Circulation is the movement of blood in the human body. It consists of three main parts: blood, blood vessels (arteries, veins, capillaries) and the heart.
We decided to prepare educational material so that each of you is aware of all the nuances of the cardiovascular system. This is important so that you can understand in time what problem you could or may encounter in the future, and also so that the terminological expressions of our specialist during a face-to-face consultation do not seem like a foreign language to you.
What are blood vessels?
Vessels are tube-like formations that extend throughout the human body and through which blood moves. The pressure in the circulatory system is very high because the system is closed. Through this system, blood circulates quite quickly.
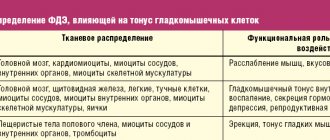
After many years, obstacles to the movement of blood - plaques - form on the vessels. These are formations on the inside of blood vessels. Thus, the heart must pump blood more intensively in order to overcome obstacles in the blood vessels, which disrupts the functioning of the heart. At this point, the heart can no longer deliver blood to the organs of the body and cannot cope with its work. But at this stage it is still possible to recover. The vessels are cleansed of salts and cholesterol deposits.
When the blood vessels are cleansed, their elasticity and flexibility returns. Many diseases associated with blood vessels go away. These include sclerosis, headaches, a tendency to heart attack, and paralysis. Hearing and vision are restored, varicose veins are reduced. The condition of the nasopharynx returns to normal.
Heart
The heart is the organ that pumps blood from the veins to the arteries. Thanks to the work of the heart, blood is supplied to the organs through arteries and capillaries. It is like a powerful pump and consists of muscle tissue - the myocardium. The heart pumps about 5 liters of blood per minute. An abrupt stop in its work is fraught with fatal consequences - myocardial infarction or heart attack often ends in the death of a person.
Human blood vessels
Blood circulates through the vessels that make up the systemic and pulmonary circulation.
All blood vessels consist of three layers:
- The inner layer of the vascular wall is formed by endothelial cells; the surface of the vessels inside is smooth, which facilitates the movement of blood through them.
- The middle layer of the walls provides the strength of blood vessels and consists of muscle fibers, elastin and collagen.
- The upper layer of the vascular walls is made up of connective tissue; it separates the vessels from nearby tissues.
Arteries
The walls of arteries are stronger and thicker than those of veins, since blood moves through them with greater pressure. Arteries carry oxygenated blood from the heart to the internal organs. The arteries of the dead are empty, which is revealed at autopsy, so it was previously believed that the arteries were air tubes. This is reflected in the name: the word “artery” consists of two parts; translated from Latin, the first part “aer” means air, and “tereo” means to contain.
Depending on the structure of the walls, two groups of arteries are distinguished:
- The elastic type of arteries are vessels located closer to the heart, these include the aorta and its large branches. The elastic framework of the arteries must be strong enough to withstand the pressure with which blood is thrown into the vessel from heart contractions. The elastin and collagen fibers that make up the frame of the middle wall of the vessel help resist mechanical stress and stretching.
Thanks to the elasticity and strength of the walls of the elastic arteries, blood continuously flows into the vessels and ensures constant circulation to nourish organs and tissues and supply them with oxygen. The left ventricle of the heart contracts and forcefully throws a large volume of blood into the aorta, its walls stretch to accommodate the contents of the ventricle. After relaxation of the left ventricle, blood does not flow into the aorta, the pressure is weakened, and blood from the aorta flows into other arteries into which it branches. The walls of the aorta regain their previous shape, since the elastin-collagen framework provides their elasticity and resistance to stretching. Blood moves through the vessels continuously, coming in small portions from the aorta after each heartbeat.
The elastic properties of the arteries also ensure the transmission of vibrations along the walls of the vessels - this is the property of any elastic system under mechanical influences, which is the cardiac impulse. The blood hits the elastic walls of the aorta, and they transmit vibrations along the walls of all the vessels of the body. Where the vessels come close to the skin, these vibrations can be felt as a weak pulsation. Pulse measurement methods are based on this phenomenon.
- Muscular-type arteries in the middle layer of the walls contain a large number of smooth muscle fibers. This is necessary to ensure blood circulation and continuity of its movement through the vessels. Muscular-type vessels are located further from the heart than elastic-type arteries, so the force of the cardiac impulse in them weakens; to ensure further movement of blood, contraction of muscle fibers is necessary. When the smooth muscles of the inner layer of the arteries contract, they narrow, and when they relax, they expand. As a result, blood moves through the vessels at a constant speed and promptly enters organs and tissues, providing them with nutrition.
Another classification of arteries determines their location in relation to the organ to which they supply blood. Arteries that pass inside an organ, forming a branching network, are called intraorgan. The vessels located around the organ, before entering it, are called extraorgan. Lateral branches that arise from the same or different arterial trunks may reconnect or branch into capillaries. At the point of their connection before they begin to branch into capillaries, these vessels are called anastomosis or anastomosis.
Arteries that do not have an anastomosis with adjacent vascular trunks are called terminal. These, for example, include the arteries of the spleen. The arteries that form the anastomosis are called anastomosing; most arteries belong to this type. The terminal arteries have a greater risk of blockage by a blood clot and a high predisposition to a heart attack, which can result in the death of part of the organ.
In the last branches, the arteries become very thin; such vessels are called arterioles, and the arterioles already pass directly into capillaries. Arterioles contain muscle fibers that perform a contractile function and regulate the flow of blood into the capillaries. The layer of smooth muscle fibers in the walls of arterioles is very thin compared to an artery. The place where the arteriole branches into capillaries is called the precapillary; here the muscle fibers do not form a continuous layer, but are located diffusely. Another difference between a precapillary and an arteriole is the absence of a venule. The precapillary gives rise to numerous branches into the smallest vessels - capillaries.
Capillaries
Capillaries are the smallest vessels, the diameter of which varies from 5 to 10 microns; they are present in all tissues, being a continuation of the arteries. Capillaries provide tissue metabolism and nutrition, supplying all structures of the body with oxygen. In order to ensure the transfer of oxygen and nutrients from the blood to the tissues, the capillary wall is so thin that it consists of only one layer of endothelial cells. These cells are highly permeable, so through them substances dissolved in the liquid enter the tissues, and metabolic products return to the blood.
The number of working capillaries in different parts of the body varies - they are concentrated in large numbers in working muscles, which need constant blood supply. For example, in the myocardium (the muscular layer of the heart) up to two thousand open capillaries are found in one square millimeter, and in skeletal muscles there are several hundred capillaries in the same area. Not all capillaries function at the same time - many of them are in reserve, in a closed state, to start working when necessary (for example, during stress or increased physical activity).
Capillaries anastomose and, branching, form a complex network, the main links of which are:
- Arterioles - branch into precapillaries;
- Precapillaries are transitional vessels between arterioles and the capillaries themselves;
- True capillaries;
- Postcapillaries;
- Venules are the transition points between capillaries and veins.
Each type of vessel that makes up this network has its own mechanism for transferring nutrients and metabolites between the blood they contain and nearby tissues. The muscles of larger arteries and arterioles are responsible for the movement of blood and its flow into the smallest vessels. In addition, regulation of blood flow is also carried out by the muscular sphincters of the pre- and post-capillaries. The function of these vessels is mainly distributive, while true capillaries perform a trophic (nutritional) function.
Vienna
Veins are another group of vessels, the function of which, unlike arteries, is not to deliver blood to tissues and organs, but to ensure its flow to the heart. To do this, blood moves through the veins in the opposite direction - from tissues and organs to the heart muscle. Due to the difference in functions, the structure of veins is somewhat different from the structure of arteries. The factor of strong pressure that blood exerts on the walls of blood vessels is much less manifested in veins than in arteries, therefore the elastin-collagen framework in the walls of these vessels is weaker, and muscle fibers are represented in smaller quantities. This is why veins that do not receive blood collapse.
Similar to arteries, veins branch widely to form networks. Many microscopic veins merge into single venous trunks, which lead to the largest vessels flowing into the heart.
The movement of blood through the veins is possible due to the action of negative pressure on it in the chest cavity. Blood moves in the direction of the suction force into the heart and chest cavity; in addition, its timely outflow is ensured by the smooth muscle layer in the walls of blood vessels. The movement of blood from the lower extremities upward is difficult, therefore, in the vessels of the lower part of the body, the muscles of the walls are more developed.
In order for blood to move towards the heart, and not in the opposite direction, valves are located in the walls of the venous vessels, represented by a fold of endothelium with a connective tissue layer. The free end of the valve freely directs blood in the direction of the heart, and the outflow is blocked back.
Most veins run adjacent to one or more arteries: small arteries usually have two veins near them, and larger ones usually have one vein near them. Veins, which do not accompany any arteries, are found in the connective tissue under the skin.
The walls of larger vessels are supplied with food by arteries and veins of smaller sizes, extending from the same trunk or from neighboring vascular trunks. The entire complex is located in the connective tissue layer surrounding the vessel. This structure is called the vascular sheath.
The venous and arterial walls are well innervated, contain a variety of receptors and effectors, well connected with the governing nerve centers, due to which the automatic regulation of blood circulation is carried out. Thanks to the work of reflexogenic areas of blood vessels, nervous and humoral regulation of metabolism in tissues is ensured.
Cellular structure of blood
Blood consists of two components: plasma (50-60%) and suspended formed elements (40-50%).
The second category includes:
· Erythrocytes (red blood cells) are the most numerous of the formed elements. According to official studies, one drop of blood contains about 5 million red blood cells. Red blood cells are responsible for transporting gases - oxygen and carbon dioxide. They contain the protein hemoglobin, which binds oxygen molecules in the lungs. Red blood cells deliver oxygen to all tissues and organs, after which they absorb carbon dioxide and carry it to the lungs. It is removed from the body during respiration.
· Leukocytes (white blood cells) - elements that protect our body from foreign bodies and compounds, are part of the immune system. White blood cells recognize and attack pathogens through the production of antibodies and macrophages. When an infection enters the body, the production of leukocytes increases significantly. Normally, their quantity is inferior to the concentration in the blood of other formed elements.
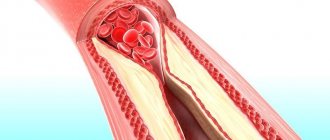
· Platelets (blood platelets) are cells that provide coagulation (clotting) of blood flowing from a damaged vessel and protect the body from heavy blood loss. They stick to the hole in the damaged vessel, forming a “sealing” plug to stop bleeding. It is the platelets that can stick together and form pathological blood clots inside the vessels, called thrombi.
All formed elements are synthesized by the bone marrow and distributed through plasma, the liquid part of the blood.
Functional groups of blood vessels
The entire circulatory system is divided into six different groups of vessels according to functional load. Thus, in human anatomy one can distinguish shock-absorbing, exchange, resistive, capacitive, shunting and sphincteric vessels.
Shock absorbing vessels
This group mainly includes arteries in which the layer of elastin and collagen fibers is well represented. It includes the largest vessels - the aorta and pulmonary artery, as well as areas adjacent to these arteries. The elasticity and resilience of their walls provides the necessary shock-absorbing properties, due to which the systolic waves that occur during heart contractions are smoothed out.
The shock absorption effect in question is also called the Windkessel effect, which in German means “compression chamber effect”.
To clearly demonstrate this effect, the following experiment is used. Two tubes are connected to a container filled with water, one made of elastic material (rubber) and the other made of glass. From a hard glass tube, water splashes out in sharp intermittent bursts, while from a soft rubber tube it flows out evenly and constantly. This effect is explained by the physical properties of the tube materials. The walls of the elastic tube are stretched under the influence of liquid pressure, which leads to the generation of so-called elastic tension energy. Thus, the kinetic energy resulting from pressure is converted into potential energy, which increases voltage.
The kinetic energy of cardiac contraction acts on the walls of the aorta and large vessels that extend from it, causing them to stretch. These vessels form a compression chamber: blood entering them under the pressure of heart systole stretches their walls, kinetic energy is converted into elastic tension energy, which contributes to the uniform movement of blood through the vessels during diastole.
Arteries located further from the heart are of the muscular type, their elastic layer is less pronounced, and they have more muscle fibers. The transition from one type of vessel to another occurs gradually. Further blood flow is ensured by contraction of the smooth muscles of the muscular arteries. At the same time, the smooth muscle layer of large elastic arteries has virtually no effect on the diameter of the vessel, which ensures the stability of hydrodynamic properties.
Resistive vessels
Resistive properties are found in arterioles and terminal arteries. The same properties, but to a lesser extent, are characteristic of venules and capillaries. The resistance of blood vessels depends on their cross-sectional area, and the terminal arteries have a well-developed muscular layer that regulates the lumen of the vessels. Vessels with a small lumen and thick, strong walls provide mechanical resistance to blood flow. The developed smooth muscles of resistive vessels provide regulation of blood volumetric velocity, controls the blood supply to organs and systems due to cardiac output.
Sphincter vessels
Sphincters are located at the end sections of the precapillaries; when they narrow or expand, the number of working capillaries that provide tissue trophism changes. When the sphincter expands, the capillary enters a functioning state; in non-functioning capillaries, the sphincters are narrowed.
Exchange vessels
Capillaries are vessels that perform an exchange function, carrying out diffusion, filtration and trophism of tissues. Capillaries cannot independently regulate their diameter; changes in the lumen of blood vessels occur in response to changes in the sphincters of the precapillaries. The processes of diffusion and filtration occur not only in capillaries, but also in venules, so this group of vessels also belongs to the exchange vessels.
Capacitive vessels
Vessels that act as reservoirs for large volumes of blood. Most often, capacitive vessels include veins - their structural features allow them to hold more than 1000 ml of blood and eject it as needed, ensuring stability of blood circulation, uniform blood flow and complete blood supply to organs and tissues.
Humans, unlike most other warm-blooded animals, do not have special reservoirs for storing blood from which it could be released as needed (in dogs, for example, this function is performed by the spleen). Veins can accumulate blood to regulate the redistribution of its volume throughout the body, which is facilitated by their shape. Flattened veins accommodate large volumes of blood, without stretching, but acquiring an oval lumen shape.
Capacitive vessels include large veins in the abdominal area, veins in the subpapillary plexus of the skin, and veins of the liver. The function of depositing large volumes of blood can also be performed by the pulmonary veins.
Shunt vessels
- Shunt vessels are an anastomosis of arteries and veins; when they are open, blood circulation in the capillaries is significantly reduced. Shunt vessels are divided into several groups according to their function and structural features:
- Pericardial vessels - these include elastic arteries, vena cava, pulmonary arterial trunk and pulmonary vein. They begin and end the systemic and pulmonary circulation.
- Great vessels are large and medium-sized vessels, veins and arteries of the muscular type, located outside the organs. With their help, blood is distributed to all parts of the body.
- Organ vessels - intraorgan arteries, veins, capillaries, providing trophism to the tissues of internal organs.
BLOOD (ARTERIAL) PRESSURE
With each contraction of the left ventricle of the heart, the arteries fill with blood and stretch. This phase of the cardiac cycle is called ventricular systole, and the phase of ventricular relaxation is called diastole. During diastole, however, the elastic forces of large blood vessels come into play, maintaining blood pressure and preventing the flow of blood to various parts of the body from being interrupted. The change of systole (contraction) and diastole (relaxation) gives the blood flow in the arteries a pulsating character. The pulse can be found in any major artery, but is usually felt in the wrist. In adults, the pulse rate is usually 68–88, and in children – 80–100 beats per minute. The existence of arterial pulsation is also evidenced by the fact that when an artery is cut, bright red blood flows out in spurts, and when a vein is cut, bluish (due to lower oxygen content) blood flows evenly, without visible tremors.
To ensure proper blood supply to all parts of the body during both phases of the cardiac cycle, a certain level of blood pressure is needed. Although this value varies widely even in healthy people, normal blood pressure averages 100–150 mmHg. during systole and 60–90 mm Hg. during diastole. The difference between these indicators is called pulse pressure. For example, a person with a blood pressure of 140/90 mmHg. pulse pressure is 50 mm Hg. Another indicator, mean arterial pressure, can be approximated by averaging systolic and diastolic pressure or adding half the pulse pressure to diastolic pressure.
Normal blood pressure is determined, maintained and regulated by many factors, the main ones being the strength of heart contraction, the elastic recoil of the artery walls, the volume of blood in the arteries and the resistance of small arteries (muscular type) and arterioles to the movement of blood. All these factors together determine the lateral pressure on the elastic walls of the arteries. It can be measured very accurately by using a special electronic probe inserted into the artery and recording the results on paper. Such devices, however, are quite expensive and are used only for special studies, and doctors, as a rule, make indirect measurements using the so-called. sphygmomanometer (tonometer).
A sphygmomanometer consists of a cuff that is wrapped around the limb where the measurement is made, and a recording device, which can be a column of mercury or a simple aneroid manometer. Typically, the cuff is wrapped tightly around the arm above the elbow and inflated until there is no pulse at the wrist. The brachial artery is located at the level of the elbow and a stethoscope is placed over it, after which the air is slowly released from the cuff. When the pressure in the cuff drops to a level at which blood flow through the artery resumes, a sound audible with a stethoscope is produced. The readings of the measuring device at the moment of the appearance of this first sound (tone) correspond to the level of systolic blood pressure. With further release of air from the cuff, the nature of the sound changes significantly or it disappears completely. This moment corresponds to the level of diastolic pressure.
In a healthy person, blood pressure fluctuates throughout the day depending on the emotional state, stress, sleep and many other physical and mental factors. These fluctuations reflect certain shifts in the normally existing delicate balance, which is maintained both by nerve impulses coming from the centers of the brain through the sympathetic nervous system, and by changes in the chemical composition of the blood, which have a direct or indirect regulatory effect on the blood vessels. With strong emotional stress, the sympathetic nerves cause a narrowing of small muscular arteries, which leads to an increase in blood pressure and pulse rate. Of even greater importance is the chemical balance, the influence of which is mediated not only by the brain centers, but also by individual nerve plexuses associated with the aorta and carotid arteries. The sensitivity of this chemical regulation is illustrated, for example, by the effect of carbon dioxide accumulation in the blood. As its level increases, the acidity of the blood increases; this both directly and indirectly causes contraction of the walls of peripheral arteries, which is accompanied by an increase in blood pressure. At the same time, the heart rate increases, but the blood vessels of the brain paradoxically expand. The combination of these physiological reactions ensures a stable supply of oxygen to the brain by increasing the volume of incoming blood.
It is the fine regulation of blood pressure that allows you to quickly change the horizontal position of the body to a vertical one without significant movement of blood to the lower extremities, which could cause fainting due to insufficient blood supply to the brain. In such cases, the walls of the peripheral arteries contract and oxygenated blood is directed primarily to vital organs. Vasomotor (vasomotor) mechanisms are even more important for animals such as the giraffe, whose brain, when it raises its head after drinking, moves up almost 4 m in a few seconds. A similar decrease in blood content in the vessels of the skin, digestive tract and liver occurs in moments of stress, emotional distress, shock and trauma, which helps provide more oxygen and nutrients to the brain, heart and muscles.
Such fluctuations in blood pressure are normal, but changes are also observed in a number of pathological conditions. In heart failure, the force of contraction of the heart muscle may decrease so much that blood pressure becomes too low (hypotension). Likewise, loss of blood or other fluids due to a severe burn or bleeding can cause both systolic and diastolic blood pressure to drop to dangerous levels. With some congenital heart defects (for example, patent ductus arteriosus) and a number of lesions of the valvular apparatus of the heart (for example, aortic valve insufficiency), peripheral resistance drops sharply. In such cases, systolic pressure may remain normal, but diastolic pressure decreases significantly, which means an increase in pulse pressure.
Some diseases are accompanied not by a decrease, but, on the contrary, by an increase in blood pressure (arterial hypertension). Older people whose blood vessels lose elasticity and become stiffer usually develop a benign form of arterial hypertension. In these cases, due to a decrease in vascular distensibility, systolic blood pressure reaches a high level, while diastolic blood pressure remains almost normal. In some diseases of the kidneys and adrenal glands, very large amounts of hormones such as catecholamines and renin enter the blood. These substances cause constriction of blood vessels and, therefore, hypertension. With both this and other forms of increased blood pressure, the causes of which are less understood, the activity of the sympathetic nervous system also increases, which further enhances the contraction of the vascular walls. Long-term arterial hypertension, if left untreated, leads to accelerated development of atherosclerosis, as well as an increased incidence of renal diseases, heart failure and strokes. See also ARTERIAL HYPERTENSION.
Regulating blood pressure in the body and maintaining the necessary blood supply to organs best allows us to understand the colossal complexity of the organization and operation of the circulatory system. This truly remarkable transport system is a real “lifeline” of the body, since insufficient blood supply to any vital organ, primarily the brain, for at least a few minutes leads to irreversible damage and even death.
Blood vessel diseases
- The most dangerous vascular diseases that pose a threat to life: aneurysm of the abdominal and thoracic aorta, arterial hypertension, coronary artery disease, stroke, renal vascular diseases, atherosclerosis of the carotid arteries.
- Vascular diseases of the legs are a group of diseases that lead to impaired blood circulation in the vessels, pathologies of the vein valves, and blood clotting disorders.
- Atherosclerosis of the lower extremities - a pathological process affects large and medium-sized vessels (aorta, iliac, popliteal, femoral arteries), causing them to narrow. As a result, the blood supply to the extremities is disrupted, severe pain appears, and the patient’s performance is impaired.
- Varicose veins are a disease that results in dilation and lengthening of the veins of the upper and lower extremities, thinning of their walls, and the formation of varicose nodes. The changes that occur in the vessels are usually persistent and irreversible. Varicose veins are more common in women - in 30% of women after 40 and only 10% of men of the same age. (