What is harmful to the liver?
Drinking regularly is harmful - anyone, even someone far from medicine, knows this. And when it comes to diseases caused by excessive consumption of strong drinks, as a rule, the first thing that comes to mind is cirrhosis of the liver. Indeed, the doctor faces a difficult task when a patient comes to him with “ready-made” cirrhosis, manifested by a violation of the structure and function of the organ. You can help at this stage, but you still shouldn’t lead the disease to cirrhosis. It is much better for both the doctor and the patient when liver changes are still minimal and reversible. We are talking about the so-called fatty hepatosis or, more simply, fatty liver.
What are the signs of fatty liver disease?
As we mentioned above, the main feature of this condition is the absence of specific symptoms. Therefore, the disease is often detected by chance, often during a routine medical examination or examination for a completely different disease.
Among the symptoms that often occur with fatty hepatosis, but can be ignored, you should pay attention to:
- Discomfort in the area of the right hypochondrium, without a clear connection with food intake
- Fatigue
- Weakness
If these symptoms are detected and there is concern about the condition of the liver, then to clarify the diagnosis, you should consult a doctor who can prescribe a diagnostic method such as ultrasound. Ultrasound will help identify increased liver volumes and changes in the echogenicity of the organ. The doctor may also recommend testing liver enzymes - ALT, AST. In some cases, a specialist may see the need for a liver biopsy (examination of liver tissue under a microscope), which provides the most reliable information about the condition of the organ.1,4
What is fatty liver?
Fatty liver, fatty hepatosis, liver steatosis - all these concepts reflect the same pathological condition, which can develop as a result of exposure to a wide variety of factors. At the same time, the literal translation of the English term “fatty liver” – “fatty liver” – attracts attention because it is understandable to both the doctor and the patient. Like an obese person, a “fatty liver” is subject to a whole range of diseases. However, in most cases, fatty liver is completely reversible if the causes leading to its formation are eliminated. It is this indisputable fact that should first of all be drawn to the attention of both doctors and patients, since timely recognition of fatty hepatosis makes it possible to prevent the development of inflammation, which is much more difficult to treat.
Enter a caption for the image
Fatty liver disease, non-alcoholic fatty liver disease (NAFLD) - symptoms and treatment
The accumulation of cholesterol, namely lipids (fat-like organic compounds) in the liver, is primarily caused by the following factors:
- excess supply of free fatty acids (FFA) to the liver;
- increased synthesis of free fatty acids in the liver;
- decreased levels of beta-oxidation of free fatty acids;
- decreased synthesis or secretion of very high-density lipoproteins.[7]
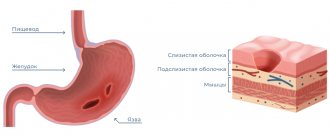
In obese patients, the liver tissue has an increased content of free fatty acids, which may be the cause of liver dysfunction, since fatty acids are chemically active and can lead to damage to the biological membranes of hepatocytes, forming a gateway for endogenous fat to enter the cell, in particular lipids (mainly low and very low density), and transport is an ester - triglyceride.[2]
Thus, hepatocytes become filled with fat, and the cell becomes functionally inactive, swells and increases in size. When more than a million cells are damaged, the liver macroscopically increases in size, in areas of fatty infiltration the liver tissue becomes denser, and these areas of the liver do not perform their functions or perform them with significant defects.
Lipid peroxidation in the liver leads to the synthesis of toxic intermediates that can trigger the process of apoptosis (programmed cell death), which can cause inflammation in the liver and form fibrosis.[2]
Also of important pathogenetic importance in the formation of NAFLD is the induction of cytochrome P-450 2E1 (CYP2E1), which can be induced by both ketones and a high-fat, low-carbohydrate diet.[7] CYP2E1 generates toxic free radicals leading to liver damage and subsequent fibrosis.
In addition, endotoxin-mediated damage is of pathogenetic importance in the formation of NAFLD, which, in turn, enhances the production of pro-inflammatory cytokines (TNF-α, IL-6 and IL-8), leading to disruption of the integrity of hepatocyte membranes and even to their necrosis[ 9], as well as to the development of inflammatory cell infiltration both in the portal tracts and in the liver lobules, which leads to steatohepatitis.
Products of lipid peroxidation, hepatocyte necrosis, TNF and IL-6 activate stellate (Ito) cells, causing damage to hepatocytes and the formation of fibrotic changes.
Symptoms of alcoholic liver disease
The symptoms of this disease are very ambiguous, it depends on the stage of development of the disease. For example, at the initial stage, the pathology may not manifest itself at all. It is worth paying attention to the following general symptoms of alcoholic liver disease, characteristic of any stage:
- heaviness, tingling and other discomfort in the hypochondrium on the right side;
- lethargy, general weakness;
- decreased performance;
- drowsiness;
- elevated body temperature (37.0-37.9 degrees);
- sweating;
- headache;
- lack of appetite;
- increased irritability, even aggressiveness;
- yellow skin tone.
Liver diseases almost always affect the functioning of other organs and systems - therefore the following accompanying symptoms are not uncommon:
- bloating;
- upset stomach, diarrhea, constipation;
- belching, heartburn;
- pain and aches in the joints;
- bitter taste in the mouth.
The presence of these signs is a signal of liver dysfunction, so it is recommended to consult a specialist as soon as possible. An experienced hepatologist at the ABIA clinic will listen to the patient’s complaints, conduct the necessary studies and, based on the diagnosis, prescribe correct and timely treatment.
Alcoholic hepatitis and liver cirrhosis
Alcoholic hepatitis, according to the International Classification of Diseases of the Liver Organ, is divided into acute and chronic. The disease is one of the main variants, along with alcoholic fibrosis, which transforms into cirrhosis
.
Acute alcoholic hepatitis - episodes of acute toxic necrosis (acute liver failure of alcoholics) are extremely difficult and often pose a threat to the patient’s life. This form of hepatitis develops in 30% of patients who abuse alcohol for at least 3-5 years, and malnutrition, parental alcoholism, decreased activity of acetal and alcohol dehydrogenase, and decreased HLA B40 antigen play a role.
The relationship between the lack of histocompatibility antigen HLA B40 and the development of chronic active hepatitis with subsequent transition to cirrhosis
.
This form of hepatitis (acute necrosis) can develop against the background of fatty liver
, acute hepatitis, fibrosis or cirrhosis.
In cirrhosis,
the development of acute hepatitis (necrosis) very often leads to decay (parenchymal) and shunt (portocaval) hepatic encephalopathy, which most often ends in death.
Histologically, perivenular damage to hepatocytes, balloon degeneration, their necrosis, alcoholic hyaline (Mallory bodies), leukocyte infiltration, pericellular fibrosis, etc. are observed. Necrosis of hepatocytes in the center of the hepatic hexagonal lobules.
Acute hepatitis often develops in young and middle-aged people after binge drinking with previous long-term alcohol consumption. An acute onset of pain and dyspeptic syndromes is typical, but in some patients the disease can develop gradually.
The most common icteric variant: severe weakness, lack of appetite, nausea, vomiting, jaundice, diarrhea, and sudden loss of body weight. The pain is localized in the right hypochondrium, epigastric region. There may be a fever.
Examination reveals jaundice, hepatomegaly, and fever. The area where the organ is located is painful on palpation and smooth. In some patients, the spleen enlarges, palmar roofing material (erythema), skin spider veins, hand tremors (asterixis), which is a sign of hepatic encephalopathy, mental disorders (lethargy, agitation, hallucinations), ascites resistant to diuretics. Concomitant infections are noted: pneumonia, pyelonephritis, active tuberculosis. The cholestatic variant with skin itching, light-colored feces, and dark urine are rare. The blood is characterized by severe hyperbilirubinemia, hypercholesterolemia, increased activity of alkaline phosphatase, gammaglutamyl transpeptidase, and a slight increase in AST and ALT.
There are fulminant (fulminant) acute alcoholic hepatitis, which is severe, often with an unfavorable prognosis, and a latent variant with an asymptomatic course. Leukocytosis with a shift to the left and a sharp increase in ESR are always observed.
Prognostically unfavorable symptoms are hepatic encephalopathy, hepatorenal syndrome, prolongation of prothrombin time by more than 50%, relapses of acute hepatitis at the stage of established cirrhosis. The prognosis is most favorable for the latent form of acute hepatitis.
Recovery is possible with complete abstinence from alcohol, but this does not always guarantee the absence of subsequent cirrhosis
.
Chronic hepatitis is divided into persistent and active mild, moderate, severe, most often representing stages of progression of acute hepatitis.
Chronic persistent hepatitis is histomorphologically manifested by pericellular and subsinusoidal fibrosis, Mallory bodies, balloon degeneration of hepatocytes. A similar picture without progression of fibrosis can persist for 5-10 years, even with moderate alcohol consumption.
Chronic persistent hepatitis is accompanied by moderate abdominal pain, bloating, anorexia, unstable stools, belching, and heartburn. The liver organ is slightly enlarged and compacted. Diffuse compaction, increase confirmed by ultrasound data. The activity of gammaglutamyl transpeptidase, serum transaminases, and sometimes the thymol test increases moderately.
Chronic active hepatitis has the above-described histomorphological picture of alcoholic hepatitis with the presence of more or less pronounced active fibrosis, sclerosing hyaline necrosis. Abstinence from alcohol for 3-6 months. leads to an improvement in the morphological picture of the type of chronic non-alcoholic hepatitis. Chronic active hepatitis in the presence of autoimmune destruction of the parenchyma is characterized by progression of the process with the transition to cirrhosis
.
Clinical manifestations are more striking than with persistent hepatitis. Jaundice and splenomegaly are more often observed (when transitioning to cirrhosis, the organ can sharply shrink). Bilirubin, gammaglutamyl transpeptidase, immunoglobulin A, moderate thymol test, and blood transaminase activity increase significantly.
There are no direct morphological markers of the alcoholic etiology of diseases of the liver organ, but there are changes that are quite characteristic of the effects of ethanol. This is alcoholic hyaline (Mallory bodies), characteristic ultrastructural changes in hepatocytes, stellate reticuloepitheliocytes. Hyalin is a protein substance synthesized by hepatocytes. In light-optical examination, it has the appearance of eosinophilic masses of various shapes (ribbon-like, reticular, globular, irregular), which are usually localized near the nucleus of the cytoplasm of hepatocytes. After the death of the hepatocyte, it can be located extracellularly. With Mallory's tricolor stain, hyaline accumulations are colored pink.
In electron microscopic examination of biopsies taken from patients with chronic alcoholism, alcoholic hyaline is detected as fibrillar or granular material. Hyaline fibrils are shorter and thicker than normal tonofilaments. The formation of Mallory bodies in hepatocytes has been described in a number of diseases of non-alcoholic etiology: diabetes mellitus, Indian childhood cirrhosis, Wilson-Konovalov disease, primary biliary cirrhosis, liver cancer, after intestinal anastomosis for obesity.
Characteristic ultrastructural changes in hepatocytes and stellate reticuloendotheliocytes reflect the toxic effects of ethanol on the body.
Changes in hepatocytes are represented by hyperplasia, vacuolization of elements of the smooth cytoplasmic reticulum, and the formation of giant mitochondria with an irregular shape. Changes in stellate reticuloepitheliocytes indicate the failure of their phagocytic function: their cytolemma does not form outgrowths, single lysosomes with electron-light content.
Constantly occurring morphological markers of the effects of ethanol on the liver are:
- fatty degeneration of hepatocytes;
- foci of liquefaction necrosis affecting the central parts of the lobules;
- inflammatory infiltrate containing, along with lymphocytes and macrophages, a large number of neutrophilic leukocytes;
- restructuring of the liver organ with the formation of false lobules of a predominantly monolobular type separated by narrow fibrous septa.
An important diagnostic value for chronic hepatitis (alcoholic, like any other etiology) is an ultrasound of the abdominal organs (liver, spleen and other organs), as well as to identify ascites and the size of the portal vein. Doppler ultrasound should be performed to exclude or establish the severity of portal hypertension. Traditionally, radionuclide hepatosplenoscintigraphy continues to be used for diagnostic purposes.
Nutrition for AFLD
The liver is a kind of “filter” in the human body; its condition directly depends on the person’s lifestyle and nutrition. When treating liver diseases, it is important not only to maintain sobriety, but also to monitor your diet - the doctor prescribes a therapeutic diet that includes a large amount of:
- vitamin E;
- B vitamins;
- Selena;
- zinc;
- amino acids.
As a rule, the patient needs to eat more fresh vegetables and fruits and limit himself to heavy, fatty, canned foods. This will help the liver recover faster and get rid of the disease.
The ABIA Clinic invites patients to undergo examination by a professional hepatologist. Remember - the initial stage of AFLD may not manifest itself in any way for quite a long time, developing even in those who drink “like everyone else” on holidays. Here you can undergo diagnostics using modern and accurate equipment, identify pathology in a timely manner and receive high-quality treatment when the diagnosis is confirmed.
Don’t delay visiting your doctor—alcoholic liver disease is becoming an increasingly common and very dangerous disease. Visit a hepatologist at the ABIA clinic and prevent the development of pathology!
Diagnostics
In addition to standard general clinical tests, the following are required:
- blood biochemistry;
- liver tests;
- coagulogram;
- analysis to determine the level of electrolytes in the blood;
- studies to identify the main markers of hepatotropic viruses, HIV;
- immunogram to assess immune function and possible concomitant autoimmune diseases;
- analysis to determine indicators of lipid and protein metabolism;
- test for blood glucose levels.
Also for liver intoxication:
- Ultrasound (usually reveals hepatomegaly, splenomegaly, characteristic changes in echostructure);
- Doppler ultrasound to assess blood flow in the portal and splenic veins;
- gastroscopy;
- elastography (non-invasive technique for diagnosing cirrhosis);
- CT or MRI;
- biopsy (if hepatocellular carcinoma is suspected).
Alcohol and the liver. What diseases are caused by excessive drinking?
It's no secret that in modern realities, in order to relax, people are increasingly turning to alcohol. Today, there are 4 types of liver diseases that are caused by alcohol:
- Fatty liver degeneration (Fatty liver)
- Hepatitis in acute form
- Chronic hepatitis
- Cirrhosis of the liver.
However, the relationship between the severity and extent of liver tissue damage remains unknown, as well as the reasons why some individuals may develop cirrhosis of the liver while drinking alcohol, while others suffer from heart disease or pancreatic disease.
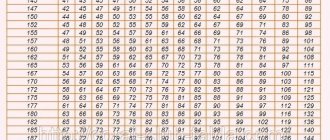
Permissible amount of alcohol consumed:
The World Health Organization does not recommend taking more than 21 drinks of alcohol for men and 14 drinks for women in a 7-day period. With 1 serving = 150 g. dry wine/=250 gr. beer/=30 g. fortified alcohol.
Why does the liver suffer from alcohol?
This is primarily due to the function of the liver in the human body. It processes most of the alcohol (ethanol), as a result of which destructive toxic substances are formed in this organ.
Steatosis or fatty degeneration of the liver. (Fatty Liver)
Due to alcohol consumption, excess weight, or, less commonly, prolonged dysbacteriosis or fasting, fat accumulation occurs in liver cells.
Also, as a result of the development of type 2 diabetes mellitus, non-alcoholic fatty liver degeneration may appear. When liver cells are filled with fat, the tissue of the organ changes and fibrosis develops.
Diagnosis and treatment of steatosis (fatty liver) of the liver.
The liver is rightfully considered a unique organ of the human body, because. Has huge recovery reserves. To prescribe effective treatment, be it diet or medication, the patient undergoes an examination at our medical center. With the help of ultrasound, a specialist is able to detect an increase in the size of the liver and detect indirect signs of its obesity. A standard biochemical blood test will show an increase in AST, GGTP and cholesterol (remember: a blood test will not be able to reflect the process of fibrosis development). Performing a biopsy was previously considered the most effective method of studying the depth of liver damage, but nowadays this method is used quite rarely.
PLEASE NOTE: our center performs FIBROTEST and FIBROMAX, a complex biochemical blood test that can objectively reflect the stage of liver fibrosis.
Fibromax consists of:
- Fibro test is a detailed analysis of the condition of the liver, as well as diagnosing the development of fibrosis.
- Steato test - diagnosing the development of fatty degeneration, special assessment of the liver.
- Nash test – liver diagnostics in patients with metabolic syndrome; diagnosis of the possibility of developing non-alcoholic liver inflammation.
- Ash test - diagnosis of the liver, in cases where the patient drinks alcohol excessively; diagnosing the possibility of developing fatty alcohol inflammation of the organ.
- Acti test – assesses the state of development of liver tissue necrosis.
Alcoholic hepatitis in acute form.
It occurs due to alcohol consumption and is expressed in acute inflammation of the liver tissue. In severe cases, hospitalization is required. Symptoms: swelling, jaundice, tremors, increased body temperature, agitation and increased sweating, pain in the abdomen, disturbances in the intellectual functioning of the brain. In the patient's blood test, the following indicators increase: AST-ALT-GGTP-cholesterol and uric acid, ESR, bilirubin and alkaline phosphatase.
With alcoholic cirrhosis, connective tissue develops in the liver, the organ loses its functions, which certainly indicates severe damage to the organ.
The appearance of the patient also leaves much to be desired, small vessels dilate, the hands are deformed, the mammary glands in men become enlarged, redness of the palms occurs, a puffy, swollen face, and enlargement of the parotid glands. Also, against the background of long-term alcohol consumption, complications of the nervous system, muscle atrophy, decreased level of intellectual abilities, pancreatitis and gastritis occur.