The body's digestive system is a complex mechanism. Its work is regulated by several sphincters. This is the name given to the valves that are responsible for the passage of food from one compartment to another. If one of them malfunctions, all organs associated with it suffer. Usually, the pathologies of most sphincters are almost invisible outwardly, only insufficiency of the gastric cardia causes pronounced symptoms. After all, it is this valve that blocks the flow of stomach contents into the esophagus and prevents belching, heartburn or vomiting. If this pathology is left untreated, serious damage to the esophageal mucosa from gastric juice develops.
The concept of achalasia cardia, the prevalence of the disease
The frequency of this disease in European countries is 1 per 100 thousand people, in the structure of all diseases of the esophagus it accounts for from 2 to 25%.
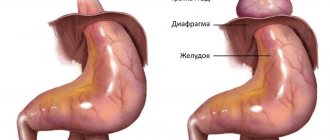
Achalasia cardia is the inability of the esophageal outlet to relax as a result of the congenital absence of specific nerve fibers in the intermuscular layer. With achalasia cardia, the esophagus becomes as if deprived of innervation in a small area. Against this background, its increased sensitivity to gastrin and cholinomimetics (local regulation hormones) is formed. Due to this, over time, a place of persistent narrowing of the esophagus forms before the entrance to the stomach. With this disease, food enters the stomach not through a reflex (during swallowing), but through mechanical opening of the cardia against the background of hydrostatic pressure exerted by a column of liquid food that has accumulated in the esophagus by this time. At first, the muscle strength of the upper esophagus copes with pushing food through this narrowed area, and then the muscle weakens, and the esophagus stretches, taking on an S-shape.
Classification of achalasia cardia
There are four stages in the development of the disease:
- The first (functional) stage
- there is a temporary disruption of the passage of food through the cardiac sphincter due to the cessation of its relaxation during the process of swallowing - The second stage
is accompanied by moderate dilatation of the esophageal wall - The third stage
is characterized by persistent suprastenotic dilatation of the esophagus and the presence of persistent narrowing in the lower part of the esophagus due to the formation of scar changes - The fourth stage
is characterized by a pronounced clinical picture, which develops against the background of an S-shaped dilatation of the esophagus and complications in the form of esophagitis, periesophagitis, fibrous mediastinitis, chronic bronchitis, chronic pneumonia and atelectasis in the lungs (against the background of constant night reflux of esophageal contents and aspiration of food into the respiratory tract mass)
Folk remedies for pathology
To tone the cardiac sphincter, drinks containing caffeine are completely excluded from the diet. However, herbal infusions from medicinal plants valerian and St. John's wort are an alternative. Traditional medicine therapy is relevant only in the initial stages of the disease, when there are no complications, or during remission. In the morning on an empty stomach, as well as before each meal, it is recommended to drink a glass of warm water.
In order to achieve a therapeutic effect, it is useful to use the following recommendations:
- Plantain juice helps normalize digestion.
- Between main meals, it is useful to drink an infusion made from calamus root. To do this, 5 grams of raw materials are poured into a glass of boiling water.
- Three times during the day, drink a medicinal infusion for the stomach, which is prepared from peppermint, plantain, St. John's wort, chamomile and yarrow.
- Dandelion flowers, which are covered with sugar and ground and then decanted, have a high therapeutic effect. The resulting syrup is diluted with water.
Cumin is an indispensable remedy for restoring and maintaining proper functioning of the stomach. It can be consumed as a decoction or crushed and added to breakfast cereals.
Symptoms and clinical picture of achalasia cardia
The first complaints of patients are difficulty swallowing (dysphagia), a lump in the throat, followed by pain in the chest, regurgitation of food, and cough.
The development of achalasia cardia occurs rather slowly, but the severity of the main symptoms of the disease is constantly increasing.
Dysphagia occurs when consuming a wide variety of foods, both liquid and solid, usually within a few seconds of the start of the act of swallowing. In this case, food is retained not in the throat, but in the chest, so the sensations are localized retrosternally.
Regurgitation
- reverse reflux of food from the lower to the overlying sections (into the oral cavity). Increased casting is observed when the torso is tilted forward, after a heavy meal, and also at night, when the patient assumes a horizontal position. In this case, food debris often gets into the respiratory tract with the development of corresponding complications and clinical manifestations.
Odynophagy
- this is pain in the chest area associated mainly with spasm of the smooth muscles of the esophagus and the overflow of its lumen with food masses.
With the development of the fourth stage, stagnant symptoms appear due to the prolonged presence of swallowed food in the esophagus (bad breath, nausea, rotten belching). Against this background, due to the formation of a large amount of lactic acid, heartburn and inflammation of the walls of the esophagus occur - esophagitis, which can be erosive and ulcerative.
To identify achalasia cardia and choose the correct surgical treatment tactics, you must send me a complete description of gastroscopy, X-ray of the esophagus and stomach with barium, preferably an ultrasound of the abdominal organs, to my personal email address, you must indicate age and main complaints. In rare cases, if there is a discrepancy between complaints, X-ray data and FGS, it is necessary to perform esophageal manometry. Then I will be able to give a more accurate answer to your situation.
Pyloric insufficiency
The pylorus of the stomach is the site of its transition to the duodenum. Another name for the organ is sphincter (pylorus, valve). The main function of the pylorus is to control the passage of partially digested food from the stomach into the small intestine. Normally, the muscle is constantly in a closed state, from time to time passing small portions of semi-digested food further along the digestive tract. With insufficiency of the pylorus of the stomach, this process is disrupted, so the pathology requires complex treatment.
Diagnosis of achalasia cardia
Puchkov K.V., Ivanov V.V. and others. Technology of dosed ligating electrothermal effects at the stages of laparoscopic operations: monograph. - M.: ID MEDPRACTIKA, 2005. - 176 p.
Puchkov K.V., Bakov V.S., Ivanov V.V. Simultaneous laparoscopic surgical interventions in surgery and gynecology: Monograph. - M.: ID MEDPRACTIKA, 2005. - 168 p.
Diagnosis of this disease is based on data obtained during a survey (the patient presents the above complaints), physical examination of the patient, as well as the results of instrumental research.
The main radiological sign of achalasia cardia is a narrowed distal section of the esophagus, which has smooth, clear contours, and an expanded section of the digestive canal located above it. In this case, the narrowed part is often located eccentrically and there is an overhang of the walls of the esophagus above it - a symptom of a “writer’s pen”.
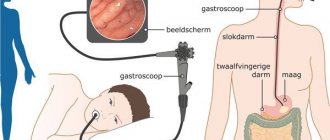
The fibroendoscopic method allows you to visually assess the condition of the terminal esophagus and gastroesophageal junction. In most cases, it is possible to pass the fiberscope through the narrowed part of the esophagus, which is more common with the functional nature of the changes, and speaks in favor of achalasia cardia.
Manometry of the esophagus makes it possible to objectively assess the motor activity of the organ and judge the quality of work of the upper and lower esophageal sphincters. Violations of the contractility of the esophagus and cardiac sphincter occur much earlier than the development of clinical symptoms of the disease, in connection with this, manometry becomes the main method of early diagnosis of the disease, when FGS and fluoroscopy do not yet have clear data for cardial achalasia.
Treatment of achalasia cardia. Drug therapy and cardiodilation.
It should be noted that pharmacotherapy (calcium channel blockers, nitrates, myotropic antispasmodics, anesthetics) is effective only in the first stage, in which mild and rare transient dysphagia is noted.
The generally accepted method of treatment is endoscopic bougienage of the esophagus, aimed at expanding the narrowed area, but, unfortunately, this occurs through tissue rupture, with the formation of rough scars in this area, which in the future only worsens the situation. The effect of bougienage of the esophagus is short-lived, repeated manipulations are required and after 4-5 procedures relief does not occur. In this situation, an operation is proposed - esophagomyotomy (dissection of part of the wall of the esophagus to the submucosal layer without opening the lumen of the organ), which allows you to restore normal swallowing and return the patient to a normal lifestyle.
At the same time, the endoscopic dilatation technique can be useful for the treatment of patients in the older age group and people with relapse of achalasia cardia who have previously undergone surgery. That is, for those patients for whom, due to concomitant diseases, surgical intervention is contraindicated or its implementation is technically extremely difficult.
Also, one of the minimally invasive methods of treating achalasia cardia is endoscopic intrasphincteric injection of botulinum toxin A. It is considered as a fairly effective alternative option for people who have absolute contraindications to endoscopic hydro- or pneumatic cardiodilation and surgical intervention, especially when it comes to patients in the older age group , about the presence of pronounced, severe concomitant pathology of the cardiovascular and bronchopulmonary systems. Treatment with botulinum toxin is safe, but it should be borne in mind that the effects on the lower esophageal sphincter often last only 2-3 months, and therefore additional repeated administration of this drug may be required.
Early surgery gives very good results, since in the narrowed area there are no scars from previous cardiodilation, and the muscle strength of the esophageal wall has not yet been depleted. But, even with a distended esophagus, good results are possible when using an adequate laparoscopic method.
Very important!
A feature of my approach to choosing treatment tactics for patients with achalasia cardia is the earlier determination of indications for surgical treatment using the laparoscopic method (through several punctures of the abdominal wall), without waiting for complications to develop and without wasting time on useless conservative treatment methods.
How does pyloric insufficiency manifest?
The larger the lumen in the pylorus, the more pronounced the signs of the disease are:
- pain a little to the right and below the solar plexus;
- after eating, nausea and vomiting begin;
- the appearance of plaque on the tongue (usually yellow);
- belching with a bitter aftertaste;
- heaviness and discomfort in the epigastric region.
The symptoms are similar to other diseases of the digestive system. In addition to insufficiency, the pylorus of the stomach can be susceptible to spasms, ulcers and erosions, the appearance of polyps and other pathologies. For this reason, each patient is required to undergo examination and consult a gastroenterologist.
Surgical methods for treating achalasia cardia
Puchkov K.V., Rodichenko D.S. Manual suture in endoscopic surgery: monograph. - M.: MEDPRACTIKA, 2004. - 140 p.
Of the many surgical methods proposed for the treatment of esophageal achalasia, currently only those interventions based on extramucosal cardiomyotomy are mainly performed. One of the main ones is the method of extramucosal cardioplasty, performed according to Heller (E. Heller). The essence of the method is a longitudinal section of the muscular lining of the distal esophagus along its anterior wall for eight to ten centimeters. In this case, the myotomy should cover not only the area of narrowing and the cardiac part of the stomach, but also a partially expanded area of the esophagus. In this case, the edges of the dissected muscular membrane diverge in opposite directions, as a result, the underlying intact mucous membrane begins to bulge into the resulting defect.
According to the literature, good results after this type of surgery are observed in up to 90% of cases. The disadvantages of this technique are associated with leaving the esophageal mucosa unprotected over a large area (8-10 cm x 1 cm). Therefore, in places where the muscular lining of the esophagus is cut, diverticula and scars that deform the cardia can form, causing a relapse of the disease.
Mortality after Heller surgery averages about 1.5% (a number of authors give the figure 4%). The main cause of death is usually overlooked damage to the esophageal mucosa, which leads to mediastinitis (inflammation of the mediastinal tissue), pleurisy (inflammation of the pleura) and peritonitis (inflammation of the peritoneum). Trauma to the mucosa is observed in 6-10% of all operations, therefore, to prevent severe complications, it is extremely important to conduct a very thorough inspection of this area. If the surgeon discovers damage to the mucous membrane, it must be sutured. Also, unsatisfactory results are associated with the destruction of the cardinal sphincter and the development of peptic reflux esophagitis. And due to the possibility of closure and fusion of the dissected walls of the muscle layer, there is a recurrence of the disease, dysphagia and impaired emptying of the esophagus.
Very important!
To reduce mortality and the number of postoperative complications, it is necessary to cover the surgical defect of the esophageal wall with one’s own tissues, which is rarely performed by surgeons due to the technical complexity of this stage of the operation.
Today, there are a variety of ways to cover the mucous membrane. What can the omentum, the anterior wall of the stomach, and a section of the diaphragm be used for? It should be noted that options for closing the defect in the muscular lining of the esophagus with any synthetic materials are not advisable due to the development of bedsores in this place.
Very important!
To prevent the development of cardiac sphincter failure and reflux esophagitis, preserve the natural anatomical relationships of the esophagus, stomach and diaphragm as much as possible.
What is Helicobacter pylori?
This is a bacterium that affects the pylorus of the stomach and duodenum. The prevalence of this infection is very wide, almost 50% of the world's population is infected with the bacterium Helicobacter pylori (Helicobacter pylori, Helicobacter pylori infection, Helicobacter pylori).
Bacteria that can survive in the aggressive, acidic environment of the stomach have been known for more than 100 years, but it was only in the 1970s that the connection between these bacteria and gastritis was discovered. A more complete understanding of the influence of these microorganisms on gastrointestinal disease occurred already in the 1980s, when it was possible to isolate and cultivate a bacterium called Campylobacter pyloridis (Campelobacter pyloridis), after studying and final classification called Helicobacter pylori (Helicobacter pylori).
Helicobacter pylori is a spiral-shaped bacterium 3.5 microns long and 0.5 microns wide. In some cases, the microorganism acquires a coccoid shape.
Laparoscopy in the surgical treatment of achalasia cardia and its complications
Laparoscopic operations for diseases of the esophagus and stomach are distinguished by their delicacy and functionality. The enlarged image on the monitor allows you to perfectly visualize all the finest anatomical formations in this area - the vagus nerve, gastric vessels and fascial spaces for gentle surgery. Laparoscopic access allows to reduce the duration of the intervention, shortens the postoperative rehabilitation period and facilitates its course, and also helps to significantly reduce the number of complications and provides a good cosmetic effect.
We have improved the technique of laparoscopic surgery in the treatment of achalasia cardia, which can reduce the number of relapses to 0.2%, and the number of complications to 1%.
My tactics in approaching surgical treatment of patients with achalasia cardia are as follows:
- Earlier determination of indications for surgical treatment, without waiting for complications to develop and without wasting time on useless conservative treatment methods;
- Using only laparoscopic access for surgery - better visualization, less trauma, better cosmetic effect and faster recovery;
- Performing extramucosal cardioplasty with mandatory dissection of the muscle and scar layers at a distance of 8-10 cm, which ensures guaranteed elimination of stenosis;
- In order to prevent complications from the exposed mucous membrane, perform a thorough revision of this area, if necessary, suturing it and obligatory covering it with the anterior wall of the stomach;
- In order to prevent relapse of the disease (fusion of the dissected muscular membrane), cover this area with the anterior wall of the stomach, with mandatory suturing it along the entire perimeter of the mucosal defect using our own method, only with synthetic absorbable threads on an atraumatic needle;
- In order to prevent insufficiency of the cardinal sphincter (as a result of dissection of the muscle layer) and the development of peptic esophagitis, strengthening this area with the anterior wall of the stomach (fundoplication at 120 degrees);
- When isolating the esophagus and stomach, I use a modern device for dosed electrothermal tissue ligation “LigaSure” (USA), which makes it possible, without damaging the surrounding structures, to “weld” the vessels and with thin electrodes to dissect the muscular lining of the esophagus without damaging the mucous membrane;
- The technique I developed allows the transgastric tube not to be left after surgery (which greatly facilitates the postoperative period), and the patient to eat liquid food the next day.
You can watch videos of operations performed by me on the website “Video of operations of the best surgeons in the world.”
As a result of using our method, the vast majority of patients (97%) report good results. In this case, the positive effect is confirmed by data from control fibroesophagogastroduodenoscopy, X-ray examination and esophagomanometry. According to the results of manometric measurements in all operated patients, it was possible to achieve a decrease in the basal tone of the esophagus. In addition, there is a noticeable improvement in the contractile activity of the esophagus and an increase, although insignificant, in the length of the cardia due to the formation of a fundoplication cuff. According to the indicators obtained during 24-hour intraesophageal pH-metry, pathological gastroesophageal refluxes (reflux of stomach contents into the esophagus) after the Heller operation, supplemented by anterior esophageal fundoplication according to Dor in our modification, are recorded at the physiological level.
My experience includes more than 600 operations for hiatal hernia and reflux esophagitis and more than 100 operations for achalasia cardia. It is summarized in three monographs: “Hiatal hernia”, “Hand suture in endoscopic surgery” and “Technology of dosed ligating electrothermal effects at the stages of laparoscopic operations”, as well as in more than 60 scientific publications in various professional peer-reviewed scientific publications in Russia and abroad.
After the operation, 3-4 incisions 5-10 mm long remain on the skin of the abdomen. From the first day, patients begin to get out of bed, drink, and the next day take liquid warm food. Discharge from the hospital is carried out on days 1-3, depending on the severity of the disease. The patient can begin work in 2 - 3 weeks. A strict diet should be followed for one and a half to two months, a softer one - for six months. Further, as a rule, the patient leads a normal lifestyle - without medications or diet.
At the request of patients, the clinic can undergo a full examination before surgery to determine the optimal treatment tactics and choose the method of surgical intervention.
Help from therapeutic exercises
The muscular structures of the gastric cardia can be easily strengthened. For this purpose, specially designed breathing exercises are used. Particularly popular is Strelnikova’s gymnastic method, which involves performing training twice during the day: in the morning and in the evening before a meal, and also after an hour and a half after its end, for 1500 breaths. As a preventive measure, gymnastics is performed in the morning or evening period. Such breathing exercises help strengthen the body and improve the health of internal organs due to increased blood flow.
Questions most often asked by patients with achalasia cardia
What anesthesia do you use for laparoscopic treatment of achalasia cardia?
If you would like to learn in more detail about the methods of pain relief used in the surgical treatment of achalasia cardia, please carefully read the information posted on the website.
Is it necessary to somehow prepare for surgery for laparoscopic treatment of achalasia cardia?
If you are planning surgical treatment for achalasia cardia, I ask you to carefully study the preoperative preparation section.
Is it possible to simultaneously perform laparoscopic surgery for achalasia cardia and, for example, fibroids?
Minimally invasive surgery techniques allow two and sometimes three operations to be performed simultaneously during one anesthesia by a team of several surgeons. The issue of simultaneous operations is discussed in more detail in a special section of the site. Simultaneous performance of several surgical interventions will reduce the load on the body, reduce hospitalization time, and speed up the body’s recovery compared to performing several operations with an interval of 5-6 weeks.
Where can I undergo surgery for achalasia cardia?
I conduct the initial consultation with all patients in Moscow at the Swiss University Clinic. Get acquainted in more detail with my main clinical sites in Moscow and Switzerland.