What's happening?
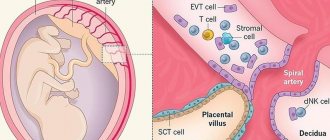
During the formation of the placenta, chorionic villi “invade” the uterine mucosa (endometrium). This is the same membrane that is shed during menstrual bleeding. However, there are cases when villi grow into the muscle layer, and sometimes throughout the entire thickness of the uterine wall. A dense attachment or accretion of the placenta occurs, differing in the depth of growth of the chorionic villi into the wall of the uterus.
Unfortunately, it is possible to recognize placenta accreta and tight attachment (and distinguish them from each other) only during childbirth, during the operation of manual separation of the placenta. If the placenta is tightly attached and accreted in the afterbirth period (III stage of labor), the placenta does not separate spontaneously.
Dense attachment or placenta accreta can be complete if the placenta is attached to its bed over the entire area, and partial if the placenta is attached only in one area. In the first case, spontaneous bleeding does not occur. In the second, when placental abruption begins, bleeding occurs, which can be very heavy.
Risk factors [edit]
An important risk factor for placenta accreta is placenta previa in the presence of a scar on the uterus. Placenta previa is an independent risk factor for placenta accreta. Additional reported risk factors for placenta accreta include maternal age and multiparity, other pre-uterine surgery, pre-uterine curettage radiation, endometrial ablation, Asherman's syndrome, uterine leiomyomas, uterine anomalies, hypertensive disorders of pregnancy[ edit
], and smoking.
The condition is increased in incidence by the presence of scar tissue, i.e. Asherman's syndrome is usually from past uterine surgery, especially from past dilation and curettage, [3] (which is used for many symptoms including miscarriage, cessation, and postpartum hemorrhage), myomectomy, [4] or cesarean section. A thin decidua may also be a contributing factor to such trophoblastic invasion. Some studies suggest that the incidence is higher in female fetuses. [5] Other risk factors include low-lying placenta, anterior placenta, congenital or acquired uterine defects (eg, uterine septum), leiomyoma, ectopic placental implantation (including horny pregnancy). [6] [7] [8]
Pregnant women over 35 years of age who have had a cesarean section and currently have placenta previa over a uterine scar have a 40% chance of placenta accreta. [9]
Manual separation of the placenta
Indications for surgery:
- no signs of placental separation without bleeding 30 minutes after the birth of the baby;
- no signs of placental separation when bleeding begins, as soon as blood loss reaches 250 ml
The operation is performed under intravenous anesthesia. Simultaneously with the start of the operation, drip administration of glucose, crystalloid solutions, and uterine contractions is started. When firmly attached, the placenta is easily separated from the uterine wall.
After manual examination of the walls of the uterine cavity and confidence that it has completely emptied, oxytocin is injected intravenously, an ice pack is placed on the lower abdomen, and the condition of the uterus is periodically monitored by palpation through the anterior abdominal wall. In order to prevent postpartum infection, antibiotics are prescribed in all cases of surgical intervention in the afterbirth period. In case of pathological blood loss (500 ml or more), blood loss is compensated.
In case of accreta, the placenta (or part of it) cannot be separated from the uterus. In this situation, doctors are obliged to stop all attempts to separate the placenta and perform an urgent removal of the uterus.
Bleeding in the third stage of labor associated with abnormal placental attachment should be differentiated from bleeding caused by retention or strangulation of the separated placenta .
Since December 2021, specialists from the Republican Scientific and Practical Center "Cardiology" and the Republican Scientific and Practical Center "Mother and Child" have performed 11 hybrid operations for the delivery of patients with placenta accreta. This is a serious complication of pregnancy and carries the risk of extensive uterine bleeding, since the placental vessels extend beyond the uterus and can even enter nearby organs. Moreover, the number of patients with this pathology is growing every year both in Belarus and throughout the world.
Etiology of the unknown
Placenta accreta develops in women who delivered by caesarean section in a previous pregnancy. It is known that the percentage of these interventions in the world is increasing every year. Our country is no exception. Accordingly, the numbers of detected placenta accreta are growing. In particular, if in 2013 the Republican Scientific and Practical Center “Mother and Child” provided assistance to 2 such patients, then in 2017 – 23, and in 2020 – already 36.
The mechanism of development of this pathology is still unclear. In one patient, placenta accreta may appear after the first cesarean section, while in another it will not occur even after several surgical deliveries. This uncertainty currently does not allow specialists to form risk groups.
“The peculiarity of our healthcare system is that almost all patients are registered during pregnancy at the antenatal clinic and undergo ultrasound at least three times in prenatal centers. Specialists from these institutions immediately pay attention to the location of the placenta in patients with a uterine scar. So the probability of detecting an ingrowth is very high,” explained Elena Goshkevich, Deputy Director for Obstetrics and Gynecology of the Republican Scientific and Practical Center “Mother and Child”. — You need to understand that pathology may not develop immediately. For some, it is detected only at 36–37 weeks. Massive ingrowth can form up to 22 weeks of pregnancy. But in most cases, pathology is detected after the second screening.
According to the expert, placenta accreta that is not detected in time is associated with a high risk of maternal mortality, since patients develop completely uncontrollable bleeding.
“In this case, the vessels are pathological, they grow from the placenta chaotically in very large numbers, and it is impossible to predict their course. In addition, the blood supply to the pregnant uterus, even normally, changes significantly, for example, the diameter of the vessels increases, noted Elena Goshkevich. — If you operate on such patients without modern technologies, without a hybrid operating room, then blood loss reaches 5–8 liters. That is, almost equal to the volume of circulating blood. And in many cases it becomes simply unrealistic to save patients. After all, it is very difficult to transfuse such a large volume of blood quickly.
For several years, specialists from the Republican Scientific and Practical Center “Mother and Child” worked on a project to develop instructions for providing medical care to patients with signs of placenta accreta. It is important to create a unified algorithm with proven logistics: operations must be carried out in a specific institution with the participation of a specific surgical team.
All patients with this pathology are dead today. After a consultation appointment, they are hospitalized in a hospital, usually for a period of 30–32 weeks. Additionally, the center performs an MRI to determine the extent of placenta accreta. In particular, the presence of signs of placenta accreta into the parametrium, posterior wall and cervix is of fundamental importance for the provision of medical care. In these cases, the ureters are stented in advance to reduce the risk of intraoperative trauma.
— The vast majority of women give birth at 34–35 weeks. Delivery at a later stage increases the risk of intraoperative complications, so such cases are rare and are associated exclusively with late diagnosis of pathology. It is extremely rare that we give birth to patients before 30 weeks of gestation. These are, as a rule, those for whom the pathology is diagnosed before 20 weeks of pregnancy and is characterized by the extensiveness of the pathological process. By 34 weeks the situation can become almost uncontrollable,” said Elena Goshkevich.
Same operating room, different specialists
In addition to the Republican Scientific and Practical Center “Mother and Child,” 2 more large medical institutions of the republic are involved in providing surgical care to patients with placenta accreta. For a long time, the center has been collaborating with the Minsk Scientific and Practical Center for Surgery, Transplantation and Hematology, on the basis of which embolization of the uterine arteries is currently performed. And since December 2021, they also began to interact with the Republican Scientific and Practical Center “Cardiology”, where balloon occlusion of the descending aorta is performed in the conditions of the X-ray operating room.
— The main task is to partially or completely block the uterine blood flow. Previously, two methods were used for this in patients with placenta accreta: balloon occlusion of the iliac arteries and embolization of the uterine arteries. However, at the level of our center, a proposal was made for a more radical solution to this problem. Not all arteries supplying the uterus arise from the iliac arteries. For example, the ovarian artery arises from the aorta. Plus, when the uterine blood flow is partially blocked, venous return occurs,” said Oleg Polonetsky, head of X-ray operating room No. 2 of the Republican Scientific and Practical Center “Cardiology”.
— We proposed to carry out occlusion of the aorta at the level of the distal segment of the renal arteries. From the point of view of X-ray endovascular surgery, this technique has its own risks, which we discussed with colleagues from the Republican Scientific and Practical Center “Mother and Child”. First of all, this is thrombus formation in the blocked aorta. But by outlining approaches to prevention, including placing the balloon as high as possible in the renal arteries and using low doses of heparin, we took a chance and received good feedback from obstetricians and gynecologists.
By the way, the tools for carrying out such operations have long been in the arsenal of specialists at the Republican Scientific and Practical Center “Cardiology”. Aortic stenting has been performed here for many years. To improve the opposition of stents to the vessel wall, they come with balloons corresponding to the diameter of the aorta. But they are not always used in cardiac patients. But their use has shown effectiveness in patients with placenta accreta.
The operation lasts 4 hours or more. First, a puncture of the femoral artery is performed under spinal anesthesia. The patient then undergoes a caesarean section under general anesthesia. And after removing the child, surgeons perform an inspection of the uterus. When ready, endovascular surgeons inflate the balloon and stop the blood flow. Moreover, occlusion should not exceed 20 minutes. As practice has shown, Oleg Polonetsky clarified, this time is enough for the main stage of the operation.
A collaborative approach to the delivery of patients with placenta accreta can significantly reduce blood loss. And its volume, according to the protocol for providing obstetric care, is of great importance in deciding whether to remove the uterus. In almost all cases of delivery using angiographic techniques, blood loss does not exceed 1,500 ml.
“The question of the possibility of performing organ-preserving surgery is decided by an intraoperative council of obstetricians and gynecologists,” noted Elena Goshkevich. — You need to understand that we work with young patients. And even if they do not intend to give birth to children in the future, preserving the uterus is psychologically important for them. Thus, since the beginning of 2021, together with specialists from the Republican Scientific and Practical Center “Cardiology,” we have operated on 8 patients, six of whom underwent organ-preserving interventions (metroplasty).
Elena Goshkevich also emphasized that such operations are very labor-intensive and require the participation of many specialists. An obstetric team, a pediatric resuscitation team, an x-ray endovascular surgeon, nursing staff and, as a rule, 2 anesthesiologists and resuscitators are involved. In addition, in cases of pathological changes in the urinary system, urologists are involved.
The use of a multidisciplinary approach requires the existence of treatment protocols for this group of patients, which would reflect all stages of care and the areas of responsibility of each member of this team, in order to obtain the maximum effect from treatment, says Sergei Spiridonov, Deputy Director for Surgical Care of the Republican Scientific and Practical Center "Cardiology".
Geographic Help Center
After the operation, the patient remains in the intensive care unit of the Republican Scientific and Practical Center "Cardiology" for 24 hours. The child is immediately taken to the children's intensive care unit of the Republican Scientific and Practical Center "Mother and Child", since he is definitely born premature. However, some are transferred almost immediately to the pediatric department.
Currently, an algorithm for outpatient monitoring of patients after surgical delivery for placenta accreta has been developed and used, since in this group of patients there are risks of long-term complications from the urinary system.
Recently, the Ministry of Health approved instructions for diagnosing placenta accreta and providing assistance to such patients. These instructions were developed by 3 medical institutions: Republican Scientific Center “Mother and Child”, Republican Scientific and Practical Center “Cardiology” and Minsk Scientific and Practical Center for Surgery, Transplantation and Hematology.
— In the future, we plan to prepare a clinical protocol based on them. I would like it to be introduced in the regions so that local specialists could provide assistance to patients with placenta accreta in cases, for example, when transportation to our center is impossible. But we still understand that this requires a skill that is developed in practice. Therefore, the bulk of medical care should be concentrated in Minsk. And especially when it comes to obstetrics, when you have two lives in your hands at once,” concluded Elena Goshkevich.
Sources
- Petersen DS., Kreuter N., Heepe L., Büsse S., Wellbrock AHJ., Witte K., Gorb SN. Holding tight to feathers — structural specializations and attachment properties of the avian ectoparasite Crataerina pallida (Diptera, Hippoboscidae). // J Exp Biol - 2021 - Vol221 - NPt 13 - p.; PMID:29712747
- Mori H., Kobara H., Nishiyama N., Masaki T. Novel concept of endoscopic device delivery station system for rapid and tight attachment of polyglycolic acid sheet. // World J Gastroenterol - 2018 - Vol24 - N2 - p.211-215; PMID:29375206
- Voigt D., Tsipenyuk A., Varenberg M. How tight are beetle hugs? Attachment in matting leaf beetles. // R Soc Open Sci - 2021 - Vol4 - N9 - p.171108; PMID:28989792
- Adams GC., Stoops MA., Skomro RP. Sleep tight: exploring the relationship between sleep and attachment style across the life span. // Sleep Med Rev - 2014 - Vol18 - N6 - p.495-507; PMID:24721278
- Fau M., Kowalczyk A., Olejnik P., Nowicka AM. Tight and uniform layer of covalently bound aminoethylophenyl groups perpendicular to gold surface for attachment of biomolecules. // Anal Chem - 2011 - Vol83 - N24 - p.9281-8; PMID:22047188
Diagnosis[edit]
When a prenatal diagnosis of placenta accreta is made, it is usually based on ultrasound findings in the second or third trimester. Sonographic findings that may indicate placenta accreta include:
- Loss of the normal hypoechoic retroplacental zone
- Multiple vascular lacunae (irregular vascular spaces) within the placenta, giving a “Swiss cheese” appearance
- Blood vessels or placental tissue connecting the edge of the uterus and placenta, the interface between the myometrium and bladder, or crossing the serosa of the uterus
- Retroplacental myometrial thickness <1 mm
- Numerous connected vessels visualized using 3D power Doppler in basal projection
Unfortunately, diagnosis is not easy to make and is affected by significant interobserver variability. [11] In doubtful cases, nuclear magnetic resonance (MRI) of the pelvis can be performed, which has very good sensitivity and specificity for this disease. [12] MRI findings associated with placenta accreta include T2 dark streaks, uterine protrusion, and loss of the T2 dark interface. [13]
Although there are anecdotal reports of placenta accreta being diagnosed in the first trimester or at the time of abortion <20 weeks of gestation, the predictive value of first trimester ultrasound for this diagnosis remains unknown. Women with placenta previa, or a “low-lying placenta” covering a scar on the uterus in early pregnancy, should undergo a follow-up examination in the third trimester, paying attention to the possible presence of placenta accreta.
Epidemiology[edit]
The reported incidence of placenta accreta has increased from approximately 0.8 per 1000 births in the 1980s to 3 per 1000 births in the last decade.
The incidence increased with the number of cesarean sections: 1 in 4027 pregnancies in the 1970s, 1 in 2510 in the 1980s, and 1 in 533 in 1982–2002. [20] In 2002, ACOG estimated that the incidence had increased 10-fold over the past 50 years. [8] The risk of placenta accreta in future births after cesarean section is 0.4-0.8%. For patients with placenta previa, the risk increases with the number of previous cesarean sections, at rates of 3%, 11%, 40%, 61%, and 67% for the first, second, third, fourth, and fifth or more number of cesarean sections. sections. [21]
Links[edit]
- Smith, Zachary L.; Sehgal, Shailen S.; Aarsdalen, Keith N. Wang; Goldstein, Irwin S. (2014). "Placenta Percreta with penetration into the bladder". Urology Case Reports
.
2
(1): 31–32. DOI: 10.1016/j.eucr.2013.11.010. PMC 4733000. PMID 26955539. - Society of Gynecologic Oncology; American College of Obstetricians and Gynecologists and Society of Maternal-Fetal Medicine; Cahill, Alison J.; Beigi, Richard; Heine, R. Phillips; Silver, Robert M.; Wachs, Joseph R. (2018-12-01). "Spectrum of placenta accreta". American Journal of Obstetrics and Gynecology
.
219
(6):B2–B16. DOI: 10.1016/j.ajog.2018.09.042. ISSN 1097-6868. PMID 30471891. - Capella-Allouc, S.; Morsad, F; Rongières-Bertrand, C; Taylor, S; Fernandez, H (1999). "Hysteroscopic treatment of severe Asherman's syndrome and subsequent fertility". Human reproduction
.
14
(5):1230–3. DOI: 10.1093/humrep/14.5.1230. PMID 10325268. - Al-Serehi, A; Mkhoyan, A; Brown, M; Benirschke, K; Housing, A; Pretorius, D.H. (2008). "Placenta accreta: association with fibroids and Asherman's syndrome." Journal of Ultrasound in Medicine
.
27
(11): 1623–8. DOI: 10.7863/jum.2008.27.11.1623. PMID 18946102. S2CID 833810. - American Pregnancy Association (January 2004) "Placenta accreta Archived 2006-01-16 at the Wayback Machine." Accessed October 16, 2006
- Arulkumaran, edited by Richard Warren, Sabaratnam (2009). Best Practices in Labor and Delivery
(1st ed., 3rd ed.). Cambridge: Cambridge University Press. pp. 108, 146. ISBN 978-0-521-72068-7.CS1 maint: additional text: list of authors (link) - Szymonowicz, S; Gurvits, A; Dushnik, M; Antebi, E; Geva-Eldar, T; Yagel, S (September 1994). "Developmental regulation of 72 and 92 kDa type IV collagenase expression in human trophoblasts: a possible mechanism for the control of trophoblast invasion." American Journal of Obstetrics and Gynecology
.
171
(3):832–8. DOI: 10.1016/0002-9378 (94) 90107-4. PMID 7522400. - ^ ab ACOG Committee on Obstetrics, Practice (January 2002). “ACOG Committee Opinion. Number 266, January 2002: placenta accreta." Obstetrics and gynecology
.
99
(1):169–70. DOI: 10.1016/s0029-7844(01)01748-3. PMID 11777527. - Hobbins, John S. (2007). Obstetric Ultrasound: Artistry in Practice
. Oxford: Blackwell. clause 10. ISBN 978-1-4051-5815-2. - ^ ab Stephen G. Gabby; Jennifer R. Nibil; Joe Lee Simpson, ed. (2002). Obstetrics: normal and problematic pregnancy
(4th ed.). New York, NY [ua]: Churchill Livingston. item 519. ISBN 9780443065729. - Bowman ZS, Eller AG, Kennedy AM, Richards DS, Winter TC, Woodward PJ, Silver RM (December 2014). "Ultrasound variability for predicting placenta accreta". Journal of Ultrasound in Medicine
.
33
(12):2153–8. DOI: 10.7863/ultra.33.12.2153. PMID 25425372. S2CID 22246937. - D - Antonio J, Iacovella S, Palacios-Jaraquemada J, Bruno CH, Manzoli L, Bhide A (July 2014). "Prenatal identification of invasive placentation using magnetic resonance imaging: a systematic review and meta-analysis." Ultrasound in obstetrics and gynecology
.
44
(1): 8–16. DOI: 10.1002/uog.13327. PMID 24515654. S2CID 9237117. - Balcacer, Patricia; Pahade, Jay; Spector, Michael; Staib, Lawrence; Copel, Joshua A.; McCarthy, Shirley (2016). "Magnetic resonance imaging and sonography in the diagnosis of placental invasion". Journal of Ultrasound in Medicine
.
35
(7):1445–1456. DOI: 10.7863/ultra.15.07040. ISSN 0278-4297. PMID 27229131. - Selman AE (April 2016). "Cesarean section hysterectomy for placenta previa/accreta using the pouch of Douglas approach". BJOG: International Journal of Obstetrics and Gynecology
.
123
(5):815–9. DOI: 10.1111/1471-0528.13762. PMC 5064651. PMID 26642997. - Washecka R, Behling A (April 2002). "Urologic complications of placenta percreta with bladder invasion: a case report and review of the literature." Hawaiian Medical Journal
.
61
(4): 66–9. PMID 12050959. - Johnston, T.A.; Paterson-Brown, S (January 2011). Placenta previa, placenta accreta and placenta previa: diagnosis and treatment. Green-top Recommendation No. 27. Royal College of Obstetricians and Gynecologists.
- ^ ab Oyelese, Yinka; Smulian, John S. (2006). "Excellent placenta, placenta accreta and vase previa." Obstetrics and gynecology
.
107
(4):927–41. DOI: 10.1097/01.AOG.0000207559.15715.98. PMID 16582134. S2CID 22774083. - ^ ab Turrentine, John E. (2008). Clinical protocols in obstetrics and gynecology
(3rd ed.). London: Informa Healthcare. item 286. ISBN. 9780415439961. - Committee on Obstetrics, Practice (2002). "Placenta Acreta No. 266, January 2002 Committee on Obstetric Practice." International Journal of Gynecology and Obstetrics
.
77
(1):77–8. DOI: 10.1016/S0020-7292(02)80003-0. PMID 12053897. S2CID 42076480. - Committee on Obstetric Practice. "Placenta accreta". American College of Obstetricians and Gynecologists
. Archived from the original on 2016-11-23. Retrieved August 22, 2014. - Silver, RM; Landon, M.B.; Rose, DJ; Leveno, K.J.; Sponge, C.Y.; Tom, E.A.; Moawad, A.H.; Karitis, S.N.; Harper, M; Wapner, R.J.; Sorokin, Yu; Miodovnik, M; Carpenter, M; Peacemaker AM; O'Sullivan, MJ; Sibay, B; Langer, O; Thorpe, J.M.; Ramin, S.M.; Mercer, B.M.; National Institute of Children's Health Maternal-Fetal Medicine Network; and others. (2006). "Maternal morbidity associated with multiple repeat cesarean births." Obstet Gynecol
.
107
(6):1226–32. DOI: 10.1097/01.AOG.0000219750.79480.84. PMID 16738145. S2CID 257455.