Drinking even small doses of alcohol can cause hangover symptoms. They are familiar to every person who has drunk alcohol at least once in his life. Dry mouth, headache, dizziness, apathy, general loss of strength - these are only a small part of the symptoms indicating the development of acute alcohol intoxication. The severity of hangover symptoms depends on how much alcohol was drunk, its quality, body characteristics and other factors.
You can eliminate the general symptoms of a hangover, improve your well-being, and literally bring a person back to life with the help of the high-quality drug Polysorb. Polysorb is a drug related to energy sorbents. Contains highly dispersed silica. Produced in Ukraine under the trademarks Atoxil and Silix. It is well tolerated and compatible with alcohol. It should be used only after carefully reading the instructions.
Small particles are capable of sorbing various substances. Their specific external surface is 300 sq.m/g. Colloidal particles are amorphous because their formula does not have a crystalline base.
The sorbent is produced in the form of a white powder for preparing a suspension. Then you need to drink it. When the powder is mixed with water, a white colloidal solution is formed. Polysorb is available in the form of a sachet with a capacity of 1 - 3 g or a jar with 12 - 50 g of powder.
All sorbents have high antitoxic ability. It has been clinically established that in acute alcohol poisoning, it is Polysorb that has the most pronounced antitoxic effect. It should be borne in mind that the sorbent does not act on alcohol, but on toxic substances formed during the breakdown of ethanol.
Mechanism of action of Polysorb
As soon as a person drinks alcohol, the liver begins to process it. It is in the largest gland in our body that the breakdown of alcohol into acetaldehyde occurs. This is an extremely toxic substance, on which the development of hangover syndrome depends. Under normal conditions, acetaldehyde undergoes a process of splitting into water and carbon dioxide. But with frequent drinking or drinking a large amount of alcohol, the liver cannot cope with detoxification, and acetaldehyde begins to accumulate in the body.
Taking Polysorb accelerates the elimination of toxins that are formed as a result of ethanol metabolism. If you drink the sorbent immediately before a feast, its microscopic particles will prevent ethanol from entering the bloodstream. The person will not get very drunk. When it enters the digestive tract, Polysorb increases the viscosity of liquids, which changes the consistency of intestinal contents. The resulting liquid with a new composition gently envelops the walls of the digestive tract.
Polysorb is able to remove the following toxins from the body:
- alcohol, including its metabolic products and derivatives;
- food allergens;
- toxins produced by bacteria and viruses;
- certain types of microorganisms;
- medicines;
- toxins, poisons;
- salts of heavy metals;
- radionuclides;
- some metabolic products, for example, bilirubin, cholesterol, nitrogenous compounds, etc.
This drug works softer and more effectively than activated carbon. It does not enter the bloodstream and leaves the body unchanged. Its most important tasks are the absorption and removal of poisons from the body.
The use of enterosorbents in the treatment of acute intestinal infections
In acute intestinal infectious diseases, the main clinical manifestations are determined by the syndrome of damage to the gastrointestinal tract (GIT): dyspepsia, vomiting, diarrhea, abdominal pain of various localizations [1]. In parallel with it, there may be varying degrees of severity of manifestations of feverish-intoxication syndrome, which is the reaction of the macroorganism to the causative agent of an infectious disease.
Dyspepsia syndrome is characteristic of salmonellosis, food poisoning, escherichiosis, rotavirus gastroenteritis and other viral diarrheas; it is also observed with various organic lesions and functional disorders of the gastrointestinal tract. Vomiting occurs due to inflammatory changes in the mucous membrane and increased secretion of fluid into the lumen of the upper gastrointestinal tract, as well as the development of intoxication syndrome. Most acute intestinal infections (AIE) are characterized by diarrhea. Based on the characteristics of the pathogenetic mechanisms, four types of diarrhea are distinguished: secretory, hyperexudative, hyperosmolar, hyper- and hypokinetic.
Secretory diarrhea is caused by increased secretion of sodium and water into the intestinal lumen. A classic example is diarrhea due to cholera, the causative agent of which, Vibrio cholerae, multiplies only on the surface of the epithelium of the small intestine, but cholera toxin disrupts intracellular regulation, as a result of which the intestinal epithelium begins to actively secrete water with electrolytes into the lumen. Hypersecretion of water and electrolytes is also caused by toxins of other bacteria (Salmonella, Escherichia, Klebsiella), enteropathogenic viruses, bile acids, prostaglandins and other biologically active substances. The secretory form is characterized by painless, profuse watery diarrhea, amounting to liters per day.
Hyperexudative diarrhea is characteristic of inflammatory bowel diseases. Develops in bacterial acute intestinal infections caused by Shigella, Salmonella, Clostridia, Escherichia and other bacteria. In this case, they are also called invasive (English invasion - invasion, invasion). The stool is liquid, often with pathological impurities (mucus, blood, pus). Similar diarrhea is also observed in non-infectious diseases: ulcerative colitis, Crohn's disease, malignant intestinal tumors.
Hyperosmolar (osmotic) diarrhea develops due to impaired absorption in the small intestine. Of the infectious agents, it is most often caused by rotaviruses, which multiply in the epithelium and disrupt the activity of enzymes in the intestinal mucosa. Because of this, disaccharides cannot be broken down into monosaccharides and absorbed. Disaccharides remain in the intestinal lumen and attract water. Under the influence of intestinal microflora, disaccharides ferment with the formation of gases (flatulence) and water, which leads to pain and “watery” diarrhea. Hyperosmolar diarrhea is observed with malabsorption syndrome, with a deficiency of digestive enzymes (congenital enteropathy, chronic pancreatitis, etc.). With osmotic diarrhea, the stool is copious, liquid, and often contains a large amount of semi-digested food residue.
Hyper- and hypokinetic diarrhea occurs when intestinal motility increases or decreases, which is accompanied by impaired transit of intestinal contents. Hyperkinetic diarrhea is caused by neurogenic factors (stress), laxatives, secretin, pancreozymin, gastrin, prostaglandins and serotonin. This type of diarrhea is common in patients with irritable bowel syndrome. With hyperkinetic diarrhea, the stool is liquid or pasty, frequent, but not abundant. Hypokinetic diarrhea is less common and is associated with excessive bacterial contamination of the small intestine.
The most important syndrome in acute diarrheal infections is dehydration (dehydration). There is a loss of water and electrolytes, which often leads to the development of metabolic acidosis. According to the classification of V.I. Pokrovsky (1978), there are four degrees of severity of dehydration: degree I corresponds to a loss of body weight not exceeding 3%; in grade II, the loss is 4–6% of body weight; at III - 7–9%; with IV - 10% or more. As a result of dehydration, hypovolemic shock may develop. Based on the pathogenesis of acute diarrheal infections, the basis of their treatment is rehydration therapy, which is aimed at restoring the water-electrolyte and acid-base state of the body. For these purposes, polyion crystalloid solutions are used for intravenous and oral use. Colloidal solutions are used only for detoxification purposes in cases where there are no signs of dehydration.
Antibacterial agents (antibiotics, fluoroquinolones, etc.) are used in the treatment of shigellosis, cholera, campylobacteriosis and yersiniosis; for other bacterial diarrheal infectious diseases they are ineffective, and for viral diarrhea they are contraindicated, since they can cause the development of dysbiosis.
To correct gastrointestinal disorders that develop during acute diarrheal infectious diseases, eubiotics, enzyme preparations, antispasmodics and a number of other groups of drugs are used in clinical practice, among which enterosorbents have become increasingly important in recent years.
Enterosorbents (Greek enteron-gut; Latin sorbens - absorbing) are substances with a high sorption capacity that are not destroyed in the gastrointestinal tract, effectively binding and removing endogenous and exogenous toxic compounds, supramolecular structures and cells from the body, used for treatment and disease prevention [2–4].
Enterosorbents as therapeutic agents have been known since ancient times. Even the healers of Ancient Egypt, India, and Greece used charcoal, clay, crushed tuff, and burnt horn internally to treat poisoning, diarrhea, jaundice and other diseases, as well as externally to treat wounds. Doctors of Ancient Rus' used birch or bone charcoal. Avicenna (Abu Ali ibn Sina) in his Canon of Medical Science, out of the seven postulates of the art of preserving health, put the method corresponding to the modern understanding of enterosorption in third place. In Russia, T. E. Lovitz (1785), studying the chemical properties of charcoal, substantiated its use for the same purposes.
The most important medical requirements for modern enterosorbents are high sorption capacity in relation to the removed components and the ability to sorb molecules and bacterial cells of different sizes and weights, the absence of toxic and traumatic effects on the mucous membranes of the gastrointestinal tract; they must be well evacuated from the intestines and not cause loss of beneficial ingredients or have a negative effect on secretion processes and intestinal microflora. As they pass through the intestines, bound components should not undergo desorption. Enterosorbents should not penetrate the gastrointestinal mucosa and therefore should not have systemic pharmacokinetics. Preparations for enterosorption must have a convenient dosage form and have good organoleptic properties [4].
The interaction of sorbents with the removed components is realized in four main ways: adsorption, absorption, ion exchange and complexation [5, 6]. During adsorption, the interaction between the sorbent and the substance being removed occurs at the interface. Absorption is the process of absorption of a substance by a liquid sorbent as a result of dissolution. Ion exchange is the process of replacing ions on the surface of the sorbent with sorbate ions. The pathogenetic mechanisms of enterosorption depend on the type of sorbent and the structure of the sorbed particles.
Sorbents have different properties and can differ in a number of ways [4].
By dosage form and physical properties: granules, powders, tablets, pastes, gels, suspensions, colloids, encapsulated materials, food additives.
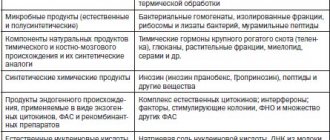
Based on their chemical structure, sorbents can be divided into several groups1:
- Carbon sorbents (activated carbon, Carbolong, Karbovit, Carbosphere, saturated spherical carbonite - SKN, Antralen, etc.).
Carbon sorbents based on activated carbon, granulated carbon and carbon fiber materials, like a sponge, absorb gases, toxins, metal salts, and drug metabolism products. Activated carbon preparations can be traumatic for the mucous membrane of the digestive tract, so their use is not recommended for erosive and ulcerative lesions of the gastrointestinal tract, hemorrhoidal bleeding.
- Silicon-containing enterosorbents (Polysorb, Sillard P, white clay, Smecta, Neosmectin, etc.).
Among silicon-containing enterosorbents, a distinction is made between natural and synthetic. The most famous natural clay is white clay (Kaolin), the suspension of which has enveloping and adsorbing properties. In addition to Kaolin, smectites (Smecta) and sodium montlorilonites (Bentonite), etc. are used in medicine.
- Sorbents of chemical origin (Enterodes, Enterosorb, Enterosgel).
Of the synthetic enterosorbents, the drug Enterosgel, which is a synthesized gel of methyl silicic acid hydroxide, is currently the most widely used. Possessing high sorption activity, it is characterized by a selective effect: it binds and removes only medium-molecular toxic substances.
- Sorbents based on natural and synthetic resins, synthetic polymers and indigestible lipids (Cholestyramine, Cholestipol, Cholesivilam, etc.).
Enterosorbents based on resins, polymers and indigestible lipids are ion-exchange materials capable of binding specific substances (anion exchangers are good at reducing the acidity of gastric juice, absorbing pepsin and bacterial toxins; Cholesteramine binds bile acids; cation exchangers can reduce the content of sodium, potassium, calcium ions.
- Natural organic sorbents based on dietary fiber, hydrolyzed lignin, chitin, pectins and alginates (microcrystalline cellulose - MCC, Polyphepan, Multisorb, Extralact, Algisorb, Zosterin, Mycoton, Filtrum-STI, etc.).
Dietary fiber - polysaccharides and lignin. Natural dietary fiber is not digested by digestive enzymes, is not absorbed by the human digestive system, and is fermented by intestinal bacteria. The most important property of dietary fiber is the ability to actively absorb and retain water (adsorption) and other substances: nitrites, nitrates, carcinogens, bacterial toxins.
Types of dietary fiber
Cellulose is an unbranched polymer of glucose containing up to 10 thousand monomers. Different types of cellulose have different properties and different solubility in water.
Hemicellulose is formed by the condensation of pentose and hexose residues, with which arabinose, glucuronic acid and its methyl ester residues are associated. Just like cellulose, different types of hemicellulose have different physicochemical properties.
Gums (gums) are branched polymers of glucuronic and galacturonic acids, to which are attached residues of arabinose, mannose, xylose, as well as magnesium and calcium salts; found mainly in seaweeds and seeds.
Mucilages (neutral and acidic) are branched, sulfated arabinoxylans; are polysaccharides of seeds and seaweeds.
Pectins are a complex of colloidal polysaccharides based on galacturonic acid with side chains of rhamnose, arabinose, xylose and fructose. Pectin substances are part of the cell walls and interstitial matter of higher plants. Pectins are gelling agents. Pectins are easily broken down by bacteria in the colon.
Alginates are salts of alginic acids, the molecule of which is represented by a polymer of polyuronic acids, found in large quantities in brown algae. Alginates have the ability to bind and remove radionuclides and heavy metals from the body.
Lignin is a polymeric residue of wood after its percolation hydrolysis, which is carried out to isolate cellulose and hymicellulose.
According to their physicochemical properties, dietary fibers are divided into water-soluble (pectins, gums, mucus, hemicellulose fractions), they are conventionally called “soft” fibers, and insoluble (cellulose, part of hemicellulose, lignin), the so-called “coarse” fibers.
- Combined sorbents contain two or more types of sorbents or additional components (vitamin C, enzymes, probiotics, fructooligosaccharides, lactulose, etc.) that expand the spectrum of therapeutic or preventive action of the enterosorbent (Ultrasorb, Entegnin-N, Laktofiltrum, Filtrum-Safari, Rekitsen -RD, White coal, Eubicor, etc.).
Based on selectivity, sorbents are classified into non-selective, selective monofunctional, selective, bi- and polyfunctional.
The main route of administration of enterosorbents is oral; sometimes enterosorbent is administered through a tube when the patient is unable to take the drug independently or there are obstacles due to stenosis of the esophagus or pyloric stomach. With probe administration, the sorbent can be removed (usually with an exposure of up to 30 minutes) and a new portion of the drug can be introduced. Sometimes, according to indications, enterosorbents are administered through enemas into the colon.
The therapeutic effect of enterosorbents is achieved as a result of their direct and indirect effects on pathogenetic mechanisms.
The direct action of enterosorbents is aimed at binding and eliminating from the gastrointestinal tract toxic products of metabolism and the inflammatory process, pathogenic bacteria and their toxins, viruses, biologically active substances, binding gases formed in excess during the putrefactive process.
The indirect effect is due to the prevention or weakening of the clinical manifestations of endotoxemia, toxic-allergic reactions, and diarrhea syndrome. The use of enterosorbents reduces the metabolic load on the liver and kidneys, helps normalize the motor, evacuation and digestive functions of the gastrointestinal tract, and has a positive effect on the functional state of the immune system [4, 6, 7].
Enterosorption is part of the group of efferent therapy (lat. efferens - remove), i.e. therapeutic measures, the purpose of which is to stop the action of toxins of various origins and their elimination from the body. Enterosorption for intestinal infectious diseases is a pathogenetically substantiated method of therapy.
We began targeted clinical studies to study the effectiveness of domestic enterosorbents back in the mid-80s of the last century [8, 9]. At that time, only carbon sorbents were used in practice, which, along with positive properties, had a relatively low sorption capacity and side effects and a number of contraindications. The creation of new drugs, derivatives of other groups of sorbents, has expanded the possibilities of using enterosorption in the complex treatment of acute intestinal infections. The first of these we used was Enterodes, a drug of low molecular weight polyvinylpyrrolidone, which was used in the complex therapy of 144 patients with acute intestinal infections (men - 71, women - 73), 124 of whom were diagnosed with foodborne toxic infection, 20 with shigellosis. In 105 (72.9%) the course of the disease was of moderate severity, in 37 (25.9%) it was mild, and in 2 (0.015%) it was severe. The drug was prescribed, as recommended by the manufacturer, in dissolved form (5 g in 100 ml of water) 2-4 doses per day for 3 days. The therapeutic effect was registered in all patients: abdominal pain, flatulence, nausea, vomiting were relieved; 6–12 hours after the start of treatment, body temperature returned to normal in 75.6% of patients. All patients who received enterodesis treatment on the first or second day of illness did not require parenteral rehydration. The pronounced clinical effect and the absence of adverse reactions (also controlled by laboratory biochemical studies) made it possible to include this drug in a complex of drugs for the treatment of patients with acute diarrheal infections.
According to infectious disease doctors and pediatricians, timely, i.e., early use of enterosorbents for acute infectious diarrheal diseases of the invasive type has a rapid and pronounced detoxification, hypothermic and antidiarrheal clinical effect [3, 10–12]. Such results were obtained with the combined use of enterosorbents with antibacterial drugs or probiotics in the treatment of acute intestinal infections. According to some authors, the clinical effectiveness of enterosorbents in mild and moderate forms of acute intestinal infections is not inferior to antibacterial drugs widely used in clinical practice [13, 14].
A. A. Novokshonov et al. (2002) used the enterosorbent Filtrum-STI to treat 60 children with mild and moderate forms of acute intestinal infections, of which 40 patients received the drug as a means of etiotropic monotherapy (20) or in combination with furazolidone (20). It has been established that “etiotropic” monotherapy with enterosorbent is more effective than treatment with furazolidone, and is significantly increased when used together in the treatment of moderate forms of acute intestinal infections of bacterial etiology of the invasive type of diarrhea. Along with the rapid and pronounced detoxification clinical effect, the sanitizing effectiveness of combination therapy also noticeably increased: re-seeding of ACI pathogens was not registered, while with monotherapy with furazolidone, in a third of patients at the end of the 5-day course, re-seeding of salmonella and Pseudomonas aeruginosa occurred. Authors about [15].
In the complex treatment of 63 patients aged 19 to 34 years admitted to the hospital with a diagnosis of foodborne toxic infection, we also used the drug Filtrum-STI. As a control, a group of 23 patients was observed, corresponding in age and other criteria to the first group, who received detoxification and rehydration therapy. Due to the fact that, according to clinical and epidemiological characteristics confirmed by laboratory tests, the etiological agents were opportunistic bacteria or rotaviruses (in 14 cases), antibacterial drugs were not prescribed to the patients. All patients were admitted in a state of moderate severity. Treatment with enterosorbent Filtrum-STI was carried out in accordance with the manufacturer’s recommendation: 2–3 tablets. 3 times a day an hour before meals and taking other medications. The average duration of drug use was 4 ± 0.3 days. As a result, in patients receiving enterosorbent, a decrease in the duration of fever and manifestations of intoxication was recorded to 2.3 ± 0.4 days, in the control group this figure was 3.2 ± 0.3 days (p > 0.05), the duration of diarrhea was reduced , which in the groups under consideration was 1.6 ± 0.5 and 2.8 ± 0.7 days, respectively (p > 0.05). The use of enterosorbent contributed to an earlier cessation of pain syndrome - after 1.4 ± 0.2 days (p < 0.05), which in patients in the control group lasted up to 2.6 ± 0.3 days, the disappearance of such manifestations as flatulence - 1.9 ± 0.2 days (p < 0.05), in the control group - up to 3.7 ± 0.4 days, lethargy and anorexia 1.8 ± 0.3 and 3.1 ± 0, 4 days (p < 0.05), respectively. The drug was well tolerated, no adverse reactions were noted. Thus, the inclusion of the enterosorbent Filtrum-STI in the complex treatment of patients with foodborne toxic infections had an obvious therapeutic effect, expressed in a decrease in the time it took for the manifestations of intoxication and functional disorders of the gastrointestinal tract to disappear.
The given examples of the use of the drug Filtrum-STI indicate the good effectiveness of an enterosorbent based on hydrolytic lignin - a polymer of plant origin with a high sorption capacity, capable of removing toxins, pathogenic microorganisms, and their metabolic products from the body, as well as helping to restore microflora and normalize intestinal motility. Drugs of this group are actively being introduced into medical practice, especially in pediatrics, since they can be prescribed to children starting from infancy.
In domestic guidelines on infectious diseases, manuals for doctors and special scientific literature of recent years, recommendations on the use of enterosorbents in the complex treatment of acute infectious diarrheal diseases are constantly present [16–18]. However, it should be noted that the list of recommended drugs is relatively small. There is little information about their use in intestinal infectious diseases of a viral nature, which, as many researchers have shown, occupy a significant proportion among diarrheal diseases. Thus, in Moscow in 2010, compared with the previous year, the incidence of rotavirus gastroenteritis increased by more than 50%; Norwalk virus was recorded 1.8 times more often [19]. In this regard, more research has been carried out by infectious disease pediatricians, which is quite natural given the wider spread of viral diarrheal diseases among children. Currently, for these diseases, specific immunoglobulins, interferon inducers and drugs with immunomodulatory effects are used as etiotropic therapy, and probiotics and enterosorbents are used for etiopathogenetic therapy. It should be taken into account that not all known enterosorbents are quite effective against viral diarrheal diseases, but some of them have a noticeable etiotropic effect, which is due to the ability to sorption and elimination of viruses and opportunistic bacteria from the intestine. A number of enterosorbents (dioctahedral smectite, preparations based on hydrolytic lignin) prevent the penetration of viruses through the protective mucous barrier of the intestine, absorb excess disaccharides, intestinal gases, reduce flatulence and associated abdominal pain; normalize the absorption of water and electrolytes, the composition of the intestinal microflora; have a pronounced detoxification and antidiarrheal clinical effect.
L. N. Mazankova et al. [10] noted a noticeable positive effect when using enterosorbent Filtrum-STI in the treatment of acute intestinal infections in children, where the etiological agents were bacteria and rotaviruses. Enterosorbent was prescribed to patients from the moment of admission against the background of oral rehydration and diet therapy. Already from the first days of treatment, a positive effect of the drug on general toxic and local acute intestinal syndromes was noted in the form of relieving fever, reducing the frequency or completely stopping vomiting, improving appetite, eliminating abdominal pain and flatulence, reducing the frequency of bowel movements and improving the general condition of patients.
According to V.F. Uchaikin et al. (2008), the inclusion of another well-known enterosorbent - the drug Neosmectin (dioctahedral smectite) in the complex therapy of acute intestinal infections of viral (osmotic) and viral-bacterial etiology (invasive-osmotic type of diarrhea) in children contributes to a more rapid disappearance of symptoms of intoxication and exicosis, fever, and relief of symptoms flatulence, abdominal pain and diarrhea syndrome. The normal intestinal flora (bifidobacteria, lactobacilli, enterococci) is restored faster than in the control group that did not receive Neosmectin [4].
Ioannidi E. A. et al. (2011) used Neosmectin to treat patients with bacterial acute intestinal infections caused by Proteus mirabilis, P. vulgaris, Citrobacter freundi, Klebsiella pneumoniae and other opportunistic bacteria. The inclusion of this enterosorbent had a positive effect on the course of the disease: it reduced the duration of intoxication and dyspeptic syndromes, shortened the time of hospitalization of patients, which indicates the effectiveness of this drug for diarrhea of various etiologies [20].
Ratnikova L. I. and Permitina M. I. (2011) positive results in the treatment of various acute intestinal infections were obtained as a result of the use of the drug Polysorb, which, when administered early, had a pronounced detoxification effect against salmonellosis, foodborne toxic infection caused by opportunistic bacteria, and botulism. Currently, there are numerous studies by other authors with similar results of the effective use of enterosorbents of different groups for the treatment of patients with acute intestinal infections of various etiologies.
In recent years, special attention has been paid to the development and introduction into clinical practice of combined enterosorbents, in which, in addition to the main active drug - the sorbent, additional components have been introduced that expand their range of therapeutic and preventive effects: Entegnin-N (lignin + ascorbic acid), Rekitsen-RD (pectin + a complex of vitamins and microelements, essential amino acids and wine yeast - Saccharomyces vini), White coal (silicon dioxide + microcrystalline cellulose), Calcium Algylose-C (alginic acid + fiber and calcium), etc. A relatively new domestic combination preparation is noteworthy Filtrum-Safari (chewable lozenges). This drug combines the properties of an enterosorbent and a prebiotic due to the content of lignin, known for its sorption and detoxification properties, and fructooligosaccharide, which helps restore the quantitative and qualitative composition of the intestinal microflora. The drug was created for use in pediatrics, is available in the form of lozenges with chocolate or forest berry flavors, and is hypoallergenic. Another drug from this group, Lactofiltrum, in addition to lignin, contains lactulose, which also has a prebiotic effect.
A. A. Novokshonov et al. (2009) studied the clinical effectiveness of enterosorbent Filtrum-Safari in the complex therapy of sick children with established rotavirus infection. A total of 45 children aged from three to 13 years were studied. It has been established that the inclusion of the drug Filtrum-Safari in complex therapy contributes to a statistically significant reduction in the duration of symptoms of intoxication, toxicosis with exicosis, diarrhea syndrome and the average duration of the acute period of the disease. The drug is convenient for use in pediatrics and has virtually no adverse reactions [22].
Most modern enterosorbents are known to practicing doctors of various specialties. However, many registered enterosorbents have not yet found widespread use due to various reasons: due to insufficient awareness of hospital doctors about the role of enterosorbents in the treatment of infectious and non-infectious diseases of the gastrointestinal tract, ignorance of the advantages and disadvantages of certain sorbents for specific pathologies, and actually still existing skepticism doctors' attitudes towards enterosorption. In one of the conclusions of Academician of the Russian Academy of Medical Sciences V.F. Uchaikin et al. [4]. against pathogenic bacteria and viruses."
Literature
- Yushchuk N. D., Rosenblum A. Yu. Syndrome of gastrointestinal tract damage in infectious diseases. In: Infectious diseases: a national guide. Ed. N. D. Yushchuk. Yu. Ya. Vengerova. M.: GEOTAR-Media. pp. 276–282.
- Belyakov N. A., Solomennikov A. V. Enterosorption - the mechanism of therapeutic action // Efferent therapy. 1997, vol. 3, no. 2.
- Uchaikin V.F., Novokshonov A.A., Sokolova N.V. Enterosorption is an effective method of etiopathogenetic therapy of acute intestinal infections // Det. infections. 2005. No. 3. P. 39–43.
- Uchaikin V.F., Novokshonov A.A., Sokolova N.V., Berezhkova T.V. Enterosorption - the role of enterosorbents in the complex therapy of acute and chronic gastroenterological pathology. A manual for doctors. M., 2008. 24 p.
- Enterosorption. Under. ed. N. A. Belyakova. Leningrad. 1991. 329 p.
- Khotimchenko Yu. S., Kropotov A. V. Application of enterosorbents in medicine // Pacific Medical Journal. 1999, no. 2, p. 84–89.
- Nikolaev V. G. et al. Enterosorption: state of the issue and prospects for the future // Bulletin of problems of biology and medicine. 2007. No. 4, p. 7–17.
- Loban K. M., Miterev Yu. G., Zherebtsov L. A. et al. Efficacy of the drug “Entero dez” for acute intestinal infections // Hematology and Transfusiology. 1983, no. 7, pp. 33–39.
- Popova S.P., Tokmalaev A.K. Oral detoxification therapy for acute intestinal infections // Soviet Medicine. 1987, no. 6, p. 89–91.
- Mazankova L.N., Pavlova A.A. Improvement of pathogenetic therapy of acute intestinal infections in children // Children's infections. 2006, 4, p. 67–69.
- Uchaikin V.F. et al. The place and significance of enterosorption in the etiopathogenetic therapy of acute intestinal infections // Pediatrics. 2007, 86 (2), p. 44–50.
- Vatutina O.V., Luchshev V.I., Burova S.V. Effect of enterosorbent filtrum on the level of specific endotoxemia in patients with Flexner’s shigellosis / Sat. mat. XIV congr. "Man and Medicine." M., 2007. P. 536.
- Zaitseva I. A., Koshkin A. P., Levin D. Yu. The use of enterosorbent “Filtrum” in the complex therapy of acute intestinal infections in children // Children's infections. 2005, No. 1, p. 61–62.
- Novokshonov A. A. et al. The role of enterosorbents in the complex therapy of acute intestinal infections in children // Pediatric Practice. 2008, No. 5, p. 20–26.
- Novokshonov A. A., Portnykh O. Yu., Sokolova N. V. Study of the clinical effectiveness of the oral sorbent “Filtrum” for acute intestinal infections in children / Collection of works “Application of the enterosorption method in practical medicine.” M., 2002. pp. 24–31.
- Infectious diseases: national guidelines / Ed. N. D. Yushchuk. Yu. Ya. Vengerova. M.: GEOTAR-Media, 2009. 1056 p.
- Rational pharmacotherapy of childhood diseases: Handbook. for medical practitioners / Ed. ed. A. A. Baranova, N. N. Volodina, G. A. Samsygina M.: Litterra, 2007. T. 1. 1088 p.
- Guide to infectious diseases / Ed. Yu. V. Lobzin 3rd ed., add. And reworked. St. Petersburg: Foliant Publishing House. 2003. 1040 p.
- Gruzdeva O. A., Maryin G. G. Features of the incidence of acute intestinal infections in a modern metropolis / Materials of the III Annual All-Russian Congress on Infectious Diseases. Moscow, March 28–30, 2011. P. 83.
- Ioannidi E. A., Makarova I. V., Timonova M. S. Clinical use of enterosorbent for acute intestinal infections / Materials of the III Annual All-Russian Congress on Infectious Diseases. Moscow, March 28–30, 2011. pp. 152–153.
- Ratnikova L.I., Permitina. Enterosorption in the treatment of intoxication syndrome // Materials of the III Annual All-Russian Congress on Infectious Diseases. Moscow, March 28–30, 2011. pp. 306–307.
- Novokshonov A. A., Sokolova N. V., Berezhkova T. V., Sakharova A. A. Clinical effectiveness of a new enterosorbent in the complex therapy of acute intestinal infections of viral etiology in children // Treating Doctor. 2009, no. 7, pp. 78–80.
A. K. Tokmalaev, Doctor of Medical Sciences, Professor of RUDN University , Moscow
Contact information about the author for correspondence
1 Detailed information on registered drugs is available in the relevant reference literature, guidelines and manuals for doctors.
Polysorb dosage
The dosage regimen is determined by the doctor based on the severity of the patient’s condition. Usually the powder is prescribed for:
- severe intoxication in purulent and septic diseases;
- poisoning with alcohol and its surrogates;
- food infections;
- acute intestinal infections;
- poisoning with drugs, potent substances, salts of heavy metals, radionuclides, medicinal plants and mushrooms;
- nonspecific diarrhea.
- hepatitis of various natures.
The average daily dose for an adult is calculated based on his weight. The optimal dosage is 0.2 g per 1 kilogram of body weight per day, but not more than 20 g. It is necessary to take the sorbent 3 - 4 times a day, at regular intervals.
Nosological classification (ICD-10)
- A05.9 Bacterial food poisoning, unspecified
- B19 Viral hepatitis, unspecified
- K59.1 Functional diarrhea
- K63.8.0* Dysbacteriosis
- N18 Chronic renal failure
- R17 Unspecified jaundice
- T50.9 Other and unspecified drugs, medicinal products and biological substances
- T50.9.0* Alkaloid poisoning
- T51 Toxic effects of alcohol
- T56.9 Toxic effect of unspecified metal
- T65.9 Toxic effects of unspecified substance
- T78.4 Allergy, unspecified
- Y57 Adverse reactions during therapeutic use of other and unspecified drugs and medications
- Y97 Factors associated with environmental pollution
- Z57 Occupational exposure to hazards
Methods of taking Polysorb
The oral suspension should be prepared immediately before use. The required dose of the medicine is mixed in 0.5 glasses of clean water, stirred and drunk. This medication should be taken one hour before meals or other medications. The course of treatment depends on the severity of the patient’s condition, but no more than two weeks. If you need to continue taking Polysorb, you should consult a doctor.
Polysorb has a positive effect on the functioning of the immune system, reduces the incidence of unwanted allergic reactions to medications, and improves the patient’s quality of life.
In case of acute poisoning, Polysorb cannot be considered as the only treatment. If the patient did not have time to drink the suspension before meals, it should be taken 2 hours after meals or taking medications.
Taking Polysorb during alcohol intoxication
Acute poisoning with ethyl alcohol can often lead to death. Poisoning with methyl and other alcohols, which are part of counterfeit alcoholic drinks, is especially dangerous. Ingestion of 10 ml of methanol leads to severe poisoning, one of the consequences of which is blindness. Taking enterosorbents allows you to achieve the following effects:
- binding of alcohols in the stomach and intestines;
- normalization of glutathione levels;
- restoration of biological blood parameters;
- preventing the primary absorption of alcoholic beverages;
- decrease in the concentration of ethyl alcohol in the blood;
- preventing the circulation of breakdown products of ethyl alcohol in the body;
- significant reduction in the half-life of alcohol (about 2 times).
Taking Polysorb improves tolerance to alcoholic beverages. In humans, the severity of symptoms of ethanol poisoning decreases. Modern use of Polysorb helps prevent deterioration of the body's condition.
In case of alcohol poisoning, the suspension is used according to the following scheme: before drinking alcohol, during libation and in the morning, after the holiday.
The inclusion of Polysorb in the complex therapy of alcohol poisoning helps to reduce the duration of alcoholic coma, improve the dynamics of restoration of cardiac and vascular functions, and reduce the length of stay of patients in a hospital.
In the case of chronic alcohol intoxication, the combination of the basic treatment regimen with Polysorb helps to reduce the hospital stay of patients, reduce the number of intravenous and infusion drugs administered, and improve the dynamics of restoration of heart and kidney functions.
Features of the use of Polysorb for hangover and withdrawal syndrome
Any case of alcohol abuse ends in a hangover, or post-intoxication syndrome. In the mechanism of development of this syndrome, the breakdown products of ethyl alcohol play a crucial role. The most toxic of them is acetaldehyde. During the further breakdown of this substance, free radicals are released, which further aggravate the patient's condition.
Against the background of intoxication, a person’s functioning of all internal organs is disrupted. Polysorb effectively removes alcohol breakdown products. Due to its biochemical properties, the drug binds toxins that are released into the blood against the background of impaired liver and kidney function.
In case of a hangover, Polysorb does not act on alcohol, but on the products that are formed during its breakdown. According to the instructions for use of this product, the suspension should be taken no later than 6 hours after finishing drinking alcohol. Or do this on the eve of a violent libation.
In case of acute alcohol poisoning due to a hangover, Polysorb actively removes toxins and eliminates the following symptoms:
- pronounced surges in blood pressure;
- headache;
- trembling of limbs;
- lethargy;
- weakness;
- sweating;
- swelling, especially noticeable on the face;
- thirsty;
- bowel disorders;
- neuropsychiatric disorders.
If you drink too much alcohol, the liver cannot process ethanol. Drinking the drug significantly alleviates the human condition and promotes faster normalization of body functions. Consuming Polysorb immediately after a stormy feast does not have a pronounced effect: small colloidal particles act in the intestines, and toxins have time to penetrate the blood. But even in this case, the medicine helps the liver function
Polysorb effectively relieves symptoms of withdrawal syndrome when stopping alcohol consumption. This promotes faster recovery of the body. However, the drug is not able to remove acetaldehyde and acetic acid from the blood - substances formed during the breakdown of alcohol.
For a hangover, the standard dose for an adult is 2 tablespoons of powder dissolved in 150 liters of water. The action begins within half an hour after oral administration.
For alcoholism, Polysorb should be taken 3–4 times a day for 5–10 days or until the patient’s condition is relatively normal. All this time, it is recommended to drink more fluid, because a significant amount of it is spent on maintaining the activity of the microparticles of the drug.
Release form
Powder for the preparation of suspension for oral administration. 1/2/3/6/10/12 g in disposable bags made of label paper with a thermal layer. 1/2/3/4/5/10/30/50/100 disposable bags per cardboard box. It is allowed to place disposable bags directly into group packaging.
50 g in double PE bags or 5/10 kg in double PE bags (for hospitals). Packages of 50 g are placed in a cardboard box.
Also 12/15/20/25/30/35/40/45/50 g in polystyrene, PE or PET jars, sealed with lids made of similar materials. The jar is placed in a cardboard box or packed in shrink film in packs of 5 and 10 pcs.
Contraindications to the use of the drug Polysorb
Ubiquitous advertising claims that this product is completely safe for humans. However, after carefully reading the instructions for use of this powder, you may find such contraindications to the use of Polysorb.
- Active phase of exacerbation of gastric or duodenal ulcer.
- Intestinal atony is a condition in which there is a lack of intestinal tone and peristalsis. It develops against the background of endocrine or neurological diseases or as a side effect of other medications.
- Bleeding from the upper digestive tract.
- Intestinal obstruction.
- Individual intolerance to the drug, tendency to allergic reactions.
A suspension prepared from Polysorb powder cannot be absorbed from the digestive tract. Its use is approved for pregnant and lactating women. For children, adolescents and people with severe chronic pathologies, the dose is selected or adjusted only by the attending physician.
Indications and contraindications
With all its positive properties, Polysorb is still a full-fledged medicinal product, and this information cannot be ignored.
Indications:
- alcohol poisoning;
- allergies;
- viruses;
- hazardous working conditions associated with the chemical industry;
- hepatitis (the level of bilirubin in the body increases, which is neutralized by Polysorb);
- purulent diseases;
- dermatitis;
- diarrhea;
- dysbacteriosis;
- long course of antibiotic treatment;
- infections;
- disturbances in the gastrointestinal tract;
- weakened immune system;
- drug overdose;
- liver failure;
- food intoxication;
- hangover;
- renal failure (causes the accumulation of urea in the body, which this drug copes well with);
- living in environmentally unfavorable areas;
- psoriasis;
- toxicosis;
- eczema.
Contraindications:
- individual intolerance;
- intestinal obstruction;
- bleeding in the gastrointestinal tract;
- violation of the evacuation function of the intestines, which is manifested by constipation, bloating, flatulence, pain in the abdomen;
- exacerbation of ulcers;
- oncology;
- severe vomiting.
If you have a history of diseases from the list of indications, cleansing the body with Polysorb will also become a course of treatment. Especially often, grateful users note its high effectiveness against allergies. By eliminating allergens, it relieves rashes, tearing and other symptoms of this disease, that is, it has an antihistamine effect.
Pregnant women, with the permission of their doctor, can take the powder in order to get rid of toxicosis and at the same time cleanse the intestines and amniotic fluid of organic debris.
It is equally important to observe contraindications. If you do not take them into account, instead of cleansing, you can get an exacerbation of existing diseases, deterioration of well-being, and even side effects.
If you are not sure about the need to cleanse the body, it is better to seek advice from an endocrinologist, gastroenterologist, or simply a therapist. Despite the fact that the drug is sold without a prescription, it is classified as a medicinal drug. This means that a doctor should recommend it.
Side effects from taking Polysorb
In most cases, the drug is well tolerated by patients. In some cases, the following side effects may occur:
- constipation (its risk occurs with atony of the digestive tract);
- acute allergic reaction in the form of rash, swelling, itching of the skin and mucous membranes;
- dyspeptic symptoms (most often manifested in the form of nausea, discomfort, or pain in the upper parts of the digestive tract, early satiety with food, flatulence, a feeling of constant fullness in the stomach when eating even a small amount of food;
- constant unpleasant taste in the mouth.
Polysorb has a non-selective effect. This means that it removes from the digestive tract not only poisons, but also substances necessary for the body. Therefore, doctors do not recommend long-term use of this drug (for more than two weeks in a row). Otherwise, the absorption of microelements, vitamins, and essential nutrients is impaired. If further use of Polysorb is necessary, patients will be prescribed supplements containing vitamins and microelements.
Compatibility of Polysorb with other drugs
Most drugs in the enterosorbent group reduce the effectiveness of any drug if taken simultaneously. Polysorb and its analogs are capable of adsorbing inorganic compounds. To avoid this interaction, it is recommended to use Polysorb one and a half to two hours before or after taking the main medications. If treated in a hospital, the responsibilities of medical personnel include monitoring the patient’s correct intake of Polysorb and other medications. Usually, in a clinical setting, errors with taking sorbents and other medications are completely excluded.
Polysorb is an effective and safe remedy for the treatment of hangover syndrome. It is a first aid drug for alcohol intoxication: headache, hand tremors, facial swelling, thirst, irritability. However, you should not use it often, because in this case useful substances are removed from the body. If it is necessary to use Polysorb for a long time, then it is necessary to additionally prescribe vitamin and mineral complexes. They will help restore water and electrolyte balance in the body and prevent the development of chronic pathologies of the digestive tract.
But treating alcoholism with Polysorb alone is inappropriate. This is only a symptomatic remedy that temporarily relieves the symptoms of excessive alcohol consumption. If a patient suffers from alcoholism, then he needs specialized treatment.
Information about the drug
Polysorb is a new generation universal enterosorbent. Sorption capacity is 300 mg/g, which is several times higher than that of other similar drugs. The main active ingredient is colloidal silicon dioxide. It is produced without additional ingredients, so there are no “chemicals” in its composition.
It is a white, slightly grayish or bluish-tinged odorless powder.
Designed for detoxification in cases of poisoning of various etiologies. But its ability to remove up to 95% of harmful substances is often used to cleanse the body and lose weight.
Available in 3 g sachets costing approximately $0.6 per piece. (10 sachets per package), as well as plastic jars:
- 12 g (ideal for a child) - $2.1;
- 25 g (can be purchased for a home first aid kit in case of poisoning) - $3.6;
- 35 g (recommended for the treatment of diseases) - $4.4;
- 50 g (can be used for complete cleansing of the body and weight loss) - $6.2.
Sold in pharmacies without a prescription.




![Table 1. Comparison of the results of treatment with Tribestan for men with oligoasthenozoospermia [7] with mod.](https://ms-pi.ru/wp-content/uploads/tablica-1-sravnenie-rezultatov-lecheniya-tribestanom-muzhchin-s-oligoastenozoospermiej-7-330x140.jpg)

