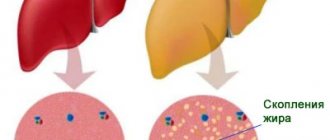
Spring rain. In a small bay, the little shells got wet through and through.
Buson
Leptospirosis is a zoonotic infection that occurs in humans in the form of an acute febrile illness with severe intoxication, damage to the kidneys, liver, central nervous system, and the development of hemorrhagic syndrome.
Leptospirosis was first described as an independent nosological form by the German scientist Weil in 1886 and the Russian scientist N.P. Vasiliev in 1888 under the name “infectious jaundice”. In 1907, Stimson discovered previously unknown microorganisms in the kidneys of patients who allegedly died of yellow fever and named them Spirochaeta interrogans. Japanese microbiologists under the leadership of Inada in 1916 isolated a spirochete from the blood of patients with jaundice, which was named Spirochaeta icterohaemorrhagiae. The name Leptospira to designate newly discovered microorganisms was proposed in 1917 by Noguchi. In 1985, WHO classified leptospirosis as one of the most important zoonotic diseases.
Despite numerous studies on leptospirosis, the use of modern methods of therapy, including extracorporeal detoxification methods, mortality in severe forms of icterohemorrhagic leptospirosis reaches 25–30%. In addition, convalescents may develop severe complications from the nervous system, eyes, kidneys and other organs. All of the above determines the relevance of the infection.
Etiology
The genus Leptospira of the Leptospiraceae family includes two species - pathogenic (L.interrogans) and saprophytic (L.biflexa). Leptospira are spiral-shaped, motile microorganisms 6–15 µm long, 0.1–0.25 µm thick, gram-negative, do not form spores or capsules. Leptospires are poorly stained with aniline dyes, and therefore in the living state they are usually studied in a dark field.
Leptospira are hydrobionts and quickly die when dried out. They are sensitive to sunlight, high temperatures, and disinfectant solutions. At a temperature of 55 °C, leptospira die in 25–30 minutes, and at a temperature of 100 °C - almost instantly. In open water bodies and moist soil, leptospira can remain viable from 2 weeks to 3 months or more, on food - from several hours to 30 days.
Leptospira in vitro is sensitive to many antibiotics: penicillin, ampicillin, tetracyclines, streptomycin, cefotaxime, erythromycin. However, the effects of antibiotics in vitro and in vivo are not always the same.
Pathogenic Leptospires are tissue parasites that affect the kidneys, liver, muscles, blood, and nervous tissue. Leptospires contain endotoxin, consisting of lipids, polysaccharides, polypeptides, which has pyrogenic, skin-necrotic and lethal properties.
Depending on the antigenic structure, there are more than 200 serological variants of pathogenic Leptospira, grouped into 25 serological groups. The most significant serogroups for human pathology are Icterohaemorrhagiae, Grippotyphosa, Pomona, Hebdomadis, and Canicola.
Diet
Diet 5th table
- Efficacy: therapeutic effect after 14 days
- Duration: from 3 months or more
- Cost of products: 1200 - 1350 rubles per week
Diet 7 table
- Efficacy: therapeutic effect after a week
- Terms: 1 month or more
- Cost of products: 1200-1300 rubles per week
In order for the treatment to be as effective as possible, the patient is recommended to adhere to the Table No. 5 , which has a beneficial effect on the liver. In case of kidney damage, it is recommended to follow the diet Table No. 7 .
The patient's diet should contain the following products:
- Fresh vegetable and fruit juices, compotes, rosehip decoction.
- Pumpkin, carrots.
- Oatmeal, buckwheat.
- Honey.
- Lean meat and fish.
- Vegetable soups.
- Egg white, one egg per day is allowed.
- Low-fat cottage cheese, yogurt
- Stale bread, oatmeal cookies.
The following should be excluded from the diet:
- Meat of young animals, fatty meat.
- Mushrooms.
- Fatty fish.
- Legumes.
- Salty foods.
- Alcohol.
- Canned food, smoked meats.
- Soda.
Epidemiology
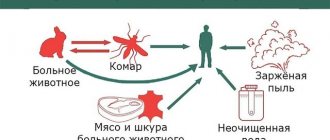
Leptospirosis is a zoonosis, a natural focal disease. The reservoir of pathogenic Leptospira in nature are mammals, amphibians, reptiles, and birds. The source of infection for humans can be many wild and farm animals that secrete Leptospira in the urine for a long time. Nowadays, natural foci of leptospirosis are affected by intensive human economic activity (water reclamation work, construction of large livestock complexes, etc.), which leads to changes in the ecology of rodents and can contribute to both the attenuation of the epizootic process in the foci and the emergence of new natural and also anthropurgic (economic) and mixed foci of leptospirosis. In anthropurgic foci, the source of infection is farm animals, rodents, and dogs. A person with leptospirosis is practically not contagious.
According to the epidemiological classification of L.V. Gromashevsky, leptospirosis, according to the transmission mechanism, is classified as an intestinal infection. However, by type of intestinal infection, leptospirosis is transmitted mainly among animals, and humans are more often infected when Leptospira penetrates through the outer integument (percutaneous mechanism of infection). Leptospirosis is transmitted by contact, water and food.
The main factor in the transmission of infection remains water contaminated with the urine of infected animals. Human infection with leptospirosis occurs when swimming in open freshwater reservoirs, during fishing, hunting, during various agricultural work, working in coal mines, drinking water from open reservoirs and wells, consuming infected products, and through direct contact with sick animals. Possible occupational infection.
People are highly susceptible to leptospirosis, but mostly young and middle-aged men are affected. Most cases of infection occur in the summer-autumn period. Along with sporadic morbidity, epidemic outbreaks are also recorded. After the illness, persistent serovar-specific immunity remains.
General information
Leptospirosis (Weil's disease or Weil-Vasiliev disease) is an acute disease of an infectious nature.
The causative agent of this disease is Leptospira bacteria. The infection affects the muscles, capillaries, central nervous system, liver and kidneys. The history of the disease dates back to 1883, when the disease was separately isolated from all jaundices. This disease was described in detail in 1886 by Adolf Weil. Most often, pathogens are found in humid regions and in areas where there are many swamps. Leptospirosis in animals leads to a mortality rate of about 90% due to this disease. It occurs most often in rats, dogs, pigs, cats, and cattle. It is these animals that are carriers of infection. A sick person suffers a severe illness, so he requires immediate hospitalization.
How leptospirosis manifests itself and which methods of treating the disease are the most effective will be discussed in this article.
Clinic
According to the International Statistical Classification of Diseases, diseases of leptospirosis etiology are grouped according to the etiological principle as follows:
A27.0 - icteric-hemorrhagic leptospirosis caused by L.Icteroha-emorrhagiae;
A27.8 - other forms;
A27.9 - unspecified leptospirosis.
According to the clinical and pathogenetic classification of leptospirosis, according to the degree of severity, there are 3 forms of the disease (mild, moderate and severe) and 2 main forms of the course (icteric and anicteric). In leptospirosis, the leading syndromes are distinguished: renal, hepatorenal, meningeal, hemorrhagic.
The course of leptospirosis can be without relapses and with relapses, without complications and with complications.
The course of leptospirosis is cyclical. There are 4 periods: incubation, initial (early, thermoalgic or bacteremic phase), height (period of organ damage, toxemic phase), convalescence.
The duration of the incubation period ranges from 2 to 30 days (usually 7–14).
The initial period of leptospirosis lasts 3–7 days. The disease, as a rule, begins acutely with chills and a sharp increase in body temperature to 39–40 °C. Patients often name not only the day, but also the hour of onset of the disease. On days 1–2 of illness, regardless of the Leptospira serogroup, patients complain of headache, chills, muscle and joint pain, general weakness, and nausea. Injection of scleral vessels and tachycardia are clearly visible.
Fever is constant or remitting, lasting from 3 to 12 days. Body temperature decreases critically or accelerated lysis. After a period of apyrexia lasting from 1 to 14 days, repeated feverish waves are possible (from 1 to 5). Normalization of temperature during leptospirosis is not always a favorable symptom. In severe cases of the disease, a decrease in body temperature, as a rule, by the 4th–5th day coincides with a significant deterioration in condition associated with the appearance of organ pathology. In severe cases of leptospirosis, prolonged low-grade fever may occur.
Muscle pain is one of the most characteristic symptoms of the initial period of leptospirosis. Muscle pain occurs at rest, intensifies with movement and palpation of muscles, and can persist until the 10th day of illness. The most pronounced pain is in the calf and lumbar muscles (false Pasternatsky sign or Kokovin sign). Less intense pain is observed in the muscles of the neck, back, and abdomen. The intensity of muscle pain in the initial period of leptospirosis corresponds to the severity of the disease. Muscle pain is more pronounced in severe forms of leptospirosis and hemorrhagic syndrome. Massive muscle necrosis may be one of the causes of subsequent kidney damage. In some cases, muscle pain can lead to diagnostic errors. For example, intense pain in the abdominal muscles can mimic an “acute abdomen.”
The initial period of leptospirosis is characterized by facial hyperemia and injection of scleral vessels. Symptoms such as enanthema on the oral mucosa, erythematous or polymorphic skin rash, herpetic eruptions on the lips are usually less common and do not depend on the severity of the disease.
Sometimes in the initial period of leptospirosis, peripheral lymph nodes become enlarged. Catarrhal phenomena are almost completely absent.
Such symptoms of intoxication, which constantly occur in the initial period of leptospirosis, such as chills, headache, general weakness, nausea, tachycardia, do not depend on the severity of the patient’s condition. However, severe headache combined with weakness, lethargy, insomnia, and vomiting is characteristic of a severe form of the disease.
The clinical picture of leptospirosis during the period of its peak (organ damage) is represented by large polymorphism, which is associated with the peculiarities of the pathogenesis of this infection. During this period, from the 3rd to 7th day of illness, symptoms of damage to the liver, kidneys, lungs, cardiovascular and central nervous systems, signs of generalized capillarotoxicosis and disorders in the hemostatic system are revealed. The polymorphism of the clinical picture creates difficulties in diagnosis, assessing the severity of the patient’s condition and predicting the outcome of the disease.
The most obvious symptom of liver damage due to leptospirosis is jaundice. In many cases, it is jaundice that allows the doctor to suspect leptospirosis. Based on this feature, icteric and anicteric clinical forms are distinguished. Jaundice can be observed in patients regardless of the Leptospira serogroup that caused the disease. However, if with leptospirosis associated with L. Pomona and L. Grippotyphosa, icteric forms account for up to 9%, then with leptospirosis caused by L. Icterohaemorrhagiae and L. Canicola - up to 80%. Jaundice in most cases appears on the 4th–6th day of illness. Leptospirosis is characterized by a short pre-icteric period. In severe cases of leptospirosis, jaundice may appear as early as the 2nd or 3rd day of illness. The severity of jaundice varies widely. In some cases, it may be limited to light coloring of the sclera, visible mucous membranes, and skin, which disappears within 1 week; and in others the jaundice is bright with a saffron-red tint and lasts for several weeks. Slight itching of the skin may occur. The urine of patients becomes dark. Complete discoloration of stool is rare, but hypocholia is present in most patients. The intensity of jaundice in most cases corresponds to the severity of lepto-spirosis. Hyperbilirubinemia is associated with increased levels of both conjugated and free bilirubin, but conjugated bilirubin increases to a greater extent. An increase in the level of total blood bilirubin above 200 µmol/l is considered an unfavorable prognostic sign.
Liver damage in leptospirosis is manifested by its enlargement from the 3rd–11th day of illness (protrudes from under the edge of the costal arch by 2–3 cm, and sometimes more), as well as pain on palpation. Simultaneous enlargement of the spleen is observed in half of the patients. Liver damage in the icteric form of leptospirosis can reach the level of liver failure with the development of encephalopathy, which has an unfavorable prognosis, especially in combination with other complications of leptospirosis - acute renal failure (ARF) and hemorrhagic syndrome.
During the height of leptospirosis, kidney damage is recorded in 50–100% of cases. In mild cases of the disease, only deviations in urine tests can be observed, in severe cases, acute renal failure develops. In addition, in severe cases, infectious toxic shock (ITS) may develop already from the 3rd–4th day of illness. Diuresis decreases to 500 ml/day. and less. Proteinuria increases in the urine; in urine sediment the number of leukocytes, erythrocytes, and casts increases. The level of nitrogen-containing compounds in the blood increases. There is a decrease in both secretory and excretory functions of the kidneys. Kidney damage is especially pronounced from the 7th–10th day of illness. Oliguria may give way to anuria, proteinuria may reach 30 g/l; the urea content in the blood will increase to 49.9-90.7 mmol/l, creatinine - to 1432-1945 µmol/l. Uremic syndrome may develop and be fatal. A feature of acute renal failure in leptospirosis is the absence of edema and arterial hypertension. Hyperkalemia, characteristic of the oligoanuric stage of acute renal failure, is detected in isolated cases; hypokalemia is more often observed.
ARF occurs more often in the icteric form of leptospirosis, especially caused by L.icterohaemorrhagiae, and can be combined with acute liver failure. In severe forms of leptospirosis during the height of the disease, combined acute renal-liver failure becomes the leading clinical syndrome and is the most common cause of death.
With a favorable course of leptospirosis, as recovery progresses, oligoanuria is replaced by polyuria with hyposthenuria and a gradual restoration of renal concentration function over 2–4 weeks. With leptospirosis, a non-oliguric type of acute renal failure is possible without a decrease in diuresis, which usually ends in recovery.
Changes in the cardiovascular system in most patients with leptospirosis at the height of the disease manifest themselves in the form of significant muffled heart sounds, tachycardia and hypotension. Bradycardia, extrasystole, and atrial fibrillation are less common. An electrocardiographic study, even in the absence of clinical manifestations, reveals diffuse changes in the myocardium or rhythm and conduction disturbances. Myocarditis is observed in 10–12% of patients, more often in severe forms of the disease. Endo- and pericarditis may develop.
Lung damage in leptospirosis at the height of the disease, according to various authors, occurs in 3–62% of cases. More often it is acute bronchitis and focal pneumonia. Hemorrhagic pneumonia or hemorrhagic pulmonary edema may develop and cause death. Severe acute pulmonary failure in a large number of cases develops with infectious-toxic shock. Patients develop shortness of breath, bloody sputum, and hypoxemia, refractory to oxygen inhalation. X-ray examination of the lungs reveals bilateral infiltrative changes. With icterohemorrhagic leptospirosis, small- and large-focal pneumonias have been described. Leptospira can be isolated from the sputum of patients.
Damage to the central nervous system in leptospirosis, caused by specific intoxication, in the form of headaches, dizziness, insomnia, adynamia, and, less commonly, delirium and hallucinations, is detected already in the initial period of the disease. During the height of the disease, up to 40% of patients have meningeal syndrome. With leptospirosis, serous meningitis is more often noted, and purulent meningitis, encephalitis, polyradiculitis, paresis, and paralysis are less common. In severe forms of the disease, toxic encephalopathy and cerebral edema may develop. Meningeal symptoms most often occur at the end of the 1st - beginning of the 2nd week of the disease, but may also accompany relapses of the disease. With the development of meningeal syndrome, the condition of patients worsens significantly, the headache intensifies, photophobia and vomiting appear, stiffness of the neck muscles and a positive Kernig and Brudzinski sign are determined. When examining cerebrospinal fluid, lymphocytic pleocytosis is more often detected, and mixed or neutrophilic less often. Changes in the cerebrospinal fluid in patients with leptospirosis in the absence of meningeal symptoms are described. The prognosis for leptospirosis meningitis is usually favorable. Liquorological changes in some cases persist longer than meningeal symptoms. With the development of encephalitis, the prognosis worsens and death may occur.
Leptospirosis at the height of the disease is characterized by hemorrhagic syndrome. More often it is observed in the icteric form of the disease. The first signs of hemorrhagic syndrome in the form of hemorrhages in the sclera, hemorrhagic rash, nosebleeds appear on the 3rd–4th day of illness and can be harbingers of more serious hemorrhagic complications. Hemorrhagic syndrome reaches its maximum in the 2nd week of the disease. These are hemoptysis, pulmonary and gastrointestinal bleeding, gross hematuria, hemorrhages at injection sites and in various organs. In severe cases of the disease, DIC syndrome develops, which can cause death.
Rare manifestations of leptospirosis at the height of the disease can be diarrhea, acute pancreatitis, non-calculous cholecystitis, mumps, iridocyclitis, uveitis, optic neuritis.
The main causes of death in patients with leptospirosis are ITS (develops in the 1st–2nd week of the disease) and acute renal-liver failure in combination with hemorrhagic syndrome (develops in the 2nd–3rd week of the illness).
With a favorable course of leptospirosis, a gradual recovery of patients begins from the 2nd (for a mild form of the disease) - 4th week. Feeling better, headaches and muscle pains, jaundice, hemorrhagic manifestations disappear, diuresis is restored. The duration of the disease is usually from 4 to 6 weeks. After suffering from leptospirosis, asthenovegetative syndrome and general muscle weakness can persist for a long time.
The relapse rate for leptospirosis is 20–60%. A second attack of fever occurs, and all the symptoms of the disease recur, but, as a rule, in a milder form. The duration of relapse ranges from 1 to 6 days. There may be several relapses. During the period of convalescence, complications and residual effects are more often observed in the organ of vision (uveitis, iritis, iridocyclitis, optic nerve atrophy, blindness) and the nervous system (mono-, polyneuritis, arachnoiditis).
Consequences and complications
If timely and correct treatment is not provided, leptospirosis can provoke the development of serious complications:
- Kidney damage, up to the development of renal failure.
- Damage to the nervous system – encephalitis , polyneuritis, meningitis .
- Liver failure.
- Leptospirosis myocarditis .
- Heart damage.
- Pancreatitis.
- Damage to the upper respiratory tract - pneumonia .
- Hemorrhages in the adrenal glands and hemorrhages in the sclera of the eye.
- Eye damage – iritis , uveitis , iridocyclitis .
- Paralysis and paresis .
- Toxic shock.
- In children - Kawasaki syndrome .
Laboratory diagnostics
In the initial period and the height of the disease with leptospirosis, neutrophilic leukocytosis, a shift in the leukocyte formula to the left, aneosinophilia, and lymphopenia are noted. ESR increases to 50–60 mm/h. In severe forms of leptospirosis, especially caused by L. Icterohaemorrhagiae, a decrease in the number of red blood cells, hemoglobin level, and platelet count is observed in the blood test. The number of red blood cells may decrease to 2 x 1012/l and below. Disturbances in the hemostasis system occur as DIC syndrome.
Pathological changes such as leukocytes, erythrocytes, casts in urine sediment are observed in almost all patients with leptospirosis, reaching a significant degree in severe forms of the disease. With the development of acute renal failure, the levels of urea and creatinine in the blood increase.
The activity of aminotransferases, reflecting liver function, even in patients with severe icteric form of leptospirosis with high levels of blood bilirubin increases, as a rule, by 2–3 times. Deviations in sediment samples (thymol, sublimate, formol) do not occur in all cases.
An increase in serum creatine phosphokinase as an indicator of muscle tissue damage has a certain differential diagnostic significance for leptospirosis.
Humans do not have natural immunity to leptospirosis. After an infection, long-term and durable immunity is formed, predominantly serovar-specific. Specific anti-leptospirosis antibodies (agglutinins, lysins, hemolysins, precipitins, complement-fixing hemagglutinins) appear in the blood of patients from the 6th–7th day of the disease and reach maximum titers in the period of convalescence. In the first 10 days of the disease, specific IgM increases in the blood, causing the primary immune response. Their titer quickly increases and also quickly decreases, and after 3-4 months they usually disappear altogether. The IgA content increases moderately.
From the 10th day of the disease, the amount of IgG increases, which persist for a long time and are considered as “anamnestic” antibodies.
Specific laboratory diagnosis of leptospirosis includes microscopic, bacteriological, biological, immunological (serological) methods.
Immunological methods are the main ones in the laboratory diagnosis of leptospirosis in humans. They make it possible to identify specific antibodies in the blood of patients and those who have recovered from the disease, and to detect Leptospira antigens in biological fluids.
To date, the most specific and reliable serological method is the microagglutination reaction (MMA) with live cultures of Leptospira. For the study, paired sera are taken (the first - on the 5-7th day of the disease and the second - after 7-14 days) and the determination of agglutinins with strains of 13 serogroups of Leptospira is carried out. The diagnosis of leptospirosis is confirmed by a change in PMA from negative to positive or an increase in antibody titer during the course of the disease. A dilution of 1:100 is considered a diagnostic titer, but it should be borne in mind that a single study is not always informative. In endemic areas, antibodies to Leptospira, even in high titers, are often found in healthy people who have previously had leptospirosis. However, a negative reaction result does not exclude leptospirosis in all cases, since in some patients, especially in severe cases of the disease, antibodies in some cases are formed late and in low titers.
To detect antibodies, you can also use the passive hemagglutination reaction, indirect immunofluorescence, and the enzyme immunoassay method.
To identify Leptospira antigens, radioimmunoassay and enzyme immunoassay, indirect hemagglutination inhibition reaction, various variants of the immunofluorescence method, and polymerase chain reaction are currently used.
Differential diagnosis of leptospirosis is carried out with influenza, hemorrhagic fevers, typhoid-paratyphoid diseases, yersiniosis, hepatitis (viral, toxic), malaria, meningitis, sepsis.
Pathogenesis
As a rule, the infection enters the body through wounds, mucous membranes, the gastrointestinal tract, and the genitourinary system. You can become infected through soil, water, and food. The incubation period in most cases lasts from 4 days to 2 weeks. However, sometimes it can last for a month. Most often, infections occur in late summer and autumn.
After infection, several phases of disease development are determined. In the first phase, the causative agents of the disease penetrate into the blood through the affected mucous membranes and skin, after which the leptospires invade the kidneys, liver, spleen, and adrenal glands, where they actively reproduce. This is the incubation period of the disease.
This is followed by a phase of generalized infection . During this period, repeated leptospiremia occurs, after which the pathogen enters the liver, kidneys, adrenal glands, and membranes of the brain. During this period of the disease (initial), Leptospira parasitizes on the surface of cells.
In the toxinemia , the disease progresses. The endothelium of the capillaries is damaged, as a result of which their penetration increases. Hemorrhagic syndrome develops , the kidneys, liver, and adrenal glands are affected.
During the formation phase of the non-sterile stage of immunity, antibodies appear in the blood, and the process gradually begins to fade.
In the sterile stage of immunity, humoral immunity is combined with local organ and tissue immunity. At this stage, the healing process occurs.
However, there are several varieties of the pathogen, so immunity to one type does not provide protection against other varieties.
Treatment approaches
Treatment of patients with leptospirosis is carried out only in a hospital. Complex therapy includes bed rest, hygienic care, good nutrition, the prescription of etiotropic drugs and strictly individualized pathogenetic treatment.
The most effective etiotropic drugs for leptospirosis are penicillin and its derivatives. Penicillin is prescribed intramuscularly at a dose of 4–12 million units/day. within 10–14 days. If you are allergic to penicillin, use chloramphenicol at a dose of 30–50 mg/kg/day. In the absence of renal-hepatic failure and severe hemorrhagic syndrome, doxycycline (0.2 g/day) can be prescribed. If etiotropic therapy begins later than the 4th–5th day from the onset of the disease, then its effectiveness is sharply reduced.
If there is a need for a second course of antibiotic therapy, semi-synthetic penicillins, cephalosporins, and chloramphenicol are used.
Specific bovine leptospirosis immunoglobulin, previously used as etiotropic therapy for severe leptospirosis, was ineffective, and is currently not available.
Pathogenetic therapy for mild and moderate forms of leptospirosis includes the prescription of analgesics, antihistamines, enterosorbents, and infusion therapy. In severe forms of the disease, intensive therapy, including detoxification, correction of disturbances in homeostasis and the functions of vital organs, becomes of particular importance in the complex of therapeutic methods.
If conservative treatment is ineffective in patients with increasing renal and hepatic failure, extracorporeal detoxification methods are used - hemosorption, hemofiltration, hemodialysis, plasmapheresis.
Treatment with folk remedies
Since leptospirosis is a serious disease that requires urgent medical attention, in this case you should not hesitate and self-medicate. The use of folk remedies for leptospirosis is possible only as an auxiliary treatment, but in no case as the main therapy. It is advisable to use folk remedies during the recovery period - to restore the body and maintain the functioning of internal organs. The following means can be used:
- Fresh apple juice with honey - drink with 1 tsp. It is recommended to drink honey every day on an empty stomach.
- Beetroot and carrot juice - freshly squeezed vegetable juices should be diluted in half with water and drunk a third of a glass on an empty stomach.
- Potato juice – it should be drunk fresh. Drink half a glass half an hour before meals.
- Tomato juice with cabbage brine - it is recommended to mix them in equal proportions and drink throughout the day.
- Herbal tea - you can prepare it from chamomile, oregano, mint, lemon balm and other herbs with a general strengthening effect.
- Lemon with garlic – mix the juice of 1 lemon and 1 head of garlic. Drink half a teaspoon after meals.
Dispensary observation
Dispensary observation of those who have had leptospirosis is carried out by infectious disease specialists at clinics. The period of clinical observation is at least 6 months. Inspections are carried out once a month. In the 1st month after the illness, patients are subject to mandatory clinical examination by an ophthalmologist, neurologist and therapist. In subsequent months, specialized specialists are involved in the profile of clinical manifestations. Control general blood and urine tests, and in those who have had the icteric form of the disease, a biochemical blood test are done every month for the first 2 months, then depending on the results of the examination.
Criteria for removal from dispensary registration: clinical recovery, normalization of laboratory parameters. In case of persistent residual effects, those who have recovered from the disease are transferred under the supervision of specialists (ophthalmologist, neurologist, nephrologist, etc.) for at least 2 years.
List of sources
- Avdeeva M.G. Leptospirosis as a disease with a prolonged complicated course (immunopathogenesis, diagnosis, prognosis, treatment, rehabilitation): abstract of thesis. Dr. med. Sci. - M., 1997. - 32 p.
- Avdeeva M.G. Causes of lethal outcomes of leptospirosis / M.G. Avdeeva // Epidemiology and infectious patients. – 2003. – No. 6. – P. 30–33.
- Leptospirosis / [V.I. Luchshev, V.V. Lebedev, S.N. Zharov, S.V. Burova] // Russian Medical Journal. – 2009. – No. 4. – P. 47–49.
- Stoyanova N.A. Current problems of leptospirosis in infectious pathology of people // Sat. report/Biol. scientific-practical .-SPb., 1996.-Issue 2.-P.5-10.
Prevention
Prevention of leptospirosis is based on a complex of medical, sanitary and veterinary measures, including the protection of water bodies from pollution by animal secretions, deratization, personal preventive measures, vaccination of farm animals, vaccination of high-risk contingents in leptospirosis-endemic areas (fishermen, hunters, agricultural workers, mines, meat processing plants, sewerage networks, etc.).
Laboratory employees working with pathogenic leptospira, as well as persons sent to construction and agricultural work in places of active natural and anthropourgic foci of leptospirosis (no later than 1 month before starting work in them) are subject to routine immunization.
For emergency antibiotic prophylaxis of leptospirosis, persons at risk of infection are prescribed doxycycline 0.1 g once a day for 5 days.
"Emergency Medicine". Selected Clinical Lectures, Volume 2
Causes
The causative agent of the disease is Leptospira interrogate. It is an aerobic, gram-negative, motile, spiral-shaped rod, the reservoir of which is animals. A person with leptospirosis is not a source of infection.
The gates of infection are the mucous membranes of the mouth, nasopharynx, and damaged skin. In the body, infection spreads through lymph and blood .
The risk zone includes those people whose activities are related to animals. These are veterinarians, farm owners and workers, meat industry workers, shepherds, milkmaids, etc.