Benign lung tumors are a collective name for neoplasms of various origins, histological structure and localization. They can develop asymptomatically or make themselves felt by coughing, hemoptysis, and shortness of breath. In most cases, the treatment of such formations is surgical.
Classification of neoplasms
Benign lung tumors can develop from various types of tissue:
- bronchial epithelium (polyps, adenomas, cylindromas);
- neuroectodermal structures (neurinoma, neurofibroma);
- germinal tissues (congenital - teratoma, hamartoma);
- mesodermal tissues (fibromas, leiomyomas, lymphangiomas).
Prices for paid services
| Thoracic surgery | price, rub. |
| Drainage of the pleural cavity by endoscopic method Histological examination is paid additionally | 3 900 |
| Transthoracic biopsy Histological examination is paid additionally | 4 800 |
| Biopsy (needle) of the lung or mediastinal formations Histological examination is paid additionally | 5 500 |
| Open biopsy of the lung, mediastinal formations Histological examination is paid additionally | 21 230 |
| Endoprosthesis replacement of the trachea and bronchi with silicone prostheses | 41 360 |
| Drainage of moderate lung abscess with subsequent treatment | 5 500 |
| Sanitation of the pleural cavity with drugs for purulent diseases (1 procedure) | 4 800 |
| Diagnostic thoracoscopy | 11 770 |
| Video-assisted thoracoscopic splanchiectomy (one side) | 24 970 |
| Videomediastinoscopy | 22 000 |
| Video thoracoscopic lung biopsy Histological examination is paid additionally | 22 000 |
| Video thoracoscopic pleurectomy Histological examination is paid additionally | 26 400 |
| Video thoracoscopic pleurectomy with spraying of sclerosing agents Histological examination is paid additionally | 33 770 |
| Video-assisted thoracoscopic bullectomy using disposable staplers | 41 360 |
| Video thoracoscopic removal of peripheral lung formations Histological examination is paid additionally | 26 400 |
| Video thoracoscopic removal of mediastinal formations Histological examination is paid additionally | 32 230 |
| Microthoracotomy with video support and the use of reusable staplers | 22 000 |
| Pleurectomy Histological examination is paid additionally | 22 000 |
| Pleurectomy with lung decortication Histological examination is paid additionally | 32 230 |
| Regional resection of the lung Histological examination is paid additionally | 22 000 |
| Removal of a lung tumor (atypical resection) Histological examination is paid additionally | 26 400 |
| Removal of round peripheral lung formations Histological examination is paid additionally | 26 400 |
| Reduction of lung volume in patients with COPD, macrobullous or diffuse pulmonary emphysema | 65 890 |
| Decortication of the lung | 36 630 |
| Lobectomy category 1 | 41 030 |
| Lobectomy category 2 | 48 400 |
| Bilobectomy | 48 400 |
| Pneumonectomy Histological examination is paid additionally | 48 400 |
| Pneumonectomy with wedge resection of the tracheal bifurcation Histological examination is paid additionally | 58 630 |
| Pneumonectomy with circular resection of the tracheal bifurcation Histological examination is paid additionally | 58 630 |
| Circular resection of the trachea for neoplasms and cicatricial stenoses Histological examination is paid additionally | 77 660 |
| Chest resection | 26 400 |
| Surgery for mediastinal tumors Histological examination is paid additionally | 61 600 |
| Thoracoplasty | 44 000 |
| Embolization of bronchial arteries for pulmonary hemorrhage and/or hemoptysis | 22 000 |
| Therapeutic and diagnostic thoracoscopy, administration of drugs for the purpose of pleurodesis | 22 000 |
| Therapeutic and diagnostic video thoracoscopy | 23 430 |
| Therapeutic and diagnostic video thoracoscopy, administration of drugs for the purpose of pleurodesis | 26 400 |
| Drainage of the pleural cavity and pleurodesis | 17 600 |
| Videothoracoscopy, drainage of the pleural cavity and pleurodesis | 26 400 |
| Videothoracoscopy, pleural biopsy, drainage of the pleural cavity and pleurodesis Histological examination is paid additionally | 27 830 |
The most common benign lung tumors are:
- Bronchial adenoma is a glandular neoplasm up to 2-3 cm in size, with a tendency to malignancy.
- Hamartoma is of embryonic origin and consists of elements of embryonic tissue. It has a round shape and a smooth surface. Slowly grows, rarely degenerates into cancer.
- Papilloma is a formation of connective tissue stroma with multiple papillary outgrowths. It grows endobronchially, mainly in large bronchi.
- Fibroma is a benign formation 2–3 cm in size, consisting of connective tissue. It can reach gigantic sizes and is not prone to malignancy.
- Lipoma is a tumor of adipose tissue. It rarely forms in the lungs, grows slowly, and does not tend to degenerate into malignant.
- Leiomyoma - develops from smooth muscle fibers of blood vessels or bronchial walls. It grows slowly.
- Vascular neoplasms have a round shape, a dense or densely elastic consistency, and are surrounded by a connective tissue capsule.
- Neurogenic tumors are formed from nerve tissue and have the appearance of round, dense nodes with a distinct capsule.
Hamartoma - what is it: symptoms, diagnosis, treatment
Hamartoma is a benign neoplasm with a predominant localization in the lungs.
Retinal hamartoma and liver hamartoma are very rare. A benign tumor is a slowly growing neoplasm without spreading into neighboring tissues. Such tumors do not metastasize and do not become malignant. The severity of symptoms depends on the size and localization features.
What types of hamartomas are there?
- lipomatous (formed by a fatty component);
- chondromatous (the most common is chondromatous hamartoma of the lung);
- leiomyomatous (consists of smooth muscle fibers);
- angiomatous (predominance of the vascular component in the structure);
- organoid;
- fibromatous (fibromatous hamartoma of infants will be discussed in a separate section).
Neoplasms can be single or multiple.
Content
- 1. History
- 2 Epidemiology
- 3 Etiology and pathogenesis
- 4 Pathological anatomy
- 5 Classification 5.1 Based on tissue predominance
- 5.2 By number of tumors
- 5.3 By localization
- 7.1 X-ray of the lungs
Chondromatous hamartoma of the lung
Lung hamartoma is a congenital benign tumor consisting of lung tissue, vascular structures and cartilage. There are three types of disease: endobronchial hamartoma, anterior peripheral and posterior peripheral.
In most cases, the symptoms are mild. Typically, the diagnosis is made by MRI or X-ray results. Sometimes the patient may complain of cough, slight shortness of breath and pain in the chest area. The diagnosis is made taking into account the medical history, general condition and the results of instrumental studies. Additional examination methods include puncture, which allows you to determine the status of the tumor, and biopsy. In contrast to biliary hamartoma of the liver, the diagnosis of chondromatous hamartoma of the lung is made three times more often.
Pathological anatomy
Macroscopically, the hamartoma is most often round in shape, its surface is finely lumpy or smooth, and the consistency is dense-elastic or dense. There is no capsule. Clear demarcation from adjacent lung tissue. On the section, the tumor has a grayish or gray-yellow tint, and has a lobular appearance. The tumor includes foci of cartilage and is separated by fibrous layers; lime inclusions are often found (according to the book “Thoracic Surgery: A Guide for Doctors,” edited by L.N. Bisenkov).
In some cases, a hamartoma removed from its bed breaks up into separate lobules. The compressed alveoli form the tumor bed. There is no anatomical connection between them and the tumor, which explains the possibility of enucleating the hamartoma during surgery.
Microscopically, hyaline, and in rare cases, elastic cartilage, which has an atypical structure, is determined; there are layers of connective and adipose tissue around it. Areas of calcification or ossification are also detected. Sometimes there are lymphoid accumulations, smooth muscle fibers, and cyst-like cavities lined with epithelium.
Fibrous hamartoma in children
The neoplasm occurs during intrauterine development. The exact causes of fibrous hamartoma are still not understood. However, many doctors associate the development of pathology with heredity, gene mutations and the impact of unfavorable facts on the embryo.
Symptoms of the disease:
- periodic cough;
- mild chest pain;
- dyspnea;
- hemoptysis (manifests itself as the disease progresses).
The tumor is usually discovered accidentally after an x-ray or examination for another disease. To clarify the diagnosis, the doctor may prescribe an ultrasound, MRI, electroencephalographic study and fibrobronchoscopy.
Treatment of fibrous hamartoma in children consists of constant medical supervision, symptomatic therapy (for exacerbation of symptoms) and surgery (for progression of the disease).
Pathogenesis
A hamartoma is formed as a result of a violation of cell development in the embryonic period and consists of various elements of embryonic tissues. The development of a tumor is associated with a violation of organ formation and tumor-like growth of tissue components around the future organ.
Despite the early formation of tumor sprouts in the embryonic period, hamartoma may not manifest itself until the patients reach adulthood. The neoplasm consists of the same elements as the organ itself, but is characterized by an incorrect arrangement of components and an unhealthy degree of differentiation. This is what distinguishes a hamartoma from a teratoma , which contains tissue buds that are foreign to a given organ.
Causes of hypothalamic hamartoma
This type of tumor is considered quite rare and difficult to diagnose and treat. Hypothalamic hamartoma manifests itself in the form of seizures, cognitive impairment and endocrinological disorders. Premature puberty is a characteristic symptom of the pathology.
The diagnosis is made based on the results of MRI, EEG (electroencephalography), neuropsychological testing, taking into account the general symptoms and complaints of the patient.
The main causes of hypothalamic hamartoma are genetic disorders and exposure to negative factors during fetal development (infections, stress and inflammatory diseases of the mother). The diagnosis is made to one in 200 thousand children.
On our website you can make a personal appointment with a doctor and get an answer to the question “hamartoma - what is it?”
Prevention
Due to the fact that the tumor-like node begins to form during embryonic development and is partly due to genetic factors, there is no specific prevention.
It is almost impossible to predict in advance at what stage of development a failure will occur. However, parents can make their contribution to the birth of a healthy baby. To do this, it is necessary to minimize all risks associated with the negative impact of the environment on the health of the expectant mother.
Parents are advised to adhere to a healthy lifestyle, give up bad habits, and unquestioningly follow the instructions of the attending physician. Particular care should be taken when taking medications, especially during pregnancy.
Only with the right organizational approach to bearing and giving birth to a baby can the risk of developing pathology be significantly reduced, even with a genetic predisposition to neoplasms.
Treatment of the disease
Lung hamartoma. If the disease does not progress, the patient is recommended to be constantly monitored by a pulmonologist or therapist. In case of tumor growth, surgical intervention is indicated. The neoplasm is removed by exfoliation of lung tissue or by resection. The decision in this case is made by the doctor.
Hypothalamic hamartoma. Treatment of the tumor is long-term, including the use of anticonvulsants and agonists to luteinizing hormone receptors. The operation is performed for special indications.
Asymptomatic breast hamartoma requires constant medical supervision. Removal of a breast hamartoma is recommended if the tumor grows and abnormal biopsy results are obtained. Lumpectomy is an operation to remove a tumor, which is performed under general anesthesia. The patient makes a small incision on the chest, through which a probe connected to a vacuum is inserted and the tumor is removed. The surgical intervention is considered minimally invasive with a minimum of complications.
Related services: Computed tomography Magnetic resonance imaging
Instrumental research
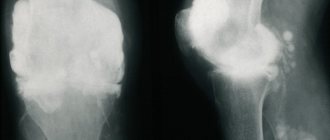
X-ray picture of a large hamartoma of the upper lobe (second segment) of the right lung
X-ray of the lungs
On radiographs, hamartomas with intrapulmonary localization have the appearance of single (much less often - multiple) spherical shadows (solitary pulmonary nodes) with clear, slightly wavy contours; with a lobular structure, the outlines of the tumor may be lumpy. Characteristic are calcareous inclusions located in the form of individual grains or in the form of a central conglomerate. Often the intensity of the shadow of the central part of the tumor is much higher than that of the marginal parts (a distinctive feature of hamartoma from other tumors). The pulmonary pattern around the hamartoma is usually unchanged. Sometimes there is a rim along the periphery (tumor bed). Characterized by the absence of changes in the root of the lung and pleural reactions. With long-term dynamic observation, the size of the hamartoma changes extremely slowly, but the intensity of calcareous deposits often progresses.
Due to the characteristics of radiological manifestations, 4 types of hamartomas are distinguished:
- Hamartomas with an irregular, spherical or oval shape, clear smooth or lumpy contours, having a very high shadow intensity, which decreases towards the periphery of the hamartoma. Characteristic are point, spotty and linear calcifications, clearly visible on direct and lateral radiographs, which merge into a single conglomerate.
- Hamartomas of medium intensity, having sharply defined smooth or lumpy contours and chaotic deposition of lumps of lime in the thickness of the tumor.
- Hamartomas with single or multiple foci of calcification located both in the thickness of the hamartoma and along its periphery.
- Hamartomas without calcification.
Endobronchial hamartomas are manifested by direct (spherical tumor-like formation in the lumen of the bronchus with smooth and clear contours on X-ray tomography) and indirect signs (various radiological manifestations of bronchial obstruction: hypoventilation, atelectasis or bloating, pendular displacement of the mediastinum, secondary bronchiectasis).
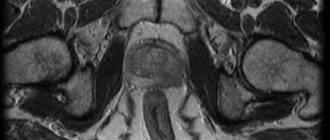
Computed tomography of the chest
CT image of a large hamartoma of the upper lobe (second segment) of the right lung.
The main advantage of computed tomography over plain chest radiography in examining patients with pulmonary hamartoma is the possibility of a more detailed assessment of the internal architecture of the tumor due to obtaining thin sections. In this regard, calcium and fat inclusions are better visualized with computed tomography than with radiography.
When computed tomography of the chest organs, hamartomas of all histological varieties are differentiated in the form of an oval-shaped volumetric formation with clear contours of various diameters, located against the background of unchanged lung tissue without reaction of the nearby interlobar or costal pleura. In approximately half of the cases, the structure of the hamartoma is heterogeneous: either due to centrally located areas of calcification (in 15-30%), or due to areas of density reduced to −130 (adipose tissue, in 34-50%). The combination of fat and calcium inclusions in one tumor is a characteristic sign of hamartoma. The frequency of calcification increases with the size of the hamartoma: from 10% for tumors less than 2 cm to 75% for hamartomas larger than 5 cm. When the tumor is located in the mantle part of the lung, it has emphasized contours and a smooth surface, and when the hamartoma is localized in the thickness of the lung tissue, it is removed from the root, the pole has emphasized contours and a smooth surface, while the pole facing the root of the lung remains clear, but acquires a wavy character due to many short fibrous strands extending into the lung tissue. The characteristic orientation of the long axis of a hamartoma is also noted: when this tumor is located in any part of the lung tissue, its long axis is always directed towards the root of the lung.
When computed tomography with bolus contrast enhancement of the image, a gradual increase in the density of the hamartoma is noted throughout all contrast phases. It is characteristic that in the arterial phase the increase in tissue density of the formation occurs by 57.2%, in the venous phase - by 26.4%.
Fiberoptic bronchoscopy
Fiberoptic bronchoscopy makes it possible to diagnose hamartoma in cases where it comes from the bronchial wall. Endobronchial hamartoma can be located on the walls of the bronchi or in the area of the bronchial “spur”, has a spherical or cone-shaped shape, whitish color and a wide base. The mucous membrane covering the hamartoma is not changed. On instrumental palpation, it has a stony density, which causes significant difficulties when taking a biopsy from the tumor.
Transbronchial ultrasound examination performed during fibrobronchoscopy allows for targeted transbronchial puncture biopsy of a hamartoma located near the bronchus. Cytological examination of the material obtained in this way makes it possible to clarify the diagnosis and determine further treatment tactics.
Ultrasound-guided transthoracic puncture
As a rule, ultrasound examination (ultrasound) is not used to detect pulmonary hamartomas. However, in the presence of a subpleural hamartoma adjacent to the chest wall, it is possible to visualize it during ultrasound examination with targeted puncture biopsy of the tumor through the chest wall under ultrasound guidance. Performing transthoracic puncture biopsy is also possible under the control of computed tomography.
Are there any complications?
Complications arise when nodules increase in size and begin to put pressure on nearby organs. A person experiences chest discomfort, depending on the location of the formation.
A single nodule in the lung tissue will not cause much harm to the body. If there are many such nodules and they grow, the size of the organ increases, and the volume of the lungs decreases. In the first years of abnormal development of compactions, the body manages to compensate for respiratory failure, but subsequently chronic lung failure appears.
The pathological development of hamartoma leads to dysfunction of the bronchi, trachea, and sometimes the gastrointestinal tract suffers. Obstructive pneumonia is considered a frequent complication: increased compaction interferes with normal air circulation.
Forecast
The prognosis for hamartoma is favorable. Hamartomas usually grow very slowly, but can reach gigantic sizes. Cases of malignancy of a hamartoma are very rare: the possibility of malignancy does not exceed 5-7%; some authors exclude this possibility altogether, doubting the reliability of the reported single observations of malignancy. Malignancy occurs both in the mesenchymal (chondrosarcoma, fibrosarcoma, liposarcoma) and epithelial component of the formation (adenocarcinoma, epidermoid cancer), with metastasis to the lymph nodes, pleura, liver, and spine.
Likely consequences
Despite its benign nature, the lack of timely removal is dangerous due to malignant transformation, the development of obstructive pneumonia, segmental or lobar atelectasis. In rare cases, the hamartoma rapidly increases in size, causing metastases to occur in the liver, spine and diaphragm.
If the pathology is started, the hamartochondroma degenerates into chondrosarcoma, liposarcoma, adenocarcinoma or fibrosarcoma. These malignant tumors are deadly for the patient.