A comprehensive study of the quantitative and qualitative composition of formed elements and biochemical blood parameters, which allows you to assess the saturation of the body with iron and detect the deficiency of this microelement even before the first clinical signs of iron deficiency appear.
The research results are provided with a free doctor’s commentary.
Synonyms Russian
Sideropenia, hypoferremia.
English synonyms
Iron deficiency test.
Research method
Colorimetric photometric method, SLS (sodium lauryl sulfate) method, conductometric method, flow cytometry, immunoturbidimetry.
Units
µmol/l (micromoles per liter), *10^9/l, *10^12/l, g/l (grams per liter), % (percentage), fl (femtoliter), pg (picograms).
What biomaterial can be used for research?
Venous blood.
How to properly prepare for research?
- Eliminate alcohol from your diet 24 hours before the test.
- Stop eating 8 hours before the test, you can drink clean still water.
- Do not take medications for 24 hours before the test (as agreed with your doctor).
- Avoid taking medications containing iron for 72 hours before the test.
- Avoid physical and emotional stress and do not smoke for 30 minutes before the test.
General information about the study
Iron deficiency is quite common. About 80-90% of all forms of anemia are associated with a deficiency of this microelement.
Iron is found in all cells of the body and performs several important functions. Its main part is part of hemoglobin and ensures the transport of oxygen and carbon dioxide. Some iron is a cofactor for intracellular enzymes and is involved in many biochemical reactions.
Iron is constantly removed from the body of a healthy person through sweat, urine, exfoliated cells, as well as menstrual flow in women. To maintain the amount of microelement at a physiological level, a daily intake of 1-2 mg of iron is necessary.
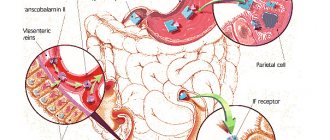
Absorption of this microelement occurs in the duodenum and upper parts of the small intestine. Free iron ions are toxic to cells, so in the human body they are transported and deposited in combination with proteins. In the blood, iron is transported by the protein transferrin to sites of use or accumulation. Apoferritin binds iron and forms ferritin, which is the main form of stored iron in the body. Its amount in the blood is related to iron reserves in tissues.
Iron deficiency develops gradually. Initially, a negative iron balance occurs, in which the body’s need for iron and the loss of this microelement exceed the amount it receives from food. This may be due to blood loss, pregnancy, growth spurts during puberty, or not eating enough foods containing iron. First of all, iron is mobilized from the reserves of the reticuloendothelial system to compensate for the body's needs. Laboratory tests during this period reveal a decrease in the amount of serum ferritin without changes in other indicators. Initially, there are no clinical symptoms, the level of iron in the blood, and clinical blood test parameters are within the reference values.
At the stage of iron deficiency erythropoiesis, hemoglobin synthesis becomes insufficient and iron deficiency anemia develops with clinical manifestations of anemia. In a clinical blood test, small pale-colored red blood cells are detected, MHC (average amount of hemoglobin in an erythrocyte), MCV (average erythrocyte volume), MCHC (average hemoglobin concentration in an erythrocyte), and hemoglobin level and hematocrit decrease. Without treatment, the amount of hemoglobin in the blood progressively decreases, the shape of red blood cells changes, and the intensity of cell division in the bone marrow decreases. The deeper the iron deficiency, the brighter the clinical symptoms become. Fatigue turns into severe weakness and lethargy, the ability to work is lost, the pallor of the skin becomes more pronounced, the structure of the nails changes, cracks appear in the corners of the lips, atrophy of the mucous membranes occurs, the skin becomes dry and flaky. With iron deficiency, the patient's ability to taste and smell changes - there is a desire to eat chalk, clay, raw cereals and inhale the smells of acetone, gasoline, turpentine.
With timely and correct diagnosis of iron deficiency and the causes that caused it, treatment with iron preparations allows you to replenish the reserves of this element in the body.
What is the research used for?
- For early diagnosis of iron deficiency.
- For differential diagnosis of anemia.
- To monitor treatment with iron supplements.
- For examination of persons who have a high probability of iron deficiency.
When is the study scheduled?
- When examining children during periods of intensive growth.
- When examining pregnant women.
- For symptoms of iron deficiency in the body (pallor of the skin, general weakness, fatigue, atrophy of the tongue mucosa, changes in the structure of the nails, abnormal taste preferences).
- When hypochromic microcytic anemia is detected according to a clinical blood test.
- When examining girls and women with heavy menstrual flow and uterine bleeding.
- When examining rheumatological and oncological patients.
- When monitoring the effectiveness of the use of drugs containing iron.
- When examining patients with asthenia of unknown origin and severe fatigue.
What do the results mean?
Reference values
- [02-014] Complete blood count (without leukocyte formula and ESR)
- [06-017] Serum iron
- [06-040] Transferrin
- [06-042] Ferritin
Initial manifestations of iron deficiency (negative iron balance, hidden deficiency):
- decreased serum ferritin levels;
- clinical blood test without signs of anemia.
Iron deficiency without anemia:
- decreased serum ferritin levels;
- clinical blood test without pathology.
Iron-deficiency anemia:
- decreased serum ferritin levels;
- in a clinical blood test there are signs of hypochromic microcytic anemia (decrease in MHC, MCV, MSHC, hemoglobin level and hematocrit).
Causes of low iron levels
- Chronic blood loss: gastrointestinal bleeding due to gastric and duodenal ulcers, hemorrhoids, polyposis, diverticulosis, ulcerative colitis or Crohn's disease;
- uterine bleeding due to uterine fibroids, cervical cancer, endometriosis, ovarian dysfunction, heavy menstrual flow;
- pulmonary bleeding in bronchiectasis, cancer, tuberculosis, pulmonary hemosiderosis;
- hematuria in polycystic kidney disease, kidney cancer, polyps and tumors of the bladder;
- nosebleeds in Rendu-Osler disease;
- helminthiasis (hookworm).
- pregnancy and lactation;
- malabsorption (after subtotal and total resection of the stomach, resection of large sections of the small intestine, chronic enteritis);
- low iron diet, vegetarianism.
Other reasons for changes in iron metabolism with normal or elevated ferritin levels (conditions associated with iron redistribution and/or its relative deficiency, which must be differentiated from an iron deficiency state):
- chronic inflammatory diseases (rheumatic diseases, tuberculosis, brucellosis);
- anemia of other etiologies (hemolytic, megaloblastic, sideroblastic, thalassemia);
- myelodysplastic syndrome;
- acute myeloblastic or lymphoblastic leukemia;
- lead poisoning;
- hemochromatosis or hemosiderosis;
- acute and chronic liver diseases;
- neoplasms (breast cancer, kidney cancer, malignant lymphoma, Hodgkin's disease);
- hyperthyroidism;
- severe renal failure.
What can influence the result?
Factors distorting the result:
- transfusion of blood and its components;
- use of radiopaque intravenous drugs shortly before the study;
- alcoholic liver disease, acute and chronic inflammatory diseases, neoplasms;
- hemodialysis;
- taking medications containing iron;
- use of oral contraceptives and antithyroid therapy.
Causes of anemia
There are quite a few factors that provoke anemia. Anemia can occur due to:
- unbalanced diet (iron deficiency, deficiency or excess of vitamin B12, vegetarianism);
- disorders of folic acid metabolism;
- increased need of the body for nutrients (growth period - adolescence, pregnancy);
- frequent infectious diseases (cytomegalovirus, herpes virus, hepatitis);
- heavy metal poisoning.
In addition, anemia often accompanies diseases of the gastrointestinal tract (chronic gastritis), develops against the background of helminthic infestations, especially often in children (parasites attach to the intestinal wall and can cause bleeding), uterine bleeding (heavy menstruation, endometriosis).
How to recognize anemia?
Typical symptoms of anemia caused by hypoxia of organs and tissues are dizziness, fatigue, weakness, tinnitus, shortness of breath when climbing stairs, decreased performance. There is also a decrease in appetite, pale skin (in some cases yellowing), and “stubs” in the corners of the mouth. Hair may begin to fall out and the condition of nails may deteriorate. In addition, the mood changes and apathy and irritability appear, even if everything is fine.
If you notice such changes, do not rush to take iron or vitamin supplements or take B12 injections. The doctor gives a conclusion about anemia based on laboratory parameters. And taking medications on your own can be unsafe.
Diagnosis of iron deficiency
Currently, several laboratory tests have been developed to diagnose iron deficiency. The main ones include determining the following blood parameters:
- the amount of serum iron;
- indicator of total iron-binding capacity of serum (TIBC);
- transferrin iron saturation percentage;
- ferritin amount;
- amount of hemoglobin.
It is important to understand that it is a big mistake to prescribe iron supplements solely based on the results of determining low ferritin. In the presence of a MTHFR mutation that disrupts the processing and absorption of iron, folic acid, and vitamin B12, ferritin is always low and serum iron is high, which does not allow prescribing iron supplements to such patients.
The goals of laboratory tests for iron deficiency anemia are:
- identification of disturbances in iron metabolism;
- determination of the nature of anemia;
- assessing the risk of developing iron overload in the body.
Preparation for laboratory tests for anemia is simple and fairly standard. It is necessary to donate blood in the morning, strictly on an empty stomach (with an 8-hour break after eating). The day before testing, you must stop taking iron supplements and/or multivitamins. If radioisotope diagnostics were carried out the day before, the study of iron metabolism should begin no earlier than 4-5 days after its completion. It is also important to consider that some medications may interfere with test results. For example, estrogen or oral contraceptives can increase TBI, while corticosteroids and testosterone, on the contrary, lower TBI.