empty stomach is normal. When performing a water-siphon test on ultrasound, a polypoid bulging of the wall into the lumen of the stomach is clearly visible. The structure of the polyps is heterogeneous, there is no layering.
Ultrasound picture for malignant tumors of the stomach
There is always a symptom of damage to a hollow organ above the area where the tumor is localized. The wall is thickened unevenly (from 10 to 30 mm), the thickening area is hypoechoic, heterogeneous, with impaired layering. The outer contour of the stomach wall in the area where the tumor is located is uneven, but clear. The lumen of the stomach in the tumor area is 2 – 16 mm. The lower border of the greater curvature of the stomach is lower than normal. The amount of fluid in the stomach on an empty stomach is either within normal limits or slightly increased. When performing a water-siphon test, uneven filling of the cavity with water and its insufficient expansion are noted. Rigidity of the thickened wall and sluggish peristalsis are also characteristic. The internal contour of the stomach is hyperechoic, fragmented and thickened more than 3 mm. In the area of the tumor, the outer and inner contours of the stomach are uneven, but clear. Pyloric stenosis is a narrowing of the outlet of the stomach, due to which the evacuation of food masses into the duodenum is impaired. The causes of pyloric stenosis are usually tumors or a long course of a peptic ulcer, as a result of which scars are formed that tighten the walls of the stomach and reduce the lumen of its pyloric part. Pyloric stenosis is characterized by a shapeless hyperechoic formation with a sharp narrowing of the lumen of the affected area. At the initial stage, the walls of the stomach are thickened, but then they become thinner and the cavity expands. An ultrasound shows that the stomach is dilated and filled with contents of different ages. The amount of fluid on an empty stomach is more than normal, and there is sediment in it. The lower limit of the greater curvature of the stomach is significantly lower than normal. Peristalsis is either absent or weak. In the area of stenosis there is a symptom of damage to a hollow organ, and the wall is thickened to 7 - 22 mm, it has no layering, and the image coefficient is 0.6 - 8.5. When performing a water-siphon test for pyloric stenosis, the patient can only drink a small amount of liquid – no more than 300 ml, due to a feeling of fullness in the abdomen, nausea and sometimes vomiting. When liquid enters the stomach, its contents are mixed and sediment floats to the surface. The lower border of the greater curvature drops even lower than when examined on an empty stomach. Peristalsis is sluggish or absent. It is impossible to visualize the normal layering of the stomach wall in the area of stenosis. Duodenogastric reflux is a pathological condition in which the contents of the duodenum are refluxed into the stomach. Reflux is detected during a water-siphon test, and on an empty stomach it can be seen on an ultrasound only if there is an accumulation of fluid in the patient’s stomach in an amount greater than normal. On ultrasound, reflux is visible by the retrograde movement of hyperechoic particles from the duodenum up the stomach after filling it with water. The presence of fluid in the stomach on an empty stomach in an amount of more than 40 ml may indicate a peptic ulcer, gastritis, pyloric stenosis or a malignant tumor. In order to understand exactly what disease the fluid in the stomach indicates in a particular case, you need to take into account other signs on ultrasound, as well as the clinical symptoms that the person has.
Pathological changes in the esophagus and ultrasound images in various diseases
Pathological changes in the esophagus on ultrasound are changes in the diameter, wall thickness, length of the abdominal organ, as well as the angle of His. Let's consider what ultrasound signs are characteristic of various pathologies of the esophagus. GER is a pathological reflux of stomach contents into the esophagus. And GERD is damage to the lining of the esophagus due to reflux. GER and GERD are characterized by expansion of the lumen of the esophagus on ultrasound and thickening of its wall. Chalazia is weak peristalsis, as a result of which food stagnates in the esophagus, moving only under the influence of gravity. On ultrasound, chalazia of the esophagus is characterized by expansion of the lumen of the organ and thickening of its wall. Chalazia cardia is characterized by a gaping of the distal esophagus up to 6–14 mm, as well as visible flow of stomach contents into the esophagus. Cardiospasm is a pathological increase in the tone of the esophagus, as a result of which food does not move well to the stomach. Cardiospasm on ultrasound is characterized by expansion of the thoracic esophagus and at the same time a sharp narrowing of the esophageal-gastric junction to 3 - 5 mm. Stagnant contents are visible in the lumen of the esophagus, the wall of the organ is slightly thickened.
3.Diagnosis of diseases
Of course, depending on the symptoms of which disease the doctor sees during the initial examination and consultation, methods for further diagnosing diseases of the esophagus will be selected individually. Let's talk about some of them:
- Upper endoscopy, FGDS (esophagogastroduodenoscopy)
. In this procedure, a flexible, thin tube with a camera on the end (endoscope) is inserted into the esophagus through the mouth. An endoscope allows you to examine the stomach and duodenum (small intestine). - pH monitoring of the esophagus
. A probe that monitors pH levels is inserted into the esophagus. This method is used to diagnose GERD and monitor the progress of GERD treatment. - X-ray examination
with preliminary administration of drugs containing barium. This method is usually used to determine the causes of difficulty swallowing. - Biopsy
. A method for diagnosing diseases of the esophagus, in which a sample of esophageal tissue is taken using endoscopy, which is then examined under a microscope. - Confocal laser endomicroscopy
. This is a new procedure in which a microscope is inserted into the patient's esophagus. Endomicroscopy can be a good alternative to biopsy.
About our clinic Chistye Prudy metro station Medintercom page!
Diagnosis of Zenker's diverticula.
Pharyngeal-esophageal diverticula can sometimes be detected by inspection and palpation of the neck. The protrusion has a soft consistency, decreases with pressure; after drinking water, a splashing noise can be detected by percussion over it.
The main diagnostic method is a contrast X-ray examination, which establishes the presence of a diverticulum, the width of the neck, the duration of barium retention in it, the degree of obstruction of the esophagus, signs of the development of a polyp and cancer in the diverticulum, the formation of esophageal-bronchial and esophageal-mediastinal fistulas. Fiberendoscopic examination makes it possible to establish the presence of a diverticulum, detect ulceration of its mucous membrane, the presence of bleeding, and diagnose a polyp or cancer in the diverticulum. Due to the high risk of perforation of the esophageal diverticulum, esophagoscopy should be performed with great caution.
It is optimal to perform esophagomanometry - a study of esophageal motility. Patients with coronary symptoms undergo a consultation with a cardiologist, an ECG study, Holter monitoring, and echocardiography.
Differential diagnosis of esophageal diverticulum is carried out with GERD, esophagospasm, hiatal hernia, esophageal strictures, achalasia cardia, esophageal cancer, mediastinal cyst, angina pectoris, and ischemic heart disease.
4. Treatment of diseases of the esophagus
Just like the diagnosis of esophageal diseases, treatment depends on what specific disease is diagnosed. Among the treatment methods include:
- Use of H2 blockers
. The release of acid in the stomach is stimulated by histamine. Some antihistamines are called H2 blockers. They can reduce acid content and improve the condition of a patient with GERD and esophagitis. - Proton pump inhibitors
. These medications block many of the acid production processes in the stomach and also help with GERD. In addition, inhibitors help heal ulcers or esophagitis. - Esophagectomy, or removal of the esophagus
. This is a surgical procedure performed by thoracic surgeons. As a rule, it is performed for esophageal cancer. - Dilatation of the esophagus
. A special device is passed down the esophagus and then expands on its own, causing the esophageal ring, stricture, and other formations that prevent swallowing to widen. - Ringing of esophageal varices
. This procedure is performed endoscopically and involves wrapping rubber band-like devices around the esophageal varices. This reduces the chance of bleeding.
Surgical treatment of pharyngeal-esophageal (Zenker) diverticula.
Indications for surgical treatment are as follows: complications (perforation, penetration, bleeding, stenosis of the esophagus, cancer, development of fistulas), large diverticula complicated by at least short-term retention of food masses in them, long-term retention of food in the diverticulum, regardless of its size. Ineffectiveness of conservative therapy.
The essence of surgical treatment is complete removal of the diverticulum.
(cutting off from the esophagus, followed by suturing the organ wall) - diverticulectomy: the diverticulum is isolated from the surrounding tissues to the neck, a myotomy is performed, it is excised and the hole in the wall of the esophagus is sutured.
We isolate pharyngoesophageal diverticula from the cervical approach. A cosmetic skin incision is made in the projection of the anterior edge of the left sternocleidomastoid muscle. We mobilize the left lobe of the thyroid gland, retract it medially, and the neurovascular bundle laterally. Before surgery, a thick probe is inserted into the esophagus, which greatly facilitates the surgical treatment of esophageal diverticula. Then we perform extramucosal esophagomyotomy
several centimeters long, making sure that all the fibers of the m. cricopharyngeus (cricopharyngeal myotomy). We isolate the diverticulum up to the neck and stitch its base with an EndoGia-30 endoscopic stapler (Switzerland). The specimen is sent for pathohistological examination. The duration of stay in the clinic is 2-3 days. You can eat after 1-2 days.
Watch a video of operations performed by Professor K.V. Puchkov. You can visit the website “Video of operations of the best surgeons in the world.”
Symptoms and clinical manifestations of epiphrenic diverticula
Almost half of epiphrenic diverticula are detected incidentally as a radiological finding. Usually these are diverticula with a diameter of up to 2-3 cm. With epiphrenic diverticula, patients complain of a feeling of heaviness, pain in the lower part of the sternum or in the area of the xiphoid process, and progressive difficulty swallowing. Some patients experience aerophagia, putrid breath, and regurgitation of old decomposed food. In some cases, attacks of bronchial asthma and angina may occur. The severity of the symptoms of the disease depends on the size of the diverticulum and the degree of its filling with food masses.
Indications for surgical intervention for epiphrenic diverticula do not differ from the treatment of Zenker's diverticula. The operation is indicated for complications: perforation, penetration, bleeding, stenosis of the esophagus, cancer, development of fistulas, large diverticula complicated by at least short-term retention of food masses in them, long-term retention of food in the diverticulum, regardless of its size. Lack of effectiveness from conservative therapy.
Very important! A feature of my approach to choosing treatment tactics for patients with esophageal diverticula is the earlier determination of indications for surgical treatment using the laparoscopic method (through several punctures of the abdominal wall), without waiting for complications to develop and without wasting time on useless conservative treatment methods.
Typically, the traditional approach, which most clinics use, to epiphrenic diverticula is to perform a left-sided thoracotomy along the VII - VIII intercostal space.
Currently, in the surgery of esophageal diverticula, methods for their removal using video thoracoscopic or laparoscopic (which is even less traumatic) techniques are becoming increasingly widespread.
My experience in treating patients with esophageal diverticula is more than 14 years
.
During this time, I was able to successfully operate and treat more than 100 patients
.
Very important! Unlike other clinics, I use a minimally invasive laparoscopic approach, which allows, without opening the pleural cavity, to isolate the epiphrenic diverticulum at a distance of up to 8-10 cm from the cardia, remove it and reliably close the esophageal wound. To do this, I stitch the base of the diverticulum with an endoscopic stapler EndoGia-30 (Switzerland), which allows you to apply a 3-row titanium suture.
The basis of a precision technique for bloodless isolation of a diverticulum from surrounding tissues is the use of the LigaSure dosed vessel ligation system (Switzerland).
Very important! I always remove the esophageal diverticulum under the intraoperative control of fibroesophagoscopy; this allows during the operation (by means of illumination) to give the surgeon an excellent reference point in the surrounding tissues and, most importantly, to excise the diverticulum under double visual control (laparoscopy and fibroisophagoscopy). This double control, in turn, guarantees the completeness of its excision and the absence of narrowing of the lumen of the esophagus after suturing the diverticulum stalk with a stapler.
In the case of a combination of epiphrenic diverticula and achalasia cardia, hiatal hernia, chronic reflux esophagitis
I perform simultaneous simultaneous surgical intervention: diverticulectomy and correction of the hiatal hernia or cardiomyotomy in my own modification.
The patient begins to walk the next day after surgery and eat food 1-2 days later. Discharged on the 3rd day, after a control chest x-ray.
Thus, the earlier (before complications develop) surgery is performed for esophageal diverticulum, the better the treatment results.
Pharyngeal-esophageal diverticula are operated on by a thoracic surgeon using access to the neck, through a cosmetic incision using the LigaSure dosed vascular ligation system (Switzerland) to isolate the diverticulum and the endoscopic stapler EndoGia-30 (Switzerland), which allows you to apply a safe 3-row titanium suture to the wall esophagus.
Rice. 2. Removal of esophageal diverticulum using an endoscopic stapler using laparoscopic access.
Epiphrenic diverticula (from 1 to 10 cm from the cardia) I operate laparoscopically
through punctures, also using the LigaSure dosed vessel ligation system (Switzerland) to isolate the diverticulum and the EndoGia-30 endoscopic stapler (Switzerland) (Fig. 2).
In this case, I perform all stages under double visual control - laparoscopic and fibroesophagoscopic from the side of the lumen of the esophagus.
All of the above measures make it possible to perform surgical interventions for esophageal diverticula reliably, with a minimum number of complications, with a short hospitalization period and a quick return to normal life.
Epiphrenic diverticula
Epiphrenic diverticula, usually pulsational, are located along the posterior or right wall of the esophagus 2-11 cm above the diaphragm. Diverticula are spherical or mushroom-shaped. The leading factors in the formation of epiphrenic diverticula are the following factors: weakness of the muscular wall, increased intra-esophageal pressure and pressure of the food bolus on weak areas of the esophageal wall. Muscular weakness can be congenital or acquired. An increase in intra-esophageal pressure occurs due to uncoordinated peristalsis of the esophagus and its lower sphincter.