Causes of meningitis
Meningitis can be of infectious or non-infectious origin. The infectious form of the disease develops as a result of the penetration of microorganisms into the body: bacteria, viruses, fungi and parasites. Non-infectious meningitis develops in patients as a result of taking certain medications and the formation of tumors.
Make an appointment
In medicine, classification is used according to the type of pathogenic microorganisms. It is important for a modern person to know how to recognize meningitis and what types of disease exist:
- bacterial meningitis is most often caused by streptococci, meningococci, pneumococci and Haemophilus influenzae, which are transmitted by airborne droplets;
- viral meningitis. The most common form of the disease. This type is characterized by the least severity. The causative agents of viral meningitis are enteroviruses;
- fungal meningitis develops as a result of the activity of certain types of fungal microorganisms;
- parasitic meningitis.
The list of therapeutic measures for meningitis is determined by the factors that caused the development of the disease. Thus, when treating bacterial meningitis, antibiotics are prescribed, which are ineffective for viral meningitis. If a person knows how to recognize meningitis, then the likelihood of diagnosing the disease at the initial stage and the effectiveness of therapeutic measures are high.
It is not possible to determine meningitis on your own. The clinical picture of the disease is varied. Signs differ according to the etiological factor. The initial symptoms of meningitis are often mistaken for cold symptoms. As the infection spreads, the condition worsens sharply. The high risk of death due to meningitis persists for 1-2 days from the onset of the first pathological symptoms. Delayed diagnosis and therapy lead to the development of severe, life-threatening complications.
Meningitis
Meningitis is a disease that causes inflammation of the meninges: the protective membranes that cover the brain and spinal cord. Meningitis is most often caused by bacteria, viruses, protozoa and fungi. However, a non-infectious form of meningitis is possible, when the meninges become inflamed due to certain diseases, medications, or injuries. (1)
Causes of meningitis
The causes of the disease are various types of pathogens. Depending on their type, there are types of meningitis that they can cause:
- bacterial. It can be caused by various types of bacteria, including meningococci, staphylococci, streptococci, E. coli and others.
- viral. Possible pathogens of this form are mumps, herpes, influenza viruses, etc.;
- fungal can be caused by candida, cryptococcus;
- a form of meningitis caused by protozoa - its causes can be amoebas, toxoplasma and other protozoa;
- a mixed form of meningitis occurs if several pathogens are simultaneously detected in the body, each of which can cause meningitis.
Types, forms of meningitis
Depending on the speed of development of the disease, several forms are distinguished. Very rapid, sudden development of symptoms is a fulminant form of meningitis. The acute form of meningitis develops within 1–2 days. In subacute meningitis, symptoms develop over several days or weeks. Chronic meningitis lasts more than 4 weeks, and if after the symptoms disappear, the disease returns again, then it is recurrent meningitis.
Based on the type of inflammatory process, there are two types of meningitis - serous, which most often develops with a viral infection (enteroviruses, adenoviruses, mumps virus, influenza, tick-borne encephalitis) and purulent meningitis - a more severe form caused by a bacterial infection. The most common causative agents of purulent bacterial meningitis are meningococci, pneumococci, and Haemophilus influenzae type b (Hib).
Based on their origin, forms of meningitis are divided into primary and secondary. Primary develops as an independent disease. Secondary meningitis is a consequence or complication of an infection already existing in the body, for example, otitis media, influenza, tuberculosis, and often occurs in the form of serous meningitis.
According to the prevalence of inflammation, they are distinguished: spinal (or spinal cord meningitis) - the inflammatory process develops in the membranes of the spinal cord. If the inflammation is mainly localized in the upper part of the brain, then it is convexital meningitis, and with inflammation of the lower part of the brain, basal meningitis develops. The process, which involves both the brain and the spinal cord, is called cerebrospinal - this is how meningococcal meningitis often occurs. (1)
Symptoms of meningitis of the brain
Depending on the cause of meningitis, the symptoms of this disease may vary. But meningitis also has common symptoms called meningeal. They are divided into general cerebral symptoms - arising due to increased intracranial pressure and true meningeal symptoms, which arise due to inflammation of the lining of the brain. (1)
Among the early cerebral symptoms, headache most often appears. It can be widespread, or it can be observed in certain areas of the head; the severity of pain also varies. For many, the pain intensifies with noise, changing position, or turning on the lights. Young children may react to it with the so-called “brain scream” - these are repeated, monotonous, high-pitched screams.
The headache may be accompanied by severe sudden vomiting, which does not bring relief. There may be seizures, tics (uncontrolled movements of small muscles), and changes in consciousness.
Meningeal symptoms may include:
- typical pose with head thrown back, arms bent and legs pulled up to the stomach (“cooper dog pose”);
- rigidity (stiffness) of the neck muscles: an attempt to press the patient’s chin to the chest from the side fails;
- other symptoms indicating irritation of the meninges.
Other symptoms may vary depending on the type of pathogen that led to the disease and the type of meningitis. They are discussed separately in the description of the corresponding forms.
Viral meningitis
Viral meningitis can be caused by enteroviruses, including Coxsackie A, ECHO, mumps, parainfluenza viruses, viruses of the herpes family (causing herpes simplex, herpes zoster, Epstein-Barr disease, roseola infantile), tick-borne encephalitis virus and others.
According to the type of inflammation, this is most often serous meningitis.
The incubation period - the time from the moment the pathogen enters the body until the development of symptoms of the disease - in adults averages from 6 to 14 days. In children, it may be shorter or longer, and the signs of the disease may be less pronounced.
Viral meningitis clinic
As a rule, the first complaints to appear are those that may indicate an infectious disease: weakness, malaise, fever, headache. Then, within 1–3 days, meningeal symptoms appear, which may include neck stiffness, Brudzinski's symptoms, Kernig's sign, hypersensitivity to light, sounds, and touch. In infants, the fontanel may bulge and pulsate, and Lesage's symptom may be observed, in which the child, taken from the armpits, pulls his legs toward his stomach.
With some types of viral serous meningitis, the clinical picture may be unexpressed, erased, complaints may be moderate, and meningeal symptoms may appear erased and not obvious. Thus, meningitis that occurs against the background of adenovirus infection often occurs without meningeal symptoms, but with severe inflammation of the nasopharynx and upper respiratory tract, conjunctivitis.
Meningitis caused by the mumps virus can occur with intense abdominal pain, signs of pancreatitis, and inflammation of the testicles or ovaries.
A prolonged course can occur with meningitis caused by herpes viruses. It often begins with signs of herpes - typical blisters on the mucous membranes, herpes zoster, etc. Often, such meningitis occurs without meningeal symptoms.
Meningitis with tick-borne encephalitis is usually characterized by a rapid onset, with a rise in temperature, severe intoxication, muscle pain and meningeal symptoms. It can occur in waves - after an acute period, the temperature drops, and after a few days it rises again. Recovery is often delayed; weakness, asthenia, and neurological symptoms persist for quite a long time.
Diagnosis of viral meningitis
Only a doctor can make a correct diagnosis, so if you suspect that a patient may have meningitis, you should seek medical help. The doctor will interview the patient or his relatives, examine and assess the condition, and if necessary, in order to make sure that the symptoms are caused by inflammation of the meningeal membranes, he will prescribe a sample of cerebrospinal fluid and an assessment of its indicators.
Treatment
In most cases, treatment of viral meningitis is symptomatic. Recommends bed rest, dim lighting. At the onset of the disease, detoxification therapy is carried out according to indications, drugs are prescribed to alleviate symptoms: headache, vomiting, fever, abdominal pain, spasms, convulsions. For meningitis caused by a virus from the herpesvirus family, the doctor may prescribe an intravenous drip of the antiviral drug acyclovir.
With proper treatment, viral meningitis is usually quite mild, and the prognosis in most cases is favorable. (12)
Prevention
Vaccination in accordance with the National Vaccination Calendar of the Russian Federation can serve as the optimal way to protect against the risk of developing certain forms of viral meningitis. This is a vaccination against polio, mumps and measles viruses.
For other viruses, measures aimed at reducing the risk of transmission of the virus from carriers and patients to healthy people may be effective. These include:
- identification of sick people and timely separation of contacts (quarantine);
- compliance with personal hygiene and sanitary standards;
- strengthening and maintaining immunity;
- a set of measures from health authorities. (12)
Bacterial meningitis
Bacterial meningitis can be caused by meningococci, pneumococci, Haemophilus influenzae, tubercle bacilli, as well as staphylococci, salmonella, listeria and other bacteria. The inflammatory process in the membranes of the spinal cord and brain, caused by bacteria, in most cases is purulent.
“In 2015 in the Russian Federation, out of 2452 cases of purulent bacterial meningitis […] the etiological structure was dominated by meningococcus (44%). Next in frequency of isolation was pneumococcus (26%), followed by Haemophilus influenzae (10%). The share of other microorganisms accounted for 19%.” (3)
According to source (3) “the greatest risk of developing purulent bacterial meningitis of any etiology is typical for children under 5 years of age, while the risk of developing generalized forms of meningococcal infection is more pronounced in this group, followed by hemophilic meningitis in this age group, followed by pneumococcal meningitis”
Meningococcal meningitis
An acute onset of the disease is typical for this form. Intoxication and fever can be severe, as well as other symptoms. The intensity of complaints increases very quickly, there is a severe headache, fever, repeated vomiting that does not bring relief, a sharp increase in sensitivity to light, sounds, touches, and movement. Meningeal symptoms soon follow: “pointing dog pose,” Kernig’s and Brudzinski’s symptoms. In severe cases, the patient may experience convulsions, disturbances of consciousness, even coma.
In infants, the onset of purulent meningitis is accompanied by crying against a background of restless behavior, refusal to breastfeed, screams, a sharp reaction to touch (withdrawal of limbs, shuddering, increased crying), and convulsions. During the examination, meningeal symptoms may be detected - Lesage, stiff neck, typical meningeal posture.
As infection and inflammation spread and meningococci enter the blood, the patient's condition worsens. Meningococcemia (sepsis, blood poisoning) and infectious-toxic shock may develop. The symptoms described above will be accompanied by a hemorrhagic rash, and the functioning of the heart and blood vessels will deteriorate. With infectious-toxic shock, the deterioration of the condition can progress very quickly, fever and rash appear almost simultaneously, convulsions develop, and consciousness is impaired.
If you suspect meningococcal meningitis, it is recommended to seek urgent medical attention, as this form of meningitis can progress rapidly (even to death) and cause serious complications.
To make a diagnosis, the doctor relies on examination data and other examinations, based on the results of which he can prescribe cerebrospinal fluid tests, blood tests, and molecular diagnostic methods (for example, PCR) to clarify the type of pathogen. Based on the examination data, a diagnosis is established and treatment is prescribed: antibiotics, detoxification and symptomatic therapy; if necessary, correction of dehydration and other metabolic disorders can be carried out.
The duration of the disease with proper treatment can average from 2 to 6 weeks. Without treatment, there is a high probability of death or the development of severe complications leading to disability: according to the source, 10–20% of those who have had bacterial meningitis develop brain damage, hearing loss, cognitive impairment, and learning difficulties. In severe cases, gangrene of the fingers, toes, and ears is possible. (4)
Prevention
Currently, the following vaccines are registered in Russia for the prevention of severe forms of meningococcal infection.
- Meningococcal polysaccharide vaccines:
- monovalent (serogroup A) - monovalent against serogroup A polysaccharide dry;
- tetravalent (serogroups A, C, W, Y).
- Meningococcal conjugates:
- monovalent (serogroup C);
- tetravalent (serogroups A, C, Y, W).
Pneumococcal meningitis
This type of meningitis is caused by various types of pneumococci. Most often it develops in young children. “Young children under 2 years of age, whose bodies are unable to resist the infection, are especially defenseless against pneumococcus.” For this age group, pneumococci are the most common cause of severe forms of pneumonia, otitis media, and the second most common cause of bacterial meningitis. infection No. 1 and the most common cause of severe forms of pneumonia, otitis media, meningitis.” (9)
Pneumococcal meningitis occurs in the form of purulent meningitis, and can be primary or secondary, when it occurs against the background of an existing disease - otitis media, pneumonia, sinusitis.
The development of infection and, accordingly, complaints and clinical signs can develop in two forms. Primary pneumococcal meningitis develops, as a rule, acutely and is most typical for children over 5 years of age and adults. Body temperature rises sharply, symptoms of intoxication quickly appear - weakness, lethargy, drowsiness, nausea, headaches. After 2-3 days from the appearance of the first signs, meningeal symptoms and repeated vomiting without relief appear. Infants cry monotonously, periodically scream and moan, and the fontanel bulges. In children and adults, rashes may appear on the mucous membranes, in the form of small petechiae, resembling a hemorrhagic rash.
Often the process of inflammation affects the substance of the brain (meningoencephalitis), and against its background there are severe manifestations of the nervous system: convulsions, paresis, chaotic movements of the limbs, disturbances of consciousness, which can result in coma.
Secondary pneumococcal meningitis most often has a protracted course. Symptoms develop gradually over 2–7 days; at first they resemble ARVI; body temperature may be elevated, but sometimes may remain normal. Then, within a few days, the complaints become similar to those of acute pneumococcal meningitis.
To establish a diagnosis and prescribe adequate therapy, the doctor may order blood and cerebrospinal fluid sampling followed by laboratory testing. Treatment consists of prescribing antibiotics to which the pathogen is sensitive, taking measures to maintain the functioning of organs and systems, and symptomatic therapy. (12)
With timely treatment, the condition begins to improve during the first week, and the inflammation and the symptoms caused by it gradually subside. However, the prognosis for pneumococcal meningitis is serious, since with this form of meningitis “complications in the form of mental retardation, impaired motor activity, epilepsy and deafness are significantly more common than in the outcome of bacterial meningitis of other etiologies” (9). The prognosis can be especially difficult if meningitis transforms into a septic form, which can lead to endo- and pericarditis, arthritis and other serious complications.
Prevention
According to the website yaprivit.ru, “mass vaccination reduces the incidence of pneumococcal meningitis by more than 80%... The carriage of pneumococci in children is decreasing, and accordingly, unvaccinated children and adults get sick less.”
In the Russian Federation, vaccination is carried out with the following vaccines:
- 10-valent pneumococcal conjugate vaccine - PCV10;
- 13-valent pneumococcal conjugate vaccine - PCV13.
Both of these vaccines can be used in children from 2 months of age and in adults.
- 23-valent polysaccharide vaccine - PPV23.
Can be used in children from the age of 2 years and adults. (6)(9)
Haemophilus influenzae meningitis (Hib meningitis)
This form of meningitis is caused by Haemophilus influenzae type b and is most often observed in children under 5 years of age, but can also occur in older children - up to 8 years of age, and an increase in incidence in adults has also been noted. (7)(9)
Complaints and symptoms depend on the age of the patient, the condition of his body and the duration of the disease. In children, Hib meningitis often begins suddenly, with fever, repeated vomiting, and headache. In young children, bulging fontanelle and severe anxiety. These general cerebral symptoms are accompanied by meningeal symptoms: Brudzinsky and Kernig symptoms, Lesage symptoms in children under one year of age, neck stiffness. Convulsions, disturbances of consciousness, even coma can also quickly appear.
If Hib meningitis develops as a secondary disease, then the development of symptoms is slow, starting with complaints about the underlying disease, and then the symptoms of meningitis and cerebral symptoms join.
Treatment begins immediately after diagnosis, even before receiving the results of blood and cerebrospinal fluid tests. Combinations of antibiotics are prescribed in large doses, symptoms are combated, complications are prevented, and after the examination data has been clarified, antibiotics are selected taking into account the identified pathogen.
The hemophilic form of meningitis is difficult to treat due to the peculiarity of the pathogen: Hib bacilli produce an enzyme that protects them from antibiotics. For this reason, a third of patients who received proper treatment develop various neurological complications: seizure syndrome, developmental delay, loss of hearing and vision. Mortality in severe purulent hemophilic meningitis can reach 16–20%. (1) (7) (9)
Prevention
A highly effective measure for preventing Hib meningitis (and other forms of Hib infection) is vaccination (8). Currently, vaccination of all children in the first year of life against this infection is included in the vaccination schedules of more than 180 countries around the world (8). Currently in Russia, unlike most other countries, the vaccine against Hib infection is recommended only for children from certain risk groups (5). In Russia, vaccines against Hib infection are available both in the form of monovaccines and as part of combined (5-, 6-component) vaccines.
Show sources
Sources
- Berezhnova I. A. Infectious diseases. - Textbook / I. A. Berezhnova - M.: RIOR. - 2007. - 319 p.
- Childhood diseases: textbook / Ed. A. A. Baranova - 2nd ed., - M.: GEOTAR-Media. - 2009. - 1008 p.
- Information and analytical review “Meningococcal infection and purulent bacterial meningitis in the Russian Federation. 2015.” Russian reference center for monitoring bacterial meningitis. - M., - 2021.
- Meningococcal infection [Electronic resource]. — Access mode: https://www.yaprivit.ru/diseases/meningokokkovaya-infekciya — Article. — (Date of access: 04/17/2018).
- Order of the Ministry of Health of the Russian Federation dated March 21, 2014 No. 125n “On approval of the national calendar of preventive vaccinations and the calendar of preventive vaccinations for epidemic indications” (with amendments and additions). — Access mode: https://base.garant.ru/. (Date of access: 04/17/2018).
- Abramtseva, M.V. Meningococcal infection. Conjugate polysaccharide meningococcal vaccines and new generation vaccines. Message 3 / M. V. Abramtseva, A. P. Tarasov, T. I. Nemirovskaya // Journal “Biopreparations. Prevention. Diagnostics. Treatment". Volume 16 No. 1 (57) / January-March 2021. — P. 3–13.
- Journal "Medical Alphabet" No. 6 / 2021, volume No. 1 Epidemiology and hygiene.
- World Health Organization. Haemophilus influenzae type b (Hib) vaccination position paper - July 2013. Wkly Epidemiol Rec 2013; 88:413-426 [Electronic resource]. — Access mode: https://www.who.int/wer/2013/wer8839.pdf. (Date of access: 04/17/2018)
- Pneumococcal infection [Electronic resource]. — Access mode: https://www.yaprivit.ru/diseases/pnevmokokkovaya-infekciya/. - Article. — (Date of access: 03/19/2017). (as of 04/17/2018)
SPRU.MENAC.18.03.0031(1)
Risk group
Children and the elderly are at risk for meningitis. In addition, this disease is often diagnosed in people with an absent spleen and immunodeficiency.
The spread of meningitis, like all other infectious diseases, is more active in crowded places, closed groups, for example, in kindergartens, schools, student dormitories, barracks, since it is easier to get meningitis if you are in the company of asymptomatic carriers.
Most often, meningitis is transmitted by airborne droplets. This mechanism of infection transmission is considered the most common and characteristic of meningitis of viral origin. The infectious agent is transmitted through coughing, sneezing, kissing and sexual contact.
Newborn babies can become infected from an infected mother through the birth canal. The likelihood of infection is especially high in children born by caesarean section. Bacterial and viral meningitis can be transmitted this way.
Infection with meningitis can occur through the oral-fecal route: through dirty food or untreated water.
In addition, meningitis can develop as a result of the bite of an insect or animal that carries an infectious agent.
Encephalomyelitis - symptoms and treatment
Diagnosis is based on identifying symptoms of multifocal damage to the nervous system. When collecting anamnesis, it should be taken into account that the disease occurs against the background of infectious manifestations or following them. Encephalomyelitis may also be associated with vaccinations or tick bites. Therefore, the patient is asked:
- whether he was in an endemic area;
- whether he was bitten by a tick;
- gave him vaccinations;
- whether there are any somatic diseases.
In a neurological examination, attention is paid to the level of consciousness, paresis or paralysis, disturbances of sensitivity and function of the pelvic organs, and autonomic disorders.
In laboratory studies of acute disseminated encephalomyelitis (ADEM), inflammatory changes are often found: leukocytosis (increased white blood cell count), increased ESR (accelerated erythrocyte sedimentation rate), and sometimes lymphopenia (decreased lymphocyte count) [7].
In patients with suspected encephalomyelitis, a cerebrospinal fluid examination is indicated. Changes in the cerebrospinal fluid in ADEM were noted in 2/3 of cases. They are characterized by mild lymphocytic pleocytosis (increased number of lymphocytes) and increased protein levels. Oligoclonal IgG, characteristic of multiple sclerosis, is often absent, but can occur in 30% of children and up to 50% of adults, making differential diagnosis difficult [12][16][17].
MRI is considered the main neuroimaging method for diagnosing ADEM. In the disease, large multiple, asymmetrical lesions are detected, involving the subcortical and central white matter, as well as the transition of the cortical gray and adjacent white matter of the cerebral hemispheres, the cerebellar hemisphere, the brain stem and the spinal cord. Often the deep gray matter is involved: the thalamus and basal ganglia. Typically symmetrical location of lesions. The corpus callosum is not usually involved, but may be involved in large lesions [7][18].
Four patterns of cerebral damage in acute disseminated encephalomyelitis (ADEM) have been identified according to MRI data:
- ADEM with small lesions (less than 5 mm);
- ADEM with large confluent, pseudotumorous (tumor-like) foci with frequent intense surrounding edema and mass effect (compression, displacement, deformation);
- ADEM with additional symmetrical bilateral involvement of the thalamus;
- acute hemorrhagic encephalomyelitis with hemorrhages in large foci of demyelination [18].
However, changes in MRI do not affect prognosis and disability and can change during treatment [7].
The differential diagnosis of disseminated encephalomyelitis is difficult. An acute neurological deficit with symptoms of diffuse damage to the brain and spinal cord requires differential diagnosis, primarily with multiple sclerosis, neuromyelitis optica (Devic's disease), secondary disseminated encephalomyelitis (infectious, post-vaccination, etc.).
In differential diagnosis with multiple sclerosis, it should be taken into account that ADEM often develops acutely against the background of or following infectious manifestations. With it, unlike multiple sclerosis, both white and gray matter can be involved. Also, ADEM often involves the peripheral nervous system with corresponding symptoms - pain, paresis, decreased reflexes. The fact that in most cases ADEM has a unidirectional course, with a transition from the acute period to recovery, and then to residual effects, also helps in diagnosis. In multiple sclerosis, a secondary progressive course is noted. In the case of chronic forms of REM, differential diagnosis becomes even more difficult [5][7][8][9][10]. Therefore, criteria for differential diagnosis between ADEM and multiple sclerosis based on MRI data have been proposed:
1) absence of a diffuse bilateral (two-sided) focal pattern;
2) the presence of “black holes” (areas of clearing inside plaques);
3) the presence of two or more periventricular lesions (around the ventricles of the brain).
Identification of two of these signs makes it possible to distinguish the first attack of multiple sclerosis from ADEM with a sensitivity of 81% and specificity of 95% (sensitivity - the ability to distinguish one disease from another and specificity for each disease) [19]. Also, in ADEM, in contrast to multiple sclerosis, the following characteristics of lesions are indicated: a single lesion, a large zone on one side, cortical lesions, damage to the subcortical (subcortical nodes) gray matter (thalamus, basal ganglia) [1][6]. Finally, the International Panel of Experts on Multiple Sclerosis reached a consensus and proposed criteria for the diagnosis of ADEM [20]. However, even under these circumstances, some patients must be observed in the future at risk for multiple sclerosis.
Criteria for the diagnosis of acute disseminated encephalomyelitis (ADEM):
- subacute encephalopathy (impaired level of consciousness, behavior or cognitive functions);
- development within 1 week to 3 months, the development of new symptoms is allowed, including demyelinating syndromes such as optic neuritis, myelitis during the first three months from the onset of the disease, if not separated by a period of complete remission from the initial symptoms (in this case it is necessary to diagnose multiple sclerosis);
- subsequent improvement and recovery, although residual neurological deficits may persist;
- on MRI, symptomatic lesions in the white matter predominate (acute, multiple, less often - one large lesion; as a rule, the presence of at least one large lesion 1-2 cm in diameter; variable accumulation of contrast agent - contrast accumulation is not necessary; may additionally be detected lesions in the basal ganglia, but their presence is not necessary).
Neuromyelitis optica or Devic's disease (this is a separate disease that differs in course and approaches to therapy) is a rare demyelinating disease of the nervous system. The disease manifests itself with a variety of symptoms - blurred vision, lower paraparesis, dysfunction of the pelvic organs. In some cases, damage to the optic nerves and spinal cord can occur simultaneously, but more often - with a time interval that can be months, years and even decades. Symptoms worsen over several days and subside over weeks and months, and often complete recovery does not occur. With each subsequent attack, the neurological deficit increases and leads to severe disorders of the motor, sensory, visual and autonomic systems [21]. MRI reveals lesions in the spinal cord; in 80% of cases they are localized in the thoracic region. In most patients in the acute phase of myelitis, MRI reveals extensive lesions of more than three vertebral segments [6]. Laboratory studies reveal antibodies to avkaporin-4, which correlate with disease activity and decrease with treatment with rituximab, azathioprine, and cyclophosphamide[21].
In case of secondary encephalomyelitis, a history of infections should be looked for (for example, measles, rubella, chickenpox) or indications of a vaccination given the day before. Most often, neurological complications are caused by the rabies vaccine, and in young children - by the pertussis vaccine [8]. Since REM in borreliosis occurs at the third stage of the disease, these patients may have indications of previous symptoms: tick bite, ring-shaped erythema, lymphadenopathy, joint pain, damage to the peripheral nervous system - Bannwart syndrome, and in the late stage - atrophic acrodermatitis ( inflammatory changes in the skin of the hands and feet and its thinning) [11]. In etiological diagnosis, bacteriological and serological examination of blood and cerebrospinal fluid is important. If borreliosis is suspected, an ELISA test is performed to determine the presence of specific IgM and IgG antibodies to borrelia in the blood.
If herpes infections are suspected, PCR of the cerebrospinal fluid is performed to detect the presence of herpes virus DNA. Similar studies are being conducted for other infections. The results obtained are important for prescribing treatment.
Symptoms of meningitis in adults
Meningitis usually has a sudden onset. The first symptoms of meningitis in adults are: fever, headaches, vomiting (the so-called meningeal triad). However, these pathological signs of meningitis also accompany other infectious diseases, so it is important to know the features of the manifestation of meningitis.
Meningitis is characterized by rapid development with pronounced signs of intoxication:
- headache;
- high fever and chills;
- confusion and loss of consciousness;
- convulsions;
- skin rash;
- muscle weakness;
- drowsiness;
- photophobia, increased skin sensitivity, reaction to sound;
- stiff neck;
- loss of appetite, nausea, vomiting;
- conjunctivitis;
- increased heart rate.
In patients with meningitis, the first sign of the disease is often a rash on the skin and mucous membranes. The rash is initially hemorrhagic in nature, sometimes spots and papules appear on the skin. The rash is considered an allergic reaction to medication.
Headache
A severe headache should alert you. Headaches caused by meningitis feel different from other types of pain. Their intensity is much higher than that of headaches associated with dehydration or migraines. Taking over-the-counter pain medications does not provide relief.
Nausea and vomiting
Nausea and vomiting that occur with a headache are not absolute signs of meningitis. These symptoms may accompany other diseases, such as migraine. Close attention should be paid to other conditions that occur along with vomiting and nausea.
Vomiting with meningitis rarely occurs once, most often it is repeated, repeated, and is not associated with food intake.
Heat
An increase in body temperature, like other symptoms, may indicate the development of meningitis. With this disease, the temperature is usually much higher than with acute respiratory infections. In addition, taking antipyretic drugs for meningitis is ineffective - it is very difficult and short-term to reduce the temperature.
The temperature during meningitis can be moderate, high and ultra-high. Moderate temperature ranges from 380 to 390C, high from 390 to 420C, ultra-high from 420C above.
Meningitis in a child without fever occurs in several cases:
- if a child has a concomitant infection of the nasopharynx, meningitis in this case is considered a secondary disease.
- if the child is premature, the infection occurred in utero, during childbirth, after childbirth, then often the disease does not manifest itself as an increase in temperature - the symptoms of meningitis are smoothed out. This condition is associated with poor functioning of the baby’s immune system and morphofunctional immaturity of the body.
- if meningitis develops in a newborn after birth, the first symptoms of the disease will appear after 20-25 days. At this point, the level of antibodies received from the mother in the child’s blood decreases. Very often, such meningitis occurs in the initial stages without fever.
- Viral meningitis often occurs without fever. It goes away in a mild form within a few days.
Regardless of whether the child has a fever or not, when the first symptoms of meningitis appear, you should immediately consult a doctor.
Pain in the neck
Quite often, patients with meningitis complain of pain and a feeling of tension in the neck, and it is difficult for them to turn or raise their head. This is due to pressure from the inflamed membranes of the brain. This symptom can also be observed when the neck muscles are strained or injured from a sudden movement of the head.
The suspicion of meningitis can be confirmed by bending the patient's hips in a horizontal position - the occurrence of pain in the neck while performing this movement is a sign of meningitis.
Difficulty concentrating
Inflammation of the meninges during meningitis is associated with perception difficulties in patients. It is difficult for them to read an article to the end, concentrate on a conversation, or complete the task at hand. The degree of confusion may worsen as brain swelling increases. In addition to lethargy and confusion, patients experience a drop in blood pressure, shortness of breath, and noisy shallow breathing.
Lethargy, drowsiness
Patients become unable to act independently, they develop drowsiness and lethargy. This condition occurs as a consequence of general intoxication of the body or cerebral edema. Bacterial meningitis can be accompanied by a sharp depression of consciousness and even coma.
Photophobia
A manifestation of photophobia in patients with meningitis is severe pain that occurs in bright light. The appearance of pain and sensitivity of the eyes, as a reaction to light, is considered an alarming signal, as it is a characteristic sign of meningitis.
Convulsions
Convulsions, sometimes with involuntary urination and disorientation in space, are observed in 20% of patients with meningitis. Their course is similar to epileptic, or the appearance of tremor of individual muscles and individual parts of the body is observed. The occurrence of seizures (generalized and local) is associated with irritation of the cortex and subcortical structures of the brain.
Characteristic rash
A hemorrhagic rash on the skin and mucous membranes is not a specific symptom of meningitis. It appears in 25% of patients with bacterial meningitis and is most often observed in diseases of a meningococcal nature, since it is meningococcus that causes damage to the internal walls of blood vessels. The appearance of skin rashes is usually observed 15-20 hours after the onset of the disease. In this case, the rash is polymorphic - it can be roseolous, papular, in the form of nodules or petechiae. The rashes have an irregular shape and may protrude above the skin level.
Psychomotor agitation, anxiety
Anxiety, agitation and disorientation occur in patients with a form of the disease such as meningoencephalitis at the onset of the disease. With the bacterial form of meningitis, similar symptoms may appear 4-5 days after the onset of the disease. After psychomotor agitation, patients may experience loss of consciousness or coma.
At the beginning of the disease, as well as in later stages, patients with meningitis may develop symptomatic psychosis, manifested by agitation or, conversely, lethargy, delirium, visual and auditory hallucinations.
Delusions and hallucinations can occur in patients with lymphocytic choriomeningitis and meningitis, which is caused by the tick-borne encephalitis virus.
Among the etiological factors of meningitis, sinusitis is distinguished. The accumulation of purulent contents in the sinuses without proper treatment can lead to the spread of infection to the meninges. In such cases, meningitis is considered as a complication of sinusitis. The effectiveness of treatment for sinus inflammation depends on the quality of the diagnosis.
When the brain is inflamed: what is encephalitis?
On the one hand, the disease is not widespread. But it still happens, especially in certain regions. And, as you know, he who is forewarned is armed.
Irina Sergeevna Ignatieva, a neurologist at the Clinic Expert, Smolensk, answers questions about encephalitis.
– Irina Sergeevna, let’s start with a definition: what is encephalitis?
– In short, encephalitis is an inflammation of the brain substance. When, for example, we talk about meningitis, we mean inflammation of the membranes of the brain. And with encephalitis, it is its substance that becomes inflamed. In the International Classification of Diseases (ICD-10), encephalitis, as the main disease, is listed under code G04. Its subspecies have different designations.
– What are the causes of encephalitis?
– Primary encephalitis occurs as a result of virus penetration through the blood-brain barrier. They can be caused, for example, by the herpes virus or arbovirus, which is carried by ixodid ticks. In some cases, the disease develops as a result of complications after vaccination. Secondary encephalitis occurs after influenza, measles, and chickenpox.
Read more about chickenpox in children in our article
– Is encephalitis a seasonal or regional disease?
– Encephalitis can be both a seasonal and regional disease at the same time. For example, tick-borne encephalitis. The peak incidence occurs in the spring and summer – ticks are most active at this time. Now about regionality. Mostly ixodid ticks (ticks that carry the tick-borne encephalitis virus) are found in Siberia, the Far East, the Urals, but sometimes also in the Central Federal District. And, say, for herpetic encephalitis, neither seasonality nor regionality are important - this disease can develop in a person in any area and at any time.
Let us also note this fact: you can also get tick-borne encephalitis as a result of eating raw, virus-containing cow's or goat's milk.
– What are the symptoms of encephalitis?
– This is headache, nausea, vomiting, fever (increase in body temperature more than 37 degrees Celsius), confusion and disorientation in space, convulsions, motor and sensory disturbances may be present. In some cases, mental disorders are observed.
– Irina Sergeevna, I have come across this formulation: to identify viral encephalitis, the cerebrospinal fluid is examined. What is it about?
– We are talking about diagnosing the disease. If encephalitis is suspected, a lumbar puncture is performed to examine the cerebrospinal fluid, which is called cerebrospinal fluid.
It is necessary to take a general blood test, conduct an EEG, MRI and CT scan of the brain to exclude other diseases (tumor, brain abscess).
If an MRI of the brain showed... Doctors from Expert Group answer some of the most frequently asked questions about MRI of the brain and its vessels
– If encephalitis can be caused by viruses, then perhaps there are corresponding vaccinations?
– The vaccine has been developed only against tick-borne viral encephalitis. Vaccination against it is included in a special calendar of preventive vaccinations for epidemic indications. That is, such a vaccination is not included in the national calendar; it is relevant only for certain, endemic regions - we talked about them above. In total, three vaccinations are given: the second - two weeks after the first, and the third - a year after the second. Moreover, vaccination must be planned in such a way that at least two weeks pass from the moment of the second vaccination to a possible encounter with a tick.
– How effective is the vaccine against encephalitis?
– I repeat: if we are talking specifically about tick-borne encephalitis – almost one hundred percent.
– How is encephalitis treated?
– Every medical institution – especially in endemic areas – should have a certain supply of so-called anti-encephalitis immunoglobulin. This is an immunologically active protein fraction that is isolated from donor serum or plasma of a vaccinated person. It is administered intramuscularly to the sick person, and the antibodies begin to fight the virus. Let me emphasize: here again we are talking specifically about tick-borne encephalitis.
In addition, symptomatic therapy is used: antipyretic, painkillers, and, if necessary, medications that replenish the volume of fluid in the body.
– Is the encephalitis virus transmitted from person to person?
- No.
– What will help you avoid getting sick?
– Vaccinations against tick-borne encephalitis. In addition, in endemic areas, the area is treated with special anti-tick preparations. After you have been in nature, you should carefully examine yourself and those you went with in order to promptly detect and remove ticks from your body. If it still manages to attach itself, you should not try to get rid of it yourself; it is better to get to the nearest emergency room or any medical facility where specialists will take care of this - so that no fragments of the arthropod remain in the body.
To minimize the risk of secondary encephalitis, it is necessary to be vaccinated against measles, mumps, influenza, chicken pox, and herpes. Avoid crowded places during ARVI epidemics. It won’t hurt to wear cotton-gauze bandages at such times. If you have herpes or any other ailment of an infectious nature, you must promptly seek medical help.
It is also advisable to exclude factors that lead to a weakening of the body’s defenses: lack of sleep, stress, hypothermia, excessive physical activity.
Interviewed by Igor Chichinov
The editors recommend:
Attack to the head. How to protect yourself from summer meningitis?
Will an MRI show meningitis?
What is ARVI?
How to prepare for flu season?
Vaccinations: where is the truth and where is the lie?
For reference:
Ignatieva Irina Sergeevna
Graduate of the Faculty of Medicine of the Smolensk State Medical Academy in 2004.
In 2005, she completed her internship, and in 2007, her clinical residency in neurology.
Currently, he is a neurologist of the first category. Conducts appointments at the “Expert Clinic” Smolensk at the address: st. 8 March, no. 20.
Sinusitis and meningitis: the relationship of diseases
Meningitis develops as an independent disease and can be a complication of pathological processes. Sinusitis and meningitis are interrelated, since the accumulation of pus in the maxillary sinuses can cause inflammation of the lining of the brain. It is important for people at risk to know how sinusitis turns into meningitis and what symptoms the patient experiences.
The development of complications with sinusitis is rare, since modern specialists use effective treatment methods. However, if treatment is untimely and ineffective against the background of reduced immunity, the patient may develop meningitis. If a patient suspects meningitis or their health has sharply worsened, it is necessary to consult a general practitioner or neurologist, who will prescribe an examination and determine the cause of the problem.
The most important and revealing test for suspected inflammatory processes in the membranes of the brain and spinal cord is a lumbar puncture. It is necessary to examine the cerebrospinal fluid to identify the cause of inflammation and prescribe adequate therapy.
Magnetic resonance imaging (MRI) in St. Petersburg
MRI of the brain. T2-weighted axial MRI. Multiple sclerosis. Color processing of the image.
Radiation diagnostics does not allow us to speak with a high degree of certainty about the pathogen; for this, bacteriological methods and detection of antibodies are used. At the same time, radiation diagnostic methods make it possible to talk about the extent of the lesion, complications and monitor the effectiveness of treatment. From the point of view of morphological changes, the infectious origin causes changes mainly such as meningitis, encephalitis, and brain abscess. MRI of St. Petersburg allows you to choose the location of tomography, and we have very extensive experience in MRI examination of the brain for infections. and MRI of the brain are the most important methods for morphological assessment of the state of the brain. Ultrasound duplex scanning is an additional method used when it is necessary to assess blood flow. The latter suffers mainly from cerebral edema. In addition, the infection may be complicated by arterial or venous thrombosis.
Bacterial infections
Meningitis
Meningitis is an inflammation of the lining of the brain. Usually accompanied by inflammation of the lining of the ventricles - ventriculitis. Inflammation of the arachnoid membrane leads to disruption of the blood-brain barrier, isolation from the body’s immune system, and increased vascular permeability. As a result, swelling and impaired blood supply develop. Pathogens: in newborns - streptococci (over 60%) and E. coli, in children - hemophilus and Nysseria (meningococcus), in adults - streptococcus pneumonia and Nysseria. In addition to bacterial ones, there are viral, tuberculous and fungal meningitis. Routes of penetration of the pathogen: hematogenous (usually the nasopharynx), extracerebral - through the inner ear (otitis media, mastoiditis, sinusitis) and direct - infection during surgery. The frequency is 0.25-1 per 1000 in newborns, 4-6.5 per 100 thousand in children, about 4 per 100 thousand in adults. 70% up to 5 years. Mortality varies greatly depending on the pathogen, the severity of infection, the age of the patient and the state of immunity. If the effectiveness of antibacterial therapy is insufficient, it reaches 15-30%.
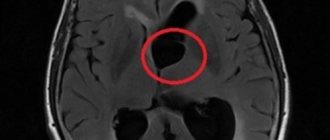
Clinical manifestations consist of headaches, fever, and may include nausea, vomiting (35%), convulsions (30%), and impaired consciousness. Very sharp start. In the neurological status, meningeal signs are determined (50%). The main diagnostic method is lumbar puncture and CSF examination. CT and MRI have a role in identifying complications. Complications are observed in 50% of patients - these are venous sinus thrombosis, arterial or venous infarction (30%), cerebritis and brain abscess, subdural accumulation of exudate (20-50%) and empyema (2%), ventriculitis (newborns - 92%, adults – 30%), hydrocephalus, cerebral edema. Non-contrast CT and MRI for uncomplicated meningitis are insensitive in 50% of cases, in other cases they reveal hydrocephalus, swelling of the gyri, widening of the interhemispheric fissure, and obliteration of the cisterns. After contrasting, there is an enhancement of the membranes (pachymeningitis) and, sometimes, the grooves (leptomeningitis). With duplex scanning, an increase in resistance indices indicates increased intracranial pressure.
Brain abscess
ICD-10 considers brain abscess as an independent disease. However, the first stage of brain damage caused by a purulent infection is cerebritis. Its early stage lasts 3-5 days and is not accompanied by macroscopic changes. In the late stage of cerebritis (days 5-14), an area of necrosis forms. After the 14th day, an abscess capsule gradually forms. The mortality rate from brain abscess is 5-50%, depending on the effectiveness of antibiotic therapy.
CT and MRI in the early stages of cerebritis reveal edema, there may be parenchymal contrast, in the late stage - central necrosis and peripheral edema, peripheral contrast is noted. The formed abscess has a contrasting capsule, its walls are smooth, their thickness is up to 5 mm. On DWI-type MRI, the contents of the abscess are bright, which distinguishes them from intratumoral necrosis.
| MRI of the brain. Brain abscess. Axial MRI type FLAIR. | MRI of the brain. Axial T1-weighted MRI with contrast. Brain abscess. | MRI of the brain. Brain abscess. Axial diffusion-weighted MRI. |
Venous sinus thrombosis
Venous sinus thrombosis is a consequence of occlusion of the sinus and/or cortical vein. Pathogenesis is associated with external compression (edema during infection, tumor invasion) and partial thrombosis (hypercoagulation). The consequence of venous thrombosis is a heart attack with a hemorrhagic component. The typical localization of infarctions in superficial vein thrombosis is at the junction of the white and gray matter, and in deep vein thrombosis (Rosenthal) - symmetrically in the visual thalamus. The mortality rate is very high.
On non-contrast CT scans, a thrombus is sometimes visible in the form of a “delta sign” - a dense triangular area (usually in the superior sagittal sinus). Contrast-enhanced CT scans show a “reverse delta sign,” that is, an unenhanced triangle. Only both signs together have diagnostic value. Additionally, venous infarctions may be detected.
CT. Hypodense area of infarction in the left temporal lobe. Hyperdense triangular area in the left transverse sinus.
On non-contrast MRI of the brain, a thrombus is visible in the form of an area of hemorrhage, the signal from which depends on the period. MR venography demonstrates absence of blood flow. With MRI, false-positive results are common due to congenital sinus hypoplasia, leak-in effect (loss of signal) and developed arachnoid granulations.
| MRI of the brain. Hyperintense with hemorrhage (dark deoxyhemoglobin) infarct area in the left temporal lobe on T2-dependent MRI images. | Lack of blood flow in the left transverse sinus with MRI. |
Arachnoiditis
Arachnoiditis is a general term that reflects inflammation of the membranes. Arachnoiditis of the brain is a rare diagnosis. Visible only on MRI of the brain with contrast as enhancement of the basal cisterns.
MRI of the brain. T1-weighted axial MRI with contrast. Arachnoiditis.
Viral encephalitis
Encephalitis is a diffuse parenchymal inflammation of the brain. Etiology - the disease can be caused by herpes infection, arboviruses, enteroviruses, echoviruses. Herpes is the most common cause of encephalitis. In adults, 95% of cases of herpes infection are caused by the herpes simplex virus type 1, in children by the herpes simplex virus type 2. In children, herpes is a primary infection, in adults it is the reactivation of latent viruses that enter the brain hematogenously or along the trigeminal and olfactory nerves . The frequency in adults is about 3 per 100 thousand or 10-20% of all viral encephalitis. Isolated sporadic cases are observed in newborns. Clinic: headache, fever, additionally – mental disorders, aphasia, convulsions, paresthesia, meningeal signs. The mortality rate for untreated herpetic encephalitis type 1 reaches 70%, with effective treatment - 30%; with untreated type 2 - 15% (local) - 60% (disseminated).
CSF cultures are positive in less than 5%. Antibodies appear in the blood only after 1-3 weeks. Therefore, the standard is a DNA test (after 24 hours) and a trial treatment with acyclovir.
CT and MRI of the brain reveal encephalitis no earlier than 3-5 days. Early signs consist of low-density fields in one or both temporal lobes on CT and hyperintensity in the same areas on T2-dependent MRI. MRI of the brain may show involvement of the lower frontal lobe and insula. Later, foci of hemorrhage appear, identified on T1-weighted MRI of the brain and a spotty type of enhancement on MRI of the brain with contrast.
| MRI of the brain. T2-weighted axial MRI. Herpetic encephalitis. | MRI of the brain. T1-weighted axial MRI after contrast. Herpetic encephalitis. |
Demyelinating diseases
Demyelinating diseases are a group of diseases, the main symptom of which is the destruction of the myelin sheaths of the nerves. In the popular MRI section there is a special article dedicated to MRI of multiple sclerosis. Many demyelinating diseases affect not only the brain, but also the spinal cord; MRI of the spinal cord in infectious diseases is described in a special section.
Acute disseminated encephalomyelitis
Acute disseminated encephalomyelitis (post-infectious encephalitis) is an autoimmune disease that occurs after a viral infection or vaccination (3-6% of cases). The pathophysiology of ADEM closely resembles the early stages of multiple sclerosis. Currently, ADEM is considered an acute demyelinating process. A variant is hyperacute hemorrhagic ADEM. The frequency is about 1 in 100 thousand. The age of patients in 80% of cases is under 10 years. The latent period is from 2 to 20 days. Clinic: acute onset in the form of fever, impaired consciousness, lethargy, convulsions (25%), may be optic neuritis, hemiparesis and ataxia. Laboratory tests are nonspecific. Mortality reaches 10-30%. In other cases, complete recovery.
On CT, in 50% of cases, subcortical areas of low density are detected, which may have a ring type of contrast. The sensitivity of brain MRI is 80-90%, and in some patients, changes are detected only a month after the onset of symptoms. MRI features consist of multiple hyperintense lesions on T2-dependent MRI images, they are asymmetrical, often confluent. There are hemorrhages into the lesions. The localization of foci can be any. A characteristic sign of ADEM is the disappearance of lesions on MRI of the brain as the patient recovers.
Proton density MRI. ODEM. The lesions are indicated by arrows.
Multiple sclerosis
Multiple sclerosis is an autoimmune demyelinating disease of the central nervous system. The process consists of local myelin destruction, axonal damage, gliosis and plaque formation. The frequency is about 2 per 1000 population. The M:F ratio is 1:2. The age can be any (2-74 years according to the literature), the peak falls on the young (average 35 years). Several variants of the course of MS are known. It is usually undulating, with progressive neurological deficits from relapse to relapse. Clinical signs consist of sensory and motor disturbances, visual disturbances and pelvic disturbances (80%). Different authors have proposed different criteria for multiple sclerosis, all of which include the presence of several (from 2 to 9) lesions typically located on MRI. The McDonald 2010 criteria were adopted by the International Committee for the Diagnosis of MS - they include the spatial distribution of lesions and dynamics over time. Spatial - 1 or more lesions on T2 in at least 2 of 4 zones: periventricular, subcortical, infratentorial or spinal cord. Temporary: new lesions appear on T2 or contrast-enhanced T1 MRI, simultaneous presence of asymptomatic contrast-enhancing or non-contrast lesions. Criteria for primary progressive MS: disease progression over the course of a year + 2 of three criteria – at least 1 lesion in a typical area, 2 or more lesions in the spinal cord, positive CSF test.
The sensitivity of CT even in clinically obvious MS is less than 50%, and increases slightly with a triple dose of contrast. The sensitivity and specificity of MRI in the early stages is 70-80%. The lesions are hyperintense on T2-weighted and proton density images. On T1-dependent MRI, only “old” lesions are visible. The localization of lesions can be any, but typical is the lower third of the corpus callosum, periventricular, in the trunk and spinal cord. The shape of the lesions is typically round and ovoid, directed radially from the ventricles on sagittal MR (finger or Dawson sign), reflecting a perivenular process. The edges of active lesions are blurred, there is weak contrast (often ring-shaped or C-shaped), which becomes more obvious with increasing dose. A slight mass effect has been described in aggressive cases (Marburg variant). The concentric variant of multiple sclerosis (Baló variant) is distinguished by the large size of the lesion, slight swelling around it and a circular structure. Cystic lesions are extremely rare in multiple sclerosis. The administration of hormones in doses significantly exceeding the physiological needs of the body causes inhibition of proliferative inflammatory processes. However, corticosteroid therapy slows astrocytic gliosis and the cavities remain unfilled.
On diffusion-weighted images, the signal from plaques is increased, the ICD is also increased, but in active plaques it may be reduced.
MRI of the brain. Axial and coronal MRI, reflecting proton density, and FLAIR type. Typical lesions of multiple sclerosis.
MRI of the brain with contrast. Parenchymal (left) and ring (right) types of contrast enhancement for multiple sclerosis.
MRI of the brain. Cystic lesions of multiple sclerosis. FLAIR and T1-dependent MRI with contrast.
MRI of the brain. Multiple sclerosis lesion on diffusion-weighted MRI (left) and diffusion map (right).
Often the first manifestation of multiple sclerosis is optic neuritis. Optic neuritis is a clinical diagnosis when vision is acutely impaired and there is pain. Isolated lesions in the optic nerve may not be accompanied by lesions in the brain, or they appear later (even after 15 years), or do not appear at all.
MRI of the brain. Optic neuritis in multiple sclerosis. T1-dependent MRI with contrast - enhancement of the intracanalicular part of the optic nerve on the left.
You can read about MRI of multiple sclerosis and other demyelinations in a separate article on this site.
Differential diagnosis of multiple sclerosis lesions should be carried out with other diseases manifested by focal changes:
- Other demyelinations
- Migraine foci
- Vasculitis (Systemic lupus erythematosus, etc.)
- Behçet's disease
- Lymphoma of the central nervous system
- Anti-phospholipid syndrome
- Infections (borelliosis, sarcoidosis, syphilis, AIDS, etc.)
- Ischemic changes
- Metabolic disorders
Proton density MRI of the brain. Migraine lesions (arrows).
MRI of the brain. Axial MRI type FLAIR. Lesions of systemic lupus erythematosus (arrows).
Progressive multifocal leukoencephalopathy
Progressive multifocal leukoencephalopathy (PML) is a demyelinating disease of viral etiology that develops against the background of immunodeficiency. Etiology – caused by JC viruses from the papovavirus group; this is the reactivation of a latent infection against the background of immunodeficiency. The virus infects oligodendrocytes and destroys them, which leads to demyelination. The clinical picture consists of a local neurological deficit and impaired consciousness. Death occurs within 9 months from the onset of the disease.
On MRI of the brain, PML lesions are often bilateral, asymmetrical, and rapidly increase in size. In 1/3 the posterior cranial fossa is affected, in 10% of cases the posterior cranial fossa is isolated. There are multiple foci. The basal ganglia are often involved. Enhancement on contrast-enhanced MRI is rare and, when observed, is peripheral and weak.
MRI of the brain. MRI type FLAIR. PML. Confluent lesion in the left frontal and parietal lobes.
Infantile ataxia with central hypomyelination
An extremely rare variant of demyelination (“vanishing” white matter disease) is observed in children after infections or minor injuries. The etiology is unknown; perhaps a gene defect plays a major role. The white matter is affected mainly in the periventricular zones with microcystic degeneration and destruction of the fibers of the corpus callosum. The clinical picture is represented by a lag in psychomotor development, spasticity, cerebellar ataxia, and visual impairment. MRI of the brain reveals symmetrical confluent lesions in the white matter. On T2-weighted MRI they have CSF signal intensity. A feature of the course of the disease is a gradual improvement in clinical symptoms and a decrease in lesions on MRI of the brain. Unlike other demyelinations, MRI of the brain shows cerebellar atrophy and significant spread of white matter lesions, down to the subcortical areas. Differential diagnosis is more carried out with dysmyelogenous diseases, especially leukodystrophies, in which a similar picture is observed on T2-weighted MRI of the brain.
MRI of the brain. T2-weighted axial MRI. Vanishing white matter disease.
Granulomatous inflammation
Tuberculosis
Neurotuberculosis is a consequence of hematogenous introduction of mycobacteria from the primary focus to the brain. Inflammation begins with subpial or subependymal cortical granulomas. The consequence of granulomatous inflammation is basal leptomeningitis, hydrocephalus, and small infarcts in the area of the subcortical nuclei. Parenchymal damage manifests itself in the form of tuberculomas, abscesses and cerebritis. Clinical manifestations consist of low-grade fever, headaches, and sometimes seizures.
CT scan reveals infarcts, contrast enhancement of membranes and tuberculomas. Tuberculomas become calcified and look like “targets”.
On MRI of the brain, tuberculomas are typically hypointense, but can also be hyperintense and surrounded by edema. Signal enhancement on T1-weighted MRIs on contrast-enhanced MRI is homogeneous or ring-shaped (with calcification). Cerebritis and meningitis appear nonspecific.
CT. Neurotuberculosis. Foci of cerebral infarction.
MRI of the brain. Axial T2-weighted MRI. Neurotuberculosis. Tuburculoma.
Sarcoidosis
The pathological anatomy of sarcoidosis is very similar to tuberculosis. Brain damage is observed in 5% of patients with sarcoidosis. Neurosarcoidosis occurs in the form of leptomeningitis and parenchymal lesions.
On CT and MRI, sarcoids, unlike tuberculomas, do not have a calcified center. The localization of sarcoids on MRI of the brain can be any, but the typical hypothalamus and optic chiasm.
MRI of the brain. T1-dependent MRI with contrast. Neurosarcoidosis. Damage to the membranes, cranial nerves, lesions in the trunk (arrows).
Acquired immunodeficiency syndrome
The disease is caused by HIV viruses. Neurological disorders are observed in more than 80% of patients, and in approximately 10% they are the first manifestations. It is necessary to distinguish between the signs of HIV infection itself and the symptoms of layered (opportunistic) infection - cytomegalovirus, cryptococcosis, toxoplasmosis, tuberculosis, syphilis, PML or layered tumors - lymphoma and Kaposi's sarcoma. At the earliest stages of HIV infection, CT and MRI do not detect pathology. As it progresses, MRI of the brain in AIDS shows that the subcortical gray matter is affected - the dementia complex, and then damage to the white matter develops - atrophy and leukoencephalopathy.
MRI of the brain. Axial T1-weighted MRI with contrast. Dementia due to HIV infection: atrophy and leukoencephalopathy.
Toxoplasmosis is the most common infection associated with AIDS. Toxoplasmosis in AIDS is a reactivation of the infection.
CT and MRI of the brain show multiple nodular or ring-shaped lesions surrounded by vasogenic edema of varying severity. Most often, MRI lesions are found at the border of the white and gray matter, the basal ganglia and the thalamus opticum.
MRI of the brain. Axial T2-dependent MRI. Toxoplasmosis.
Cryptococcosis - occurs as an independent infection, as well as as an opportunistic infection in 6-7% of AIDS patients. It is a fungal infection and in AIDS occurs in the parenchymal form. Cysts, pseudocysts and multiple hyperintense foci are detected on T2-dependent MRI of the brain. Leptomeningitis does not always enhance on contrast-enhanced MRI. The choroid plexuses are dilated (plexitis). Other mycoses also occur with AIDS: candidiasis and coccidioidomycosis.
MRI of the brain. Axial T1-dependent MRI with contrast. Cryptococcosis. Lesions and leptomeningitis.
Cytomegalovirus infection occurs in the form of encephalitis and ventriculitis. Bilateral lesions with characteristic localization in semi-oval centers are identified.
MRI in St. Petersburg in leading centers; for any questions, please contact the administrator by phone. 676-66-48. When examining in an open MRI, there is no fear of confined space, but the examination takes a little longer.
Leave feedback.
10/06/2016 Added by Sergey
MRI in St. Petersburg, USA
Great article. Thank you. MRI doctor.
business 0.3 MRI in St. Petersburg, USA 5.0 5.0 1 1 Excellent article.
Thank you. MRI doctor. MRI in St. Petersburg USA
Pain due to meningitis
The most characteristic sign of pathology is headache. It occurs in any form of meningitis and appears from the first days of the disease. Headaches can vary in nature, but, as a rule, patients complain that their entire head hurts. Also, attacks of nausea and vomiting are often observed against the background of headaches.
What kind of pain occurs?
The manifestation of pain directly depends on the localization of the area of brain damage, the nature of the occurrence of meningitis (viral or infectious, or as a consequence of the development of the disease due to narrowing of blood vessels and spinal disorders).
In all cases, the nature of the headache will be different. Pain depends on the location of the inflammation, its prevalence, and the degree of impact on brain function.
Headache with serous meningitis
With serous meningitis, moderate pain is observed throughout the skull. In this case, there is no fever or increase in body temperature. The patient also experiences chills, nausea and vomiting against the background of constant headaches. However, after vomiting the patient does not feel any relief.
How does a headache occur with purulent meningitis?
With this form of meningitis, the patient develops severe headaches that are bursting in nature. The pain either subsides or increases again. Characteristic symptoms in this case are nausea, vomiting, fever, and chills.
Pain from subarachnoid hemorrhage
In this situation, headaches are constant, that is, they do not subside either day or night, neither in summer nor in winter. Headache is characterized by intense, sharp and acute manifestation.
How does a headache occur with tuberculous meningitis?
This is the weakest form of meningitis in its manifestations, characterized by an increasing nature of the manifestation of symptoms. Patients experience constant weakness, increased sweating, and depression. Nausea and vomiting occur very rarely.
With any form of meningitis, headaches lead to blurred vision. Patients often develop intolerance to loud sounds and photophobia. The pain intensifies several times when pressing on the area of the temples or eyes.
Causes of secondary headaches
Causes of secondary headaches (associated with illness or injury) include:
- arterial hypertension;
- cerebrovascular diseases (ischemic stroke, hemorrhagic stroke, cerebral aneurysm);
- infectious diseases (meningitis, encephalitis, otitis media, sinusitis);
- hydrocephalus;
- idiopathic intracranial hypertension;
- head injuries;
- uncontrolled (excessive) use of medications;
- benign and malignant brain tumors.
Diagnosis of meningitis
The diagnosis of meningitis can be made based on the results of additional studies - laboratory and instrumental:
- detailed blood test;
- fundus examination;
- X-ray examination of the skull;
- heart electrocardiograms;
- electroencephalography;
- computer and magnetic resonance imaging.
To confirm the diagnosis of meningitis, doctors use bacteriological examination of mucus from the nasopharynx and cerebrospinal fluid. During bacterioscopic examination of cerebrospinal fluid, smears are stained with Gram or methylene blue. To exclude fungal meningitis, the specimen containing cerebrospinal fluid is stained with ink. Laboratory assistants isolate a pure culture on media with the addition of normal horse serum or cattle serum and identify it by biochemical activity and antigenic structure.
In case of viral meningitis, in preparations prepared with Gram staining and ink, it is impossible to identify the causative agent of the infection. Cultivation of bacteria and fungi also gives negative results. By culturing cellular material with standard laboratory cell lines, a pathogen serologically identical to the measles virus can be isolated. Rubella virus is isolated using the co-cultivation method.
To identify oligoclonal immunoglobulins, the method of agarose gel electrophoresis or isoelectric focusing of cerebrospinal fluid gamma globulins is used. Immunoglobulins appear in a number of viral infections. As a result of immunological studies, viral antigens or antibodies are detected in the cerebrospinal fluid, and the nucleic acid of the virus is detected using the polymerase chain reaction method. The enzyme immunoassay method detects pathogen antigens in feces, urine or saliva. Express methods allow you to quickly and early determine the presence of the herpes simplex virus antigen in the cerebrospinal fluid and blood or the DNA of the virus (using the polymerase chain reaction method).
CSF cytosis in meningitis
Analysis of cerebrospinal fluid allows not only to confirm the diagnosis, but also to differentiate purulent and serous meningitis, identify the causative agent of the disease, determine the degree of intoxication, and also makes it possible to monitor the effectiveness of treatment.
Bacteriological examination of cerebrospinal fluid in the case of tuberculous meningitis may give a false negative result. Detection of tubercle bacilli in the cerebrospinal fluid depends on the thoroughness of the research. At the Yusupov Hospital, all diagnostic procedures are performed using modern medical equipment and the use of new drugs and techniques. The results of studies conducted at the Yusupov Hospital are reliable and as informative as possible.
How is meningitis treated?
At the Yusupov Hospital, patients can receive a full range of medical services for the detection and treatment of meningitis, rehabilitation after illness and prevention. Patients with meningitis can contact the neurologist clinic of the Yusupov Hospital every day for 24 hours to receive emergency care.
When patients are admitted to the Yusupov Hospital, a comprehensive diagnosis is carried out, including a number of examinations to identify the causes of meningitis, collection of complaints and symptoms. Patients with meningitis need inpatient treatment, so the Yusupov Hospital has created comfortable living conditions and ensures interaction with qualified personnel.
Consequences of meningitis
Since men are less likely to consult a doctor in a timely manner and more often than women suffer from cerebrospinal meningitis, they often develop complications during the illness. Mild complications include headaches when the weather changes or overwork, slight decreases in hearing, concentration, and memory. Depending on the severity of meningitis and the timeliness of seeking medical attention, the following complications may develop:
- a sharp decrease in visual acuity;
- stuttering;
- strabismus;
- significant hearing loss;
- decreased intelligence;
- dropsy of the brain;
- epilepsy;
- mental disorder;
- development of schizophrenia;
- dementia.
The patient may fall into a coma, he may develop paralysis, and with complicated meningitis, death is possible.
The Yusupov Hospital effectively diagnoses the disease. The patient undergoes examination at the hospital's diagnostic center, which is equipped with modern equipment from leading global manufacturers. You can make an appointment with a doctor by calling the Yusupov Hospital.
Bacterial infections
A huge number of pathogens related to bacterial infections can affect the brain. Diseases such as meningitis, encephalitis or brain abscess may well be caused by such “ordinary” pathogens as pneumococcus, staphylococcus, and enterobacteria. But this can only happen if:
- damage to the bones of the skull, with disruption of the integrity of the membranes of the brain;
- introduction of pathogens during neurosurgical operations;
- the presence of a purulent focus in the body and weakened immunity.
However, with other pathogens the situation is different.
Meningococcal infection is a traditional neuroinfection that affects the brain. The peak incidence is observed in the autumn-winter period, when the immune system is reduced due to frequent hypothermia and lack of vitamins. If the immune system is normal, then you will limit yourself to ordinary nasopharyngitis; otherwise, the likelihood of getting meningitis or meningoencephalitis increases.
Symptoms of meningococcal infection
- fever,
- increase in body temperature to 39-40° C.
- chills,
- headache
- weakness
- neck muscle tension
- nausea,
- vomit,
specific symptoms
- A red-violet rash protruding above the surface of the skin, the elements of which resemble a star in shape
- The disease begins very acutely (often you can specify a specific time (hour) when the person fell ill)
- Treatment must begin within 24 hours while the person is conscious, otherwise he may fall into a coma.
Mycobacterium tuberculosis, among other things, can also affect the brain. Children, elderly people and people suffering from immunodeficiency are more often affected.
The symptoms of the onset of the disease are not clearly expressed, most often it is general weakness, malaise, lack of appetite, headache and irritability, body temperature is subfebrile (the temperature rises over a long period of time within 37.1 - 38°C.). Subsequently, “usual” meningeal symptoms appear.
Afterwards, neurological disorders appear - paresis and paralysis of the facial nerve, oculomotor muscles, dizziness. Mental disorders occur against the background of neurological disorders.
Neurosyphilis, now almost never occurs, but before the discovery of penicillin it formed the basis of the work of neurologists. Neurosyphilis comes in several types:
- Asymptomatic, occurs without any special symptoms, the disease can only be detected by testing.
- Meningitis - often appears during the first year of the disease, manifested by disturbances in the functioning of cranial nerves and increased intracranial pressure (ICP).
- Cerebrovascular - occurs mainly in the 2-5th year of the disease and can lead to a stroke or transform into tabes dorsalis or progressive paralysis.
- Progressive paralysis is a disease that was also called “crazy paralysis.” Occurs 15-20 years after infection and first manifests itself with mental symptoms, then muscle paralysis occurs and progresses, which ultimately leads to death.
- Congenital, which, strictly speaking, affects the entire body and is characterized by multiple defects in the development of the child.
- Gumma of the brain - manifests itself as a space-occupying formation. Symptoms include increased ICP and focal symptoms, depending on the location of the gumma.
An unpleasant feature of the disease is its difficult diagnosis.