Diffuse large B cell lymphoma (DLBCL) is a group of tumors of the lymphatic system, which is based on the transformation of B lymphocytes into malignant cells.
- Causes and risk groups
- Symptoms of diffuse large cell B lymphoma
- Classification, forms and stages of diffuse lymphoma
- Diagnosis of diffuse large cell lymphoma
- Treatment of diffuse large B-cell lymphoma
- Recovery after treatment for large cell non-Hodgkin lymphoma
- Relapses of large cell lymphoma
- Complications of diffuse large B cell lymphoma
- Prognosis and prevention of large cell lymphoma
What are lymphomas?
Lymphomas belong to the group of hemoblastoses, that is, tumor diseases that develop from blood cells. Conventionally, hemoblastoses include:
- leukemia - with primary localization in the bone marrow
- non-leukemic hemoblastoses - characterized by tumor localization outside the bone marrow. These are non-Hodgkin's lymphoma and Hodgkin's lymphoma.
Non-Hodgkin's lymphoma (NHL) is a malignant disease of the lymphatic system. The name "malignant lymphoma" literally means "malignant enlargement of the lymph nodes." This medical term covers a large group of cancers that begin in the cells of the lymphatic system.
Prevalence of NHL in children:
- In childhood, NHL ranks 3rd among all oncological pathologies, accounting for 5-7%.
- The incidence of the disease in children under 15 years of age is 1:700-750 people. Boys get sick more often than girls. The peak incidence occurs between 3 and 9 years of age.
- NHL is extremely rare in children under 3 years of age.
Get a free consultation
Leading specialists of the Center will answer your questions.
To get a consultation
Find out the price
Lymphomas are a type of malignant tumor that affects the lymphatic system. Non-Hodgkin's lymphomas include all lymphomas except Hodgkin's lymphoma. This group of diseases is very heterogeneous and includes very different course patterns, structures and characteristics.
In the structure of cancer incidence, the share of non-Hodgkin lymphomas (lymphosarcoma) is approximately 3%. In Belarus this figure is slightly lower.
It is worth noting that over the past 10 years there has been an increase in the incidence of NHL in many countries of the world, including Belarus. If in 2001 there were 470 cases, then in 2010 there were already 638, i.e. the incidence increased 1.4 times.
Causes of lymphoma development
The disease begins to develop when lymphocytes mutate, that is, they change malignantly. Why this happens is unknown. Lymphocytes are a group of white blood cells that are found primarily in lymphatic tissue. Therefore, non-Hodgkin's lymphomas can appear anywhere there is lymphatic tissue. Most often, the disease develops in the lymph nodes. But it can also develop in other lymphoid tissues and lymphoid organs, for example, the spleen, thymus (thymus gland), tonsils and lymphatic plaques of the small intestine.
Some viruses can cause NHL. A number of studies have established a possible connection between viruses and some forms of NHL.
When should you take your child to the doctor?
- If there is an enlargement of at least one lymph node, which cannot be associated with an infectious process.
- If the child is lethargic, weak, has stopped doing well at school, and sleeps a lot.
- If, while maintaining the same diet, the baby loses weight.
- If sweating is periodically or constantly observed, mainly at night.
- If your body temperature regularly rises and stays at 37.1-37.4.
- If a child has chronic diseases that take a long time to be treated and cannot be put into remission.
Clinical stages of NHL
- Stage I - tumor damage to individual lymph nodes of one anatomical group or damage to one lymphoid tissue. With the exception of damage to the lymphoid tissue inside the chest and in the abdominal space.
- Stage II - tumor involvement of lymph nodes of several anatomical groups or involvement of other lymphoid tissues with local spread and without local spread. But all regions affected by the tumor are on one side of the diaphragm.
- Stage III - tumor damage to the lymph nodes or lymphoid tissue on both sides of the diaphragm. Or the tumor has affected the lymphoid tissue or other organs inside the chest - mediastinum, pleura, thymus, lungs. Also extensive inoperable tumors in the abdominal cavity.
- Stage IV - tumor damage to the central nervous system (CNS) and (or) bone marrow.
Non-Hodgkin's lymphomas in children and adolescents are characterized by rapid progression of the oncological process. The tumor grows so quickly that most children are admitted to the clinic already in stages III-IV of the disease.
However, regardless of the stage of the process, childhood lymphomas have good sensitivity to chemotherapy treatment, which allows up to 80% of patients to be cured.
Course of the disease
The progression of lymphoma is largely determined by the morphology and immunology of the cell that initiated tumor growth.
Thus, if a cell was transformed into a malignant one at an early stage of its development and did not have time to leave the bone marrow, then the result is a picture of predominantly bone marrow tumors (acute lymphoblastic leukemia, lymphoblastic lymphoma).
In cases where the ancestor of the tumor clone becomes a more mature cell of the lymphoid series, which leaves the bone marrow during maturation, the lesion is initially localized in the peripheral lymphoid organs and is characterized by a more favorable course.
Clinical symptoms of lymphomas
Often the first manifestation of the disease is an enlargement of the lymph nodes, which, as a rule, do not hurt, acquire a rocky density, and merge into conglomerates. Lymph nodes can be detected in the head, neck, arms, legs, armpits, groin areas, chest or abdominal cavities. Often the disease spreads to other organs - the spleen, liver, meninges, bones, bone marrow.
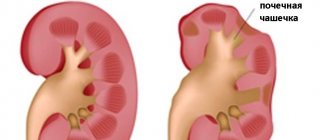
If the tumor is localized in the abdomen, the patient may experience nausea, vomiting, and loss of appetite, which quickly leads to significant weight loss and dehydration. Patients often complain of abdominal pain, and upon examination a large, dense, large tumor is detected. Fig.1. The disease can manifest itself as intestinal obstruction, “acute abdomen” syndrome associated with bleeding, intussusception, perforation of the tumor-affected intestine, which require immediate qualified surgical treatment.
Rice. 1. Nodular formation of the right kidney, merging with a conglomerate of enlarged retroperitoneal lymph nodes - a specific lesion for lymphoma
The liver and spleen are often enlarged.
When the tumor process is localized in the chest, typical complaints include coughing, difficulty breathing and swallowing, and sometimes loss of voice.
A very serious complication that develops with a sharp and significant enlargement of the mediastinal lymph nodes is compression syndrome of the superior vena cava. It is manifested by breathing problems, swelling and cyanosis of the face and neck. The appearance of these symptoms threatens the patient’s life and requires immediate medical attention.
In addition, fluid accumulation may develop in the pleural cavity and pericardial sac, which also quickly leads to respiratory disorders.
The disease can manifest itself with the appearance of complaints of nasal congestion, breathing problems, and the sensation of a foreign body when swallowing, which occurs when the lymphopharyngeal (Waldeyer's) ring is damaged. On examination, there is an enlargement of the tonsils, a tumor hanging from the nasopharynx, which often closes the entrance to the oropharynx. With this localization, enlarged cervical and submandibular lymph nodes are most often found.
When bathing and changing a child, parents may notice the appearance of nodular formations ranging in size from a pea to the size of a walnut, with a dense consistency of flesh-colored or bluish-reddish color with possible ulceration on the surface. This is how soft tissue damage manifests itself in lymphoma. The favorite localization of soft tissue formations is the scalp, anterior chest and abdominal wall, and back.
In boys, the disease can often manifest itself as an increase in the size of the scrotum.
When the central nervous system is damaged, symptoms such as headache, impaired vision, hearing, speech, paresis and paralysis are characteristic.
Primary bone lesions in children and adolescents are rare (2-4%). In this case, the pelvic bones, shoulder blades, and tubular bones are affected with the presence of various sized areas of destruction of the bone structure.
Introduction
Non-Hodgkin's lymphomas (NHL) are a heterogeneous group of lymphoproliferative diseases of the hematopoietic system, characterized by a variety of morphoimmunological variants, characterized by a highly aggressive course in childhood with rapid dissemination, damage to the bone marrow and central nervous system [1].
This group of nosologies accounts for up to 12% of all malignant tumors in children [2], ranking third in the structure of cancer incidence among children [3]. The incidence in the children's age group is 11.5 cases per 100 thousand people per year [3]. The peak age for diagnosing the disease is the period from 5 to 9 years [3]. Localization in the lymph nodes is possible; there are frequent cases of extranodal lymphomas with a source in the lymphoid tissue of the mucous membrane of the gastrointestinal tract, bronchi, and urinary tract. If more than 25% of tumor cells are found in the bone marrow, acute leukemia is diagnosed [4]. In the structure of childhood morbidity in this broad group, the following morphological variants lead [5]:
- Burkitt's lymphoma accounts for 38–43% of all NHLs;
- T- (T-LL) and B-lymphoblastic (B-LL) lymphomas – 29%;
- diffuse large B-cell lymphoma (DLBCL) – 13%;
- anaplastic large cell lymphoma (ALCL) – 10–15%;
- mediastinal large B-cell lymphoma (MCLCL) – 4%.
Burkitt's lymphoma is characterized by the most aggressive course; its fraction of proliferating cells is maximum (Ki-67 about 100%) [6]. However, high proliferative activity also determines good sensitivity to cytostatic therapy.
Etiology
In the vast majority of cases, the etiology of NHL remains unknown. It has been established that mutations that occur in the affected cell are formed against the background of activation of proto-oncogenes (MYC, BCL-2, BCL-6, PIM-1, PAX-5) and inactivation of anti-oncogenes (p16INK4a, P53, P27KIP1) [7]. Not conclusively proven, but possible environmental effects have been reported [8].
These include chemicals (herbicides, chlorophenols, history of chemotherapy); physical (radiation, radiation therapy history). The influence of immunodeficiency conditions (Down, Klinefelter, Louis-Bar syndrome, HIV), autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus, Sjögren's syndrome), and infectious diseases (infectious mononucleosis) has also been reported [9].
Clinical picture
The clinical picture of NHL in children develops quickly. As a rule, the initial symptoms are determined by the location of the tumor. In the presence of formations in the mediastinum (in particular, with lymphoblastic lymphoma), respiratory disorders, cough and respiratory failure with pleurisy, dysphagia, exudative pericarditis, and signs of compression of the superior vena cava may be observed [10]. Disorders of the gastrointestinal tract, a picture of an acute abdomen, ascites - this is how the clinical picture of B-mature cell tumors often unfolds, and hepatosplenomegaly can be detected; with a large volume, the tumor can be detected by palpation [11]. If the ovaries are involved, an acute abdomen may also appear. Due to the rapid dissemination of the process, along with any of the above pictures and separately from them, the development of a symptom complex of damage to the central nervous system is possible, with germination into the epidural space – compression of the spinal cord [12]. Often, against the background of dissemination of the disease, the testicles are affected, but their primary damage is also possible [13]. The lymph nodes involved in the process are enlarged, painless, dense, asymmetrical, and can merge into conglomerates. No positive dynamics are observed with the use of antibacterial therapy. Hemorrhagic and pain syndromes can be detected at any tumor location.
Patients with NHL also experience common symptoms. Their severity is variable and depends on the extent of the disease and the duration of its course. Against the background of intoxication, there is a decrease in appetite and lethargy. The disease may be accompanied by fever and weight loss [1]. However, these symptoms rarely come to the fore; manifestations associated with the localization of the tumor are considered to be decisive in the clinical picture of the disease.
Diagnostics
The initial examination includes the collection of complaints, anamnesis, and physical examination.
An assessment of laboratory data is carried out: clinical (assessment of the blood count, special attention is paid to platelets - if their number is less than 30 thousand / μl, replacement therapy is necessary before invasive interventions) and biochemical (assessment of liver function, kidney function, lactate dehydrogenase activity, uric acid content, electrolytes ) blood tests, coagulogram (fibrinogen, prothrombin index, thrombin time, activated partial thrombin time, XIIa-dependent fibrinolysis), urine analysis and diuresis assessment, determination of blood group and Rh factor, serum immunoglobulins, markers of viral infections.
Upon admission, a bone marrow puncture is performed from 2–4 points for the following studies:
- myelogram;
- cytological examination;
- immunophenotyping (if bone marrow is involved).
In addition, a lumbar puncture is performed for cytological and biochemical studies. It should be taken into account that cerebrospinal fluid analysis should be performed only during atraumatic puncture [1].
Mandatory instrumental studies are aimed at searching for the underlying formation, identifying metastases, assessing the extent of the process and complications.
These include:
- ultrasound examination (ultrasound) of the abdominal organs, pelvis, peripheral lymph nodes, testicles;
- X-ray examination of the chest organs;
- computed tomography of the chest, abdomen, and pelvis;
- Magnetic resonance imaging of the brain/spinal cord (used in the presence of neurological symptoms or a tumor in the head and neck);
- technetium scan (can be performed if skeletal bone lesions are suspected).
To obtain a tumor substrate, a biopsy of the formation or an excisional biopsy of the affected lymph node can be performed; in addition, cytological material can be made from ascitic fluid or exudate of the pleural cavity, bone marrow punctate. The drug is sent for cytological and histological examination, and immunohistochemical analysis is performed.
To determine the type of tumor and choose treatment tactics, the immunological and molecular genetic characteristics of the tumor should be studied. Reciprocal translocations are most characteristic of NHL; numerical changes in the karyotype and the formation of isochromosomes are less common [14].
The main genetic and immunomarkers detected in children with NL are presented in Table. 1 and 2.
In Burkitt's lymphoma, the expression of differentiation clusters CD19, CD20, CD10, CD22, sIgM is most often detected on the cell surface, there are no markers of T cells and progenitor cells, and high proliferative activity is determined based on the level of the Ki-67 biomarker [15]. Cytogenetic research in 80% of cases reveals abnormalities of chromosome 8 (where the c-MYC proto-oncogene is located): t(8;14) (q24;q32) - rearrangement of the c-MYC gene and heavy chains of immunoglobulin H (IgH), less often - t( 8;22)(q24;q11) – rearrangement with the lambda Ig chain locus occurs in 15%, and kappa chain – t(2;8)(q11–12;q24) – in 5% [15]. These disorders stimulate hypersynthesis of the c-MYC protein [16]. In addition to these changes, aberrations in the 1q loci are detected. 6q. 7q, 17q, di- and trisomies of chromosomes-1 and -7, deletions of chromosome-6, while rearrangements in 6q, 7q are unfavorable [17]. Currently, the effect of defects in other genes ID3, GNA13, RET, PIK3R1, SWI/SNF, ARID1A, SMARCA4 is being studied [18].
In T-LL, rearrangement of the T-cell receptor (T-cell receptor, TCR) genes is detected. More often (up to 70% of cases) changes in the karyotype are determined, but no correlations with the prognosis of the disease were found [19].
B-LL is characterized by a dependence of the disease prognosis on karyotype abnormalities. Hyperploidy is prognostically favorable provided there are no translocations and other chromosomal abnormalities [20]. Hyperploidy is typical in childhood: it occurs in 25% of cases. The worst prognosis was found in children with the t(12;21) (q13;q22) translocation, especially with hyperleukocytosis and over 10 years of age [4].
DLBCL is classified into 4 variants: centroblastic (67%), immunoblastic (12%), anaplastic (6%) and T-cell rich variant (9%) [21]. This disease is characterized by activation of the BCL-6 oncogene as a result of the t(3;14) (q27;q32) translocation. In addition, rearrangement of the c-MYC gene loci (8q24) can be detected. Separately, double-hit (with a combination of c-MYC and BCL-2 translocations) and triple-hit (plus BCL-6) lymphoma are identified, which are characterized by an extremely aggressive course and chemoresistance, which is associated with the launch of an anti-apoptotic cascade [22].
ALCL is usually ALK (anaplastic-lymphoma kinase)-positive, and the affected cell is characterized by atypia and polymorphism. This tumor is represented by three histological variants: classical, small cell and histiocytic [23]. ALCL is characterized by the expression of CD30 without B-cell and histiocytic markers, as well as the t(2;5)(q23;q35) translocation and its product, the chimeric protein ALK-NMP (nucleophosmin, nucleophosmin). Trisomy, in particular chromosome 7, is common in children [24]. An unfavorable prognostic factor is the occurrence of the t(3;8)(q26.2;q24) translocation and rearrangements in the c-MYC, MCL1, HOX11/TCL3 genes. CD3 expression is prognostically unfavorable in case of ALCL relapses: 5-year survival is 18 versus 72% for CD3-negative status [25].
Based on the examination results, the disease was staged according to S. Murphy (1980) [26]:
• Stage I – damage to one nodal or extranodal area (E), with the exception of the mediastinum and abdominal cavity;
• Stage II:
a) damage to one extranodal area with involvement of regional lymph nodes (NOT);
b) damage to two or more areas of lymph nodes on one side of the diaphragm;
c) damage to two extranodal areas with the involvement of regional lymph nodes on one side of the diaphragm (or without their involvement in the process);
d) primary lesion of the gastrointestinal tract (ileocecal angle) with involvement of mesenteric lymph nodes (or without their involvement).
• Stage III:
a) damage to two separate extranodal areas on both sides of the diaphragm (IIIE);
b) damage to two or more areas of lymph nodes on both sides of the diaphragm;
c) all primary mediastinal tumors;
d) all common lesions of the abdominal cavity and retroperitoneal space.
• Stage IV – one of the above lesions involving the central nervous system (CNS) and/or bone marrow, bones, or internal organs (liver, kidneys, lungs, pleura, skin, pericardium, stomach and other organs).
Treatment
Due to the high probability of developing emergency conditions, immediate initiation of therapy is required. When a space-occupying lesion is located in the mediastinum, compression syndrome of the superior vena cava may develop. As a rule, upon initiation of cytoreductive chemotherapy, these symptoms are leveled out and do not require surgical interventions. In case of airway compression, tracheal intubation may be performed. In case of respiratory failure caused by exudative pleurisy, with effusion of pericarditis and the threat of cardiac tamponade, and in some cases with tense ascites, puncture of these cavities is carried out on an emergency basis with further use of the contents for diagnosis. The presence of intestinal obstruction, bleeding or organ perforation also often requires emergency surgical treatment. When neurological symptoms develop against the background of the location of the tumor formation in the structures of the brain or spinal cord, chemotherapy is urgently started, and, if indicated, neurosurgical decompression measures are started [1].
Currently, for the treatment of NHL, risk-adapted polychemotherapy programs (PCT) are used, varying in intensity, duration, taking into account the nature of the tumor (T- or B-series, degree of maturity). For example, in the case of mature cell B-NHL, intensification of the starting blocks of chemotherapy is extremely important, and in case of lymphoblastic lymphomas from progenitor cells, long-term treatment with further maintenance therapy is used [27].
An integral aspect of treatment for NHL, especially B-NHL, is timing. For example, the B-NHL-BFM (Berlin-Frankfurt-Munster) 90/95 protocol (B-NHL-BFM 90/95) recommends maintaining an interval between courses of no more than 3 weeks [28]. Often this rule is violated, mainly due to the development of complications, which worsens the results of treatment.
For the treatment of mature cell B-NHL in children, effective protocols B-NHL-BFM 90, FAB (France-America-Britain, France-America-Britain)-2006 and their more modern modifications have been developed [29]. The ability to use a single treatment program for this group of hemoblastoses is determined by a similar immunophenotype (CD10, CD19, CD20, CD22), high Ki-67 levels (which determines good sensitivity to cytostatic therapy). The Russian Federation also uses the combined immunochemotherapy program B-NHL-2004m, which is a modification of B-NHL-BFM90/95, which involves reducing the dose of methotrexate to 1 g/m2 in the first and second blocks for patients with stages III–IV and adding rituximab in the first 4 blocks [30]. In the new version of this protocol (B-NHL-2010m), the criteria for stratifying patients into risk groups have been improved. All of these programs consist of a cytoreductive prephase and further cytoreductive and consolidative blocks using high-dose methotrexate and cytarabine, as well as cyclophosphamide, vincristine, dexamethasone and etoposide. Maintenance therapy is not required for diseases of this group. The duration of treatment is from 2 to 5 months. If treatment is ineffective, second-line therapy is carried out with courses of ICE (ifosfamide, carboplatin, etoposide; ifosfamide, carboplatin, etoposide), DHAP (dexamethasone, high dose cytarabine, cisplatin); the issue of hematopoietic stem cell transplantation is being decided. however, repeated remission is not always achieved and is often short-term [31]. The five-year overall survival rate for patients with early stages of the disease is close to 100%, and for late stages it is about 85% [21].
MVBCL differs from other B-NHL in its clinical picture (as a rule, it is localized in the mediastinum, quickly reaches large volumes, compresses vital structures), morphology and immunophenotype, and therefore standard therapy for B-NHL is ineffective for it [32]. Currently, attempts are being made to improve the results of therapy using the DA-R-EPOCH immunochemotherapy program (dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, doxo-rubicin; rituximab, etoposide, prednisolone, vincristine, cyclophosphamide, doxorubicin with dose regulation). If there is a residual lesion that is determined to be active by positron emission tomography, local radiation therapy is considered [31].
The main agents in PCT for lymphoblastic lymphomas/leukemia (protocols ALL – acute lymphoblastic leukemia: mBFM90/95, ALL IC-BFM 2002) are anthracycline antibiotics, vincristine, cyclophosphamide, antimetabolites (mercaptopurine, methotrexate), prednisolone and L-asparaginase. In this case, methotrexate is used in high doses (up to 5000 mg/m2) depending on the origin of the tumor, stage and prognostic risk group [33]. Of the new drugs included in the therapy of lymphoblastic lymphomas/leukemia, it is necessary to highlight clofarabine, as well as nelarabine (the latter is applicable to T cells) [34]. Treatment is long-term (up to 30 months) and includes phases of induction, consolidation, reinduction and further maintenance therapy. In case of initial damage to the central nervous system, cranial irradiation is used. In addition to systemic chemotherapy, endolumbar prophylaxis/therapy of neuroleukemia is carried out. For the treatment of relapses, gemcitabine, nelarabine, vinorelbine, ICE courses (ifosfamide, carboplatin, etoposide; ifosfamide, carboplatin, etoposide), etc. are used, but the prognosis for this group of patients remains unfavorable [35]. To secure the second remission, allogeneic bone marrow transplantation is used [31].
ALCL is the most common tumor of the group of peripheral T-cell lymphomas [5]. There is currently no uniform standard of treatment for ALCL. Various programs are used that are used for other types of NHL (B-NHL, lymphoblastic lymphomas, taking into account stratification by risk groups, depending on the activity of lactate dehydrogenase, stage of the disease, expression of ALK and CD8, the presence of extranodal lesions) [36]. The ALCL-BFM protocol (Berlin–Frankfurt–Münster) 2012 has been developed. Targeted therapy for this disease includes herbimycin A and 17-AAG (anti-NPM-ALK drugs), but the possibility of developing resistance to them should be taken into account [37]. In addition, in relation to ALK-positive ALCL, the transfer of ALK-NPM suppressors, Jak3 (Janus kinase), STAT3 (Signal Transducer and Activator of Transcription) by adenovirus is being studied [38]. As with all CD30+ tumors, brentuximab can be used; Crizotinib is also used for ALK+ ALCL [39, 40]. A radioconjugate, a monoclonal anti-CD25 antibody conjugated to 90-yttrium, is applicable to this type of tumor [25]. In case of disease relapse, there is a high probability of repeated remission when performing second-line chemotherapy and auto- or allogeneic hematopoietic stem cell transplantation [41]. In general, it can be noted that ALCL are quite sensitive to therapy, but the relapse rate for this disease is high [42].
Thanks to studies of cell receptors of differentiation clusters, which have become targets for specific monoclonal antibodies, targeted therapy is actively developing [39, 40]. In the treatment of NHL from peripheral B cells, rituximab (an anti-CD20 antibody) began to be used, which made it possible to reduce the dose of methotrexate, thereby reducing its side effects [43]. In addition to complement-mediated lysis of CD+ cells, rituximab enhances the cytostatic effect of doxorubicin, vinblastine, and glucocorticosteroids, and stimulates apoptosis by increasing Ca2+ ions in the cell and activating tyrosine kinases [44, 45]. The use in pediatric practice of a specific 26S proteasome inhibitor, bortezomib, has begun, which activates apoptosis of tumor cells and increases their sensitivity to chemotherapy and radiation therapy [46]. Brentuximab vedotin is used in CD30-positive lymphomas, particularly ALCL, Hodgkin lymphoma and primary mediastinal large B-cell lymphoma [47]. The therapeutic potential of epratuzumab (anti-CD22 antibody) and crizotinib (ALK tyrosine kinase inhibitor) are being studied [48].
Recently, the Children's Oncology Group began a clinical trial on the use of a new drug, ibritumomab tiuxetan (a 90-yttrium radioimmunoconjugate) in the treatment of B-NHL along with PCT and rituximab [49].
The surgical method in the treatment of NHL is not used as an independent method. Invasive interventions are required to diagnose the disease (biopsy) and if necessary to treat complications, as well as in some cases to remove residual formation [29].
Radiation therapy has limited use: as prophylaxis and treatment of central nervous system lesions in acute lymphoblastic leukemia/progenitor cell lymphoma, and also sometimes in primary mediastinal large B-cell lymphoma [50].
Patients with NHL require comprehensive accompanying therapy, which can be provided in large centers. For the prevention and treatment of emergency conditions, the availability of surgical, neurosurgical and resuscitation services, constant monitoring of vital functions and laboratory parameters are necessary. By creating aseptic conditions, regularly monitoring the flora of the department, and using antibacterial therapy, infections are prevented and treated.
In case of expected development of cytopenia, hematopoiesis stimulants may be used [51]. Against the background of aggressive chemotherapy, damage to the mucous membrane of the gastrointestinal tract is often observed, incl. severe oral mucositis. Currently, to treat this condition, a number of hygienic measures are used to care for the oral cavity, and, if necessary, parenteral nutrition. To prevent tumor lysis syndrome, infusion therapy is prescribed in the mode of hyperhydration with forced diuresis, and hypericemic drugs [52].
Conclusion
Currently, patients with NHL have a favorable prognosis for life and health: overall survival for non-advanced stages approaches 100%, however, therapy is accompanied by severe complications, sometimes posing a risk to life, and survival for stages 3–4 is still unsatisfactory . The prospects for treatment are largely determined by studying the genetic and histochemical nature of this disease. This will make it possible to synthesize new drugs, the use of which will increase the effectiveness of treatment and reduce the risk and severity of complications. Active research work on their development is being carried out in the largest medical centers of the Russian Federation and the world, which gives hope for an improvement in the situation in the coming years.
Methods for diagnosing lymphomas in children and adolescents
If a child experiences any of the complaints described above, you should immediately contact your pediatrician. If the child's medical history, a thorough examination, the result of a clinical blood test, as well as an ultrasound and/or x-ray examination suggest non-Hodgkin's lymphoma, the child is referred to a specialized pediatric oncology and hematology clinic.
A comprehensive examination is carried out in a specialized hospital:
- Tumor tissue analysis: examination of a diseased lymph node or other diseased tissue. Samples of the material are obtained surgically. The tumor tissue is sent for cytological, immunological and genetic tests. Based on the results of these studies, we can say for sure whether the child has contracted non-Hodgkin lymphoma, and if so, what type of lymphoma it is.
- Determination of the prevalence of the disease in the body: ultrasound examination of the abdominal organs, retroperitoneal space and pelvis, computed tomography of the chest, abdominal cavity and pelvis, magnetic resonance imaging of the brain and spinal cord (if indicated). To check whether tumor cells have entered the central nervous system, a lumbar puncture is performed - they take the cerebrospinal fluid and examine whether there are tumor cells in it or not. All children also undergo a bone marrow puncture to find out whether malignant cells have entered it or not.
- To assess heart function, electrocardiography and echocardiography are performed.
- Comprehensive laboratory tests: clinical blood tests, urine tests, biochemical blood test with assessment of kidney and liver function, determination of uric acid, electrolytes, lactate dehydrogenase (LDH), study of the blood coagulation system (coagulogram), determination of blood group and Rh factor.
Modern treatment programs for non-Hodgkin's lymphomas in children are based on an individual approach, taking into account various morphological and clinical variants of the disease.
Diagnosis of diffuse large cell lymphoma
The diagnosis of non-Hodgkin lymphoma is made on the basis of histological and immunohistochemical examination of tumor tissue. In order to obtain material, an incisional or excisional biopsy of the lymph nodes is performed. In addition, molecular genetic and immunophenotypic studies are performed, which will help determine the type of tumor, the presence of certain genetic changes and select the optimal treatment method.
To determine the stage of lymphoma, the following studies are performed:
- Trephine biopsy of bone marrow.
- Radiation diagnostic methods - ultrasound, CT, PET-CT, MRI.
- A number of laboratory tests are also prescribed - a complete blood count, determination of markers of parenteral hepatitis, HIV testing, biochemical studies, etc.
General principles of treatment of non-Hodgkin lymphomas
- For stages I and II of the disease, less intensive chemotherapy is used.
- For all types of NHL in children, prevention of damage to the central nervous system is mandatory.
- During intensive program polychemotherapy of mature cell lymphomas in children, radiation therapy is not indicated.
- Polychemotherapy is carried out against the background of a complex of adequate accompanying therapy.
Causes of NHL
The root cause of the development of the oncological process is currently unclear. There are factors that provoke the occurrence of the disease:
- viral and bacterial infections (mainly Epstein-Barr virus, HIV, hepatitis virus, H. pylori and other infectious agents);
- prolonged contact with carcinogenic substances;
- taking cytostatics;
- episodes of radioactive exposure;
- history of autoimmune diseases (systemic lupus erythematosus, thyroiditis, multiple sclerosis);
- genetic (congenital) disorders (Klinefelter syndrome);
- family history (presence of the disease in close relatives).
Treatment of mature T- and B-cell lymphomas
For the treatment of mature cell lymphomas, strict but short-term treatment (up to six months) is used using high-dose chemotherapy and immunotherapy (Fig. 2).
Treatment is carried out in short intensive courses - from 2 to 6. Their number depends on the stage of the disease and the risk group of the child. To determine the risk group, parameters such as the radicality of the operation (if any), the size and location of the tumor, the level of LDH in the blood and damage to the bone marrow and central nervous system are taken into account.
For the treatment of mature B-cell lymphomas, the cells of which express the CD20 antigen, the targeted drug rituximab (Mabthera, Acellbia) is used.
Rice. 2. NHL-BFM protocol for the treatment of mature B-cell lymphomas
Treatment of lymphoblastic lymphomas from T- and B-precursors
Treatment of children with lymphoblastic lymphoma is long-term, continuous for 2 years. It consists of several successive phases: prophase, induction - protocol I, consolidation - protocol M, reinduction - protocol II, prevention of damage to the central nervous system. Rice. 3.
To prevent damage to the central nervous system, the introduction of chemotherapy into the spinal canal and radiation therapy are used. Maintenance therapy is carried out for 1.5 years.
The intensity of the treatment program depends on the stage of the disease.
Rice. 3. NHL-BFM protocol for the treatment of lymphoblastic lymphomas from T- and B-precursors
Prognosis and prevention of large cell lymphoma
The prognosis for diffuse large B cell lymphoma depends on the IPI score. The higher the score, the worse the prognosis. For patients with a score of 4-5 (high risk), the five-year survival rate ranges from 31%. At low risks, the five-year survival rate is about 91%.
As for specific prevention, it does not exist today, and all recommendations for minimizing the risk of the disease boil down to maintaining a healthy lifestyle and proper nutrition.
Book a consultation 24 hours a day
+7+7+78
Clinical observation for NHL
Dynamic observation of children and adolescents is carried out for at least 3 years after completion of the treatment program.
In the first 3 months, the patient is examined every month, in the next 9 months - every quarter, then every six months.
The examination includes an examination of the patient with an assessment of complaints, clinical and biochemical blood tests with determination of LDH, ultrasound of the primary lesion, chest X-ray, and CT/MRI is used if indicated.
In recent years, whole body PET/CT with glucose has become widespread for dynamic monitoring of cured patients for the purpose of early diagnosis of relapse.