Folate deficiency anemia
Iron deficiency
26967 October 28
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Folate deficiency anemia: causes, symptoms, diagnosis and treatment methods.
Definition
Anemia caused by folic acid deficiency, also called vitamin B9, is a blood disease characterized by a decrease in the amount of hemoglobin and red blood cells (red blood cells).
Folic acid is a natural vitamin that is necessary for normal hematopoiesis.
Under normal conditions, it is synthesized by the intestinal microflora and enters the body as part of folate with food of plant origin (legumes, wholemeal flour, asparagus, spinach, lettuce, broccoli, beef liver).
In the body, folic acid is present in the form of its coenzyme form - tetrahydrofolic acid, which is actively involved in the synthesis of glutamic acid, pyrimidine and purine bases, as well as thymidine monophosphate - a component of DNA. With folate deficiency anemia, first of all, the synthesis of nucleic acids of actively dividing hematopoietic cells is disrupted, resulting in the development of anemia, often combined with leukopenia and thrombocytopenia.
Causes of folate deficiency anemia
The development of folate deficiency anemia is based on many different causes and risk factors. The supply of folic acid in the body is insignificant, so it must be constantly replenished.
One of the main reasons for the development of vitamin B9 deficiency is its insufficient dietary intake.
Often the problem of lack of folic acid in the body is observed in people who abuse alcohol and psychotropic substances. People who consume little vegetables and fruits, especially older people, are also at risk of developing vitamin B9 deficiency.
Folic acid is involved in the process of cell division and is required in large quantities for their growth and rapid renewal.
In this regard, a common cause of folate deficiency anemia is an excessive need for folic acid with low dietary intake. The risk group includes women during pregnancy and lactation, children during periods of intensive growth, and adolescents. People suffering from chronic skin diseases, such as psoriasis and eczema, also need a large amount of folic acid.
Hemolytic anemia (in which, for various reasons, increased destruction of red blood cells occurs) of various origins also contributes to the development of folic acid deficiency.
Malabsorption of folic acid occurs in various intestinal diseases, which are characterized by malabsorption syndrome (decreased function of nutrient absorption in the intestine).
These include inflammatory bowel diseases (for example, Crohn's disease), celiac disease (celiac disease), food allergies in children with intestinal manifestations, lactase deficiency.
In children, the following risk factors play a significant role in the development of folate deficiency anemia: prematurity, low birth weight (less than 2500 g), feeding with whole goat milk, use of unadapted milk formulas, frequent infectious and inflammatory diseases, including the gastrointestinal tract. Various enteritis (inflammation of the small intestine) pose a particular danger of developing anemia in young children.
Medicines and toxic substances can disrupt the absorption and metabolism of folic acid in the body.
Some drugs (for example, methotrexate, used to treat cancer, psoriasis, rheumatoid arthritis, etc.) are folic acid antagonists. Anticonvulsant medications can also lead to folic acid deficiency in the body.
Rare causes of the development of folate deficiency anemia include hereditary defects in folic acid metabolism associated with insufficiency of enzyme systems.
Classification of folate deficiency anemia
There is no generally accepted classification of folate deficiency anemia. However, any anemia is divided into degrees of severity depending on the level of decrease in blood hemoglobin. For children over 6 years of age and adults the following classification applies:
- mild anemia: hemoglobin level from 90 to 120 g/l;
- moderate anemia: hemoglobin level from 70 to 89 g/l;
- severe anemia: hemoglobin level below 70 g/l.
For children under 6 years of age, the normal hemoglobin level is above 110 g/l.
According to ICD-10
The following types of folate deficiency anemia are distinguished:
- Diet-related folate deficiency anemia.
- Folate deficiency anemia is drug-induced.
- Other folate deficiency anemias.
- Folate deficiency anemia, unspecified.
Symptoms of folate deficiency anemia
With folate deficiency anemia, pallor of the skin and mucous membranes with a slight icteric tint, general weakness and decreased performance are noted. Characterized by rapid fatigue and irritability. Due to a decrease in oxygen delivery to tissues, shortness of breath occurs, heart rate increases, and blood pressure may decrease. Patients complain of poor appetite, ringing in the ears and flashing “spots” before the eyes. In severe cases, fainting is possible.
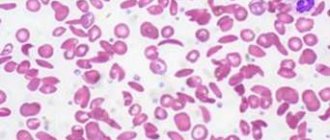
When examining blood, a decrease in the amount of hemoglobin and red blood cells is noted, the color indices of the blood increase (showing an increase in the saturation of red blood cells with hemoglobin), as well as the size of red blood cells. An increase in the content of indirect bilirubin in the blood serum is associated with the destruction of “wrong” red blood cells that are too large. Often, folate deficiency anemia is combined with B12 deficiency anemia, in which various neurological disorders develop, and also accompanies iron deficiency anemia.
For infants and young children, additional symptoms of the development of folate deficiency anemia are lethargy or increased excitability, which develop due to a decrease in oxygen delivery to brain tissue.
Diagnosis of folate deficiency anemia
It is necessary to diagnose folate deficiency anemia before starting treatment, since folic acid deficiency is often combined with iron deficiency, vitamin B12 and protein deficiency. The plan for the necessary laboratory and instrumental examinations includes the following tests:
- level of folic acid in the blood;
The significance of the internal factor
Cyanocobalamin from food products entering the gastrointestinal tract is absorbed using the so-called intrinsic factor (IF)
. Here's how it happens:
- In the stomach, B12 is absorbed with the internal factor, as was previously thought, in no hurry; it finds protein-R and combines with it in order to be sent to the duodenum in the form of a complex “Vit B12 + protein-R” and there, under the influence of proteolytic enzymes, break down;
- In the duodenum, cyanocobalamin is freed from protein-R and, in a free state, meets the internal factor that has arrived there, interacts with it and forms another complex - “Vit B12 + VF”;
- The “Vit B12 + VF” complex is sent to the jejunum, finds receptors intended for internal factor, connects with them and is absorbed;
- After absorption, cyanocobalamin “sits” on the transport protein transcobalamin II, which delivers it to the sites of primary activity or to a depot to create a reserve (bone marrow, liver).
It is obvious why such great importance is given to the internal factor, because if everything is in order with it, then almost all of the cyanocobalamin supplied with food will safely reach its destination. Otherwise (in the absence of VF), only 1% of vitamin B12 will leak through the intestinal wall by diffusion, and then the person will not receive the amount of such an important vitamin he needs.
The body's daily need for cyanocobalamin is from 3 to 5 mcg, and its reserve is from 4 to 5 grams, therefore, it can be calculated that if the supply of vitamin B12 is completely excluded (for example, during a gastrectomy), then the reserves will dry up in 3- 4 years. In general, the supply of vitamin B12 is designed for 4-6 years, while folic acid, in the absence of supply, will disappear in 3-4 months. From this we can conclude that B12 deficiency during pregnancy does not threaten if its level was normal before, but folic acid, if the woman did not consume raw fruits and vegetables, is quite capable of falling below the permissible limit and creating a deficiency state (the development of folate deficiency anemia ).
Vitamin B12 is found in products of animal origin, folic acid is found in almost all food products, however, cyanocobalamin tolerates heat treatment remarkably well for a long time and is preserved for entry into the body, which cannot be said about folic acid - after 15 minutes of boiling, this vitamin does not there will be no trace...
How do B12- and B9-deficiency states manifest?
If the described conditions are classified as anemia, then it goes without saying that they will be characterized by all the symptoms of anemia:
- Rapid onset of fatigue even with minimal physical activity, weakness, decreased performance;
- Episodes of darkening of the eyes;
- Tendency to hypotension (low blood pressure);
- Breathing disorders (the desire to speed up the pace or other movements cause shortness of breath);
- Periodic headaches, often feeling dizzy;
- Often there is a rhythm disturbance (tachycardia);
- The skin is pale and slightly yellow (subicteric);
- Problems develop in the oral cavity with signs characteristic of glossitis: the papillae are atrophied, the surface of the tongue is varnished, the tongue swells and hurts;
- Possible enlargement of the liver and spleen;
- Swelling of the lower extremities;
- Frequent bowel movements, which, however, may alternate with constipation;
- A noticeable decrease in appetite and, accordingly, weight.
Due to the fact that with a lack of cyanocobalamin, a triad of syndromes occurs (damage to the blood, gastrointestinal tract and nervous system),
and if there is a deficiency of folic acid, there is no suffering from the nervous system, the following symptoms indicating involvement of the nervous system in the pathological process will apply
only to the B12 deficiency state
:
- Funicular myelosis (degenerative pathology of the spinal cord), which in severity does not correlate with the clinical manifestations of anemia;
- Peripheral polyneuropathy with muscle weakness, sensitivity disorder and decreased tendon reflexes;
- In other cases, depression, memory impairment, and rarely mental disorders are observed due to anemia.
It should be noted that B12- and folate-deficiency conditions do not differ in rapidly progressing course and are not particularly rich in symptoms. Until recently, the diseases were classified as a pathology of old age, however, in recent years there has been a tendency towards “rejuvenation” - this kind of anemia has begun to occur in young people.
Diagnostics
Clinically manifested icterus of the sclera and jaundice of the skin are signs that give reason to immediately send the patient to the laboratory,
where the diagnosis of folate and B12 deficiency conditions begins.
The first stage of laboratory tests makes one suspect megaloblastic anemia:
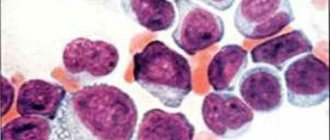
- Complete blood count (CBC) - typical for such conditions: low levels of red blood cells and hemoglobin, thrombocytopenia, neutropenia with polysegmentation, CP is usually higher than 1, macrocytosis, poikilocytosis, anisocytosis, in red blood cells - Jolly bodies, Cabot rings;
- Increased bilirubin values due to the unbound fraction in the biochemical blood test (BAC).
Considering that other hematological pathologies (hypoplastic and aplastic conditions, hemolytic anemia, leukemia) can give a similar picture of peripheral blood, the patient is required to undergo a puncture of the spinal cord, in which megaloblasts are found (a characteristic sign of B12-deficiency anemia), gigantic megakaryocytes and cells of the granulocytic series.
As a rule, after laboratory tests (or in parallel with them), the patient undergoes a “terrible procedure” - fibrogastroscopy (FGS), according to which it is clear that the gastric mucosa is atrophied.
Meanwhile, further diagnosis of B12-deficiency anemia requires its dissociation from anemia associated with a lack of vitamin B9.
It is very important to carefully collect the patient’s history: study his lifestyle and diet, thoroughly identify symptoms, examine the state of the cardiovascular and nervous system, but clarifying the diagnosis still requires laboratory tests. And here it should be noted that in any case, the differential diagnosis of these two anemias is difficult for conventional laboratories, because it creates the need to determine the quantitative values of vitamins, however:
- The microbiological method is far from perfect and gives only approximate results;
- Radioimmunological studies are not available to residents of villages and small towns, since the analysis requires the participation of modern equipment and highly sensitive reagents, which are the privilege of large cities.
In this case, for differential diagnosis, a urine test would be useful to determine the amount of methylmalonic acid in it: with B12-deficiency anemia, its content increases markedly, while with folate deficiency the level remains unchanged.
Treatment
They start with prescribing folic acid supplements. For pregnant women, this is most often the only purpose. In other cases, the treatment regimen is drawn up taking into account the causes of the disease. If you have an unbalanced diet, you need to review your diet and include foods rich in vitamin B9. Quitting alcohol abuse is also an important step in the fight against folate deficiency anemia.
Problems with internal organs require specific treatment, depending on the type of disease.
If the level of vitamin B12 in the blood is low, the patient is prescribed injections or tablets. This is very important because normalizing folic acid levels can mask the symptoms of B12 deficiency, which can cause nervous system dysfunction.