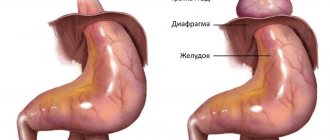
Hiatal hernia (HH) - symptoms and treatment
To diagnose hiatal hernia, in addition to detailed questioning of the patient, almost all research methods used in gastroenterology are used. Mandatory diagnostic methods include:
- clinical and radiological examination;
- fibroesophagogastroduodenoscopy (FEGDS);
- esophagotonometry;
- pH-metry of the esophagus and stomach;
- Ultrasound of the abdominal cavity.[12][158]
The leading instrumental methods are considered to be X-ray diagnostics and FEGDS.[8][16]
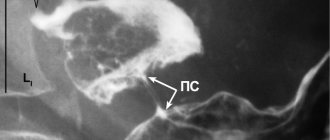
X-ray diagnostics
Thanks to the X-ray diagnostic method, fundamental research has been carried out on hiatal hernias, classifications have been developed, various forms of this pathology have been studied, and a number of indications and contraindications for various types of treatment of hiatal hernias have been developed.
The modern full name is “Polypositional X-ray diagnostic examination of the esophagus, stomach and duodenum using a liquid suspension of barium sulfate on a troscope.”
This X-ray examination allows you to reliably diagnose various forms of hiatal hernia, including “small” esophageal hernias, identify cardia insufficiency, gastroesophageal reflux, reflux esophagitis, and exclude cardia insufficiency associated with impaired passage of food in the underlying sections of the gastrointestinal tract.
Endoscopic esophagogastroduodenoscopy
In the middle of the 20th century, the latest technologies in endoscopy were developed and widely introduced into clinical practice. They have made it possible to significantly expand the possibilities for diagnosing gastroenterological diseases.
The peculiarity of endoscopic esophagogastroduodenoscopy is:
- the use of flexible fiber optics and the creation of endoscopic devices - fiber gastroscopes;
- high resolution of these devices with the ability to conduct research while visualizing images on the monitor;
- minimally invasive endoscopic diagnostics;
- minimal percentage of complications that arise;
- no need for special preparation of the patient before the start of endoscopic examinations;
- outpatient nature of endoscopic diagnostic methods.
All this allows us to recommend this diagnostic method not only to patients, but also to the population as a whole for medical examination and detection of the disease in the early stages.
Of course, endoscopic diagnosis of hiatal hernia is not an easy procedure, but FEGDS doctors consider it as a screening method indicated for all patients, including people with minimal symptoms of gastroesophageal reflux, dyspepsia or dysphagia (digestive or swallowing disorders), as well as anyone who suffers from digestive diseases. tract.
The main direct and indirect symptoms of hiatal hernia, usually manifested during FEGDS, include:
- reduced distance from the anterior incisors to the cardia;
- reduced length of the abdominal esophagus;
- hernial cavity;
- “second entrance” to the stomach;
- gaping (opening) of the cardia or its incomplete closure;
- prolapse (protrusion) of the gastric mucosa into the esophagus;
- reflux (reverse flow) of stomach contents into the esophagus;
- segmental dilation (expansion) of the esophagus in the area of the ninth segment;
- absent, poorly visualized or blurred Z-line;
- flattened fold of the cardioesophageal junction detected during inversion examination of the cardia;
- a smoothed angle of His, also detected during inversion examination of the cardia.
Most of the listed endoscopic symptoms of the hiatal hernia can be detected through video monitoring during FEGDS, which helps to establish an accurate diagnosis.
1st degree hiatus hernia
Alexander
June 26, 2021
Good afternoon, about a year ago, based on the results of gastroscopy, reflux esophagitis 0-1 according to Savary Miller was diagnosed against the background of a sliding hiatal hernia of the 1st degree. There was no heartburn, I was then treated for erosive gastritis, and against the background of a control FGD this was an accidental finding. Then I had a gastroscopy at the sanatorium since it was part of the check-up, the diagnosis was similar, only there was a scarlet erosion in the esophagus, and about 3-4 months ago I did another FGDS with the same doctor as the first time and the diagnosis was the same - reflux esophagitis 0-1 according to Savary Miller against the background of a sliding hiatal hernia of the 1st degree, superficial focal non-atrophic gastritis, superficial duodenitis. I almost never have heartburn, and I don’t seem to experience any discomfort either. But literally a month ago, problems with cardiac activity began (although he abruptly stopped taking antidepressants a week before, prescribed for the treatment of an anxiety disorder). There were sensations of interruptions in the functioning of the heart, freezing, discomfort, pain in the left side of the chest, shoulder, and so on. Shortness of breath or something similar to it, maybe lack of air (akin to panic attacks) I donated blood and the leukocytes were elevated at 10.1, while the norm was 8.7; lymphocytes and eosinophils with monocytes were also slightly elevated. Holter recorded 563 supraventricular extrasystoles. The rest is normal. I also did an ECG 2 times, which was also normal. There was also an ecg with a stress test and it was negative. there was no ischemia. And I also took an ultrasound of the heart there without any pathologies at all and took a Velergometry test with exercise - no ischemia was recorded, only exercise tolerance was reduced. I consulted with 4-5 cardiologists in person and in absentia - they said that the heart is healthy, there is no cardiac pathology and that treatment is needed from a neurologist and psychotherapist. tachycardia, something like shortness of breath (although I’m not suffocating) I read somewhere in a couple of sources, plus one of the cardiologists told me that the hiatal hernia can provoke both tachycardia and extrasystole. The endoscopist who did the FGDS last time said that it does not require treatment since there is 1 wall. It is enough to drink Pariet a couple of times a year. And the gastroenterologist said about the same thing, she did not focus on the hernia. I would like to note that the diagnosis of hiatal hernia was made only by FGDS; I did not take an x-ray in the Trendelburg position. My question is, can a sliding hiatal hernia of stage 1 affect the heart and give similar symptoms? What kind of extrastresses did you have before, the tachycardia now, pain in the left side of the chest, in the shoulder, in the arm? And if so, how to treat stage 1 hiatal hernia in my case?
The question is closed
HHH 1 tbsp
Reviews
Those who are afraid of esophageal plastic surgery, do not be afraid, this will save the quality of your life! I would like to express my deepest gratitude to surgeons Alexey Anatolyevich Nitkin and Dmitry Valerievich Ruchkin! Thanks to their professionalism, I live a full life. They performed an esophageal plastic surgery, removing it and replacing it with a gastric tube. I am writing half a year after the operation so that everyone who doubts the effect of this operation can calmly exhale and decide to have it. Since 2014, I began to develop achalasia cardia. The diagnosis was made 4 years later, when she reached the second stage. Moreover, the Internet helped me make the diagnosis, not doctors. Then I didn’t know anything about thoracic surgeons and went to gastroenterologists. I was prescribed pills and “not to be nervous.” And the condition gradually worsened. Food did not pass well, at first water helped, but over time, water stopped passing through the spasmodic cardia. When eating, there was a pain behind the sternum, as if a stake had been stuck into it. Dry food and carbonated drinks were the first to be banned, and then soups stopped passing, accumulating in the esophagus. In 2021, about 20% of food ended up in the stomach, everything else was vomited, because the bursting pain in the esophagus left no choice. The worst thing was at night, when food and water remaining in the esophagus entered the respiratory tract and I woke up coughing and choking. Pneumonia was also ahead of me. There was no choice left and I turned to thoracic surgeons in Tula. In 2019, I was operated on (a fundoplication was performed through laparoscopy (the esophagus was cut to relax the cardia and covered with a cuff from the tightened edge of the stomach). I did not feel the effect, because a week later I was brought by ambulance with suspected peritonitis. They did an emergency laparotomy (cut abdominal wall along the entire length), washed, but the cause of peritonitis was not found. They stitched it up. And two days later a perforated ulcer opened near the operation site and a second peritonitis began. The second emergency operation, and now the cuff was made 360 degrees... and most likely too tight. Recovery was difficult. After a month and a half, I was able to be discharged, but the expected effect from the operations did not occur. It was as if they had never been done. Then I did bougienage, but it did not help, since the cuff was in the way. Fear of new operations and Covid They didn’t let me go further. Achalasia continued to progress and a fear of eating appeared, I practically stopped sleeping, even a sitting position did not save me from the reflux of food into the respiratory tract. I was rapidly losing weight (from 67 to 43 kg with a height of 175 cm). I was simply dying from hunger and lack of sleep. I was very lucky that in August 2021, when the Tula hospital was repurposed as a Covid hospital, I was sent to Moscow to the Vishnevsky Institute. And what was my surprise to learn that there is a department of reconstructive surgery (a place where other people's unsuccessful operations are redone). The service is at a very high level, the surgeons answer all questions and are very competent. I was given a quota very quickly and underwent surgery. ON OMS! Despite the fact that the operation lasted 6 hours, it was only done laparotomically and they cut into a place that had been sewn up more than once, I was discharged within a week! A few days of obligatory hunger strike, pureed food and then a full life! Within a couple of weeks I started eating everything, absolutely everything! Yes, another scar was added near the jugular cavity. Below it is now the junction of the remainder of the esophagus and the gastric tube (anastamosis). It is he who always causes concern among surgeons and is carefully monitored. Initially, I was scared by the fact that after the operation I would not have a stomach, because they would cut it open and sew a tube out of it, which would become my new esophagus. There were a thousand questions: how could it work like the esophagus and push food through? Will gastric juice be released in the tube? How will food be digested if it has nowhere to be deposited as before? If there is no “valve” (cardia), I will continue to choke, because nothing will stop the food when I lie down? Will I suffer from heartburn? But I also understood that I didn’t have many options for a full life. And I didn’t regret agreeing to the operation! You are in the hands of the best specialists in this field! I can’t speak for other surgeons, but Nitkin A.A. and Ruchkin D.V. worthy of the highest praise for their professionalism! I received clear answers to all my questions and was always surrounded by attention, almost 24 hours a day. One got the feeling that Nitkin A.A. lives in the workplace. And after discharge he was always in touch and continued to advise about stitches and well-being. And now I’ll dispel your fears, because I’m specifically writing a review six months later: I don’t feel any difference in the passage of food through the gastric tube, it feels like my esophagus is there as before, nothing gets stuck there. I calmly drink soda, eat dry food and sometimes on the run (I hope my surgeons don’t read this :)). I did not have any problems with the pancreas, liver or stool due to the absence of a depot in the form of a stomach. Everything is within the normal range. I sleep horizontally, sometimes without a pillow, even on my stomach and immediately after eating (although the recommendations were to eat a couple of hours before bed, not later) and nothing causes a cough, there is no reverse casting! For me this is not at all explainable, but it’s a fact! No heartburn or stomach acid where it is not needed. Yes, I can’t eat more than 200 grams of food at a time, or rather I can, but after that I feel like I’ve been severely overeating and feel discomfort for a couple of hours. Now I know exactly what “fed up” means. Exercising immediately after eating is also not comfortable, but this is nitpicking and generally not correct))). Belching air after every meal is a little annoying, but I don’t deny myself anything. The weight is restored slowly, but this is good for the girl))). Oh yes, I got a neat cosmetic stitch! But unfortunately my body decided to make the scar not so beautiful. But these are all trifles! The main thing is that Nitkin A.A. and Ruchkin D.V. with their golden hands (and telling names) they gave me a full life! If you still doubt whether it’s worth it, then I’ll tell you it’s definitely WORTH IT!
I would like to express my deepest gratitude to surgeons Alexey Anatolyevich Nitkin and Dmitry Valerievich Ruchkin! Thanks to their professionalism, I live a full life. They performed an esophageal plastic surgery, removing it and replacing it with a gastric tube. I am writing half a year after the operation so that everyone who doubts the effect of this operation can calmly exhale and decide to have it. Since 2014, I began to develop achalasia cardia. The diagnosis was made 4 years later, when she reached the second stage. Moreover, the Internet helped me make the diagnosis, not doctors. Then I didn’t know anything about thoracic surgeons and went to gastroenterologists. I was prescribed pills and “not to be nervous.” And the condition gradually worsened. Food did not pass well, at first water helped, but over time, water stopped passing through the spasmodic cardia. When eating, there was a pain behind the sternum, as if a stake had been stuck into it. Dry food and carbonated drinks were the first to be banned, and then soups stopped passing, accumulating in the esophagus. In 2021, about 20% of food ended up in the stomach, everything else was vomited, because the bursting pain in the esophagus left no choice. The worst thing was at night, when food and water remaining in the esophagus entered the respiratory tract and I woke up coughing and choking. Pneumonia was also ahead of me. There was no choice left and I turned to thoracic surgeons in Tula. In 2019, I was operated on (a fundoplication was performed through laparoscopy (the esophagus was cut to relax the cardia and covered with a cuff from the tightened edge of the stomach). I did not feel the effect, because a week later I was brought by ambulance with suspected peritonitis. They did an emergency laparotomy (cut abdominal wall along the entire length), washed, but the cause of peritonitis was not found. They stitched it up. And two days later a perforated ulcer opened near the operation site and a second peritonitis began. The second emergency operation, and now the cuff was made 360 degrees... and most likely too tight. Recovery was difficult. After a month and a half, I was able to be discharged, but the expected effect from the operations did not occur. It was as if they had never been done. Then I did bougienage, but it did not help, since the cuff was in the way. Fear of new operations and Covid They didn’t let me go further. Achalasia continued to progress and a fear of eating appeared, I practically stopped sleeping, even a sitting position did not save me from the reflux of food into the respiratory tract. I was rapidly losing weight (from 67 to 43 kg with a height of 175 cm). I was simply dying from hunger and lack of sleep. I was very lucky that in August 2021, when the Tula hospital was repurposed as a Covid hospital, I was sent to Moscow to the Vishnevsky Institute. And what was my surprise to learn that there is a department of reconstructive surgery (a place where other people's unsuccessful operations are redone). The service is at a very high level, the surgeons answer all questions and are very competent. I was given a quota very quickly and underwent surgery. ON OMS! Despite the fact that the operation lasted 6 hours, it was only done laparotomically and they cut into a place that had been sewn up more than once, I was discharged within a week! A few days of obligatory hunger strike, pureed food and then a full life! Within a couple of weeks I started eating everything, absolutely everything! Yes, another scar was added near the jugular cavity. Below it is now the junction of the remainder of the esophagus and the gastric tube (anastamosis). It is he who always causes concern among surgeons and is carefully monitored. Initially, I was scared by the fact that after the operation I would not have a stomach, because they would cut it open and sew a tube out of it, which would become my new esophagus. There were a thousand questions: how could it work like the esophagus and push food through? Will gastric juice be released in the tube? How will food be digested if it has nowhere to be deposited as before? If there is no “valve” (cardia), I will continue to choke, because nothing will stop the food when I lie down? Will I suffer from heartburn? But I also understood that I didn’t have many options for a full life. And I didn’t regret agreeing to the operation! You are in the hands of the best specialists in this field! I can’t speak for other surgeons, but Nitkin A.A. and Ruchkin D.V. worthy of the highest praise for their professionalism! I received clear answers to all my questions and was always surrounded by attention, almost 24 hours a day. One got the feeling that Nitkin A.A. lives in the workplace. And after discharge he was always in touch and continued to advise about stitches and well-being. And now I’ll dispel your fears, because I’m specifically writing a review six months later: I don’t feel any difference in the passage of food through the gastric tube, it feels like my esophagus is there as before, nothing gets stuck there. I calmly drink soda, eat dry food and sometimes on the run (I hope my surgeons don’t read this :)). I did not have any problems with the pancreas, liver or stool due to the absence of a depot in the form of a stomach. Everything is within the normal range. I sleep horizontally, sometimes without a pillow, even on my stomach and immediately after eating (although the recommendations were to eat a couple of hours before bed, not later) and nothing causes a cough, there is no reverse casting! For me this is not at all explainable, but it’s a fact! No heartburn or stomach acid where it is not needed. Yes, I can’t eat more than 200 grams of food at a time, or rather I can, but after that I feel like I’ve been severely overeating and feel discomfort for a couple of hours. Now I know exactly what “fed up” means. Exercising immediately after eating is also not comfortable, but this is nitpicking and generally not correct))). Belching air after every meal is a little annoying, but I don’t deny myself anything. The weight is restored slowly, but this is good for the girl))). Oh yes, I got a neat cosmetic stitch! But unfortunately my body decided to make the scar not so beautiful. But these are all trifles! The main thing is that Nitkin A.A. and Ruchkin D.V. with their golden hands (and telling names) they gave me a full life! If you still doubt whether it’s worth it, then I’ll tell you it’s definitely WORTH IT!
Yulia Aleksandrovna Ch., 36 years old, Tula