When the cornea or sclera of the eye is damaged, with damage to only part of their thickness, we are talking about non-penetrating wounds. Such injuries account for more than half of all eye injuries, rarely affect visual function, and usually do not cause serious complications.
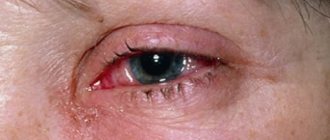
Microtraumas that cause superficial damage are usually the result of mild blows to the eye or punctures from some sharp objects. They lead to the formation of superficial erosion of epithelial tissues, causing in some cases traumatic keratitis. In addition, quite often, the occurrence of superficial damage is associated with the penetration of small foreign bodies into the eye - pebbles, ash, plant particles. They do not damage the eye capsule, but remain on the surface of the cornea or sclera. To detect them, due to their small size, side lighting and a binocular magnifying glass are required, or better yet, biomicroscopy.
It is very important to identify how deep the foreign body is located. So, if it is localized in layers close to the surface, photophobia may occur, lacrimation begins, and redness is noted (pericorneal injection), caused by irritation of the endings of the trigeminal nerve present in large numbers here.
Therapy of non-penetrating wounds
Removing foreign objects from the eye as quickly as possible is mandatory. After all, their prolonged stay inside, especially on the surface of the cornea, is often complicated by traumatic keratitis or a purulent ulcer occurs. Removal of superficial foreign objects is performed on an outpatient basis. Quite often, this requires only a cotton swab and a few drops of local anesthesia (alcaine 0.5%). Particles that get inside the layers of the cornea and penetrate into the middle are neutralized with a grooved chisel, special. with a spear or a regular injection needle. But, when a foreign body has penetrated deep, it is advisable to remove it surgically, using a microscope. Since there is a high risk of opening the anterior chamber. Metal particles are often removed using a magnet, cutting the surface layers of the cornea above them, as required.
Removal of foreign particles is necessarily accompanied by the application of an aseptic bandage and the administration of appropriate therapy with disinfectant eye drops. In addition, it is recommended to add ointments with antibiotics or sulfonamides. Corneregel (which improves epithelization) and methylene blue can be used.
If foreign particles get into the deep layers of the cornea, they should be removed only by an ophthalmologist, especially when the eye is the only one remaining.
Penetrating wounds
The species diversity of penetrating injuries to the organ of vision is quite large, so they are divided into three groups with seriously different injuries. The largest percentage of penetrating wounds occurs in lesions in which the wounding object cuts the outer eye membranes (sclera and cornea) completely. Such damage is considered extremely dangerous, since it can seriously reduce the visual functions of the eye (often to the point of blindness) or cause the death of a paired healthy eye.
Systematization of penetrating wounds
In terms of species, penetrating eye lesions are usually divided into:
1. By localization. Corneal lesions, limbal lesions, corneal-scleral lesions, scleral lesions.
2. In depth. Highlight:
- Damage with a wound channel in the cornea or sclera, of varying depths in the eye cavity, without going beyond its limits.
- Penetrating wounds, with the entrance and exit of the wound channel beyond the boundaries of the eye cavity.
- Destruction of the eyeball is its destruction with irreversible loss of vision function.
3. By size . Lesions of small size (up to 3mm), medium size (4-6mm), large size (over 6mm).
4. In form. Lesions are linear, irregular, punctured, star-shaped, torn.
There are also wounds that are adapted (with edges that fit tightly) and gaping.
Symptoms and diagnosis
Up to 40% of penetrating wounds occur with damage to the lens, at least 30% of wounds cause pinching or prolapse of the iris, approximately 20% of wounds cause hemorrhages in the vitreous body or anterior chamber and the development of endophthalmitis due to infection. In 30% of cases, the foreign body remains inside the eye.
Diagnosis of penetrating wounds must begin with a history taking into account the medico-legal consequences of existing eye damage. Often, victims (especially children) distort or conceal real information about the causes and mechanism of the lesion. But, as experience shows, the most common are domestic, sports and industrial causes of injuries. The size of the wounding object, its kinetic energy and the speed of impact usually determine the severity of the damage.
In all (with rare exceptions) cases of penetrating wounds, X-ray examination, ultrasound, MRI and computed tomography are mandatory. This will allow you to accurately determine the degree of damage and the absence (presence) of a foreign body that has penetrated inside.
The basis of diagnosis is the identification of characteristic signs, absolute or relative in importance.
The absolute characteristics include:
- Penetrating wounds of the sclera or cornea;
- Prolapse of the inner eye membranes and vitreous body into the wound;
- Leakage of intraocular fluid through the corneal wound (test with fluorescein);
- Identification of the wound channel through the internal structures of the eye;
- Detection of a foreign body inside;
- Air in the vitreous body.
Relative signs are:
- Depth of the anterior chamber (shallowness - when the cornea is injured, greater depth - when the sclera is injured, uneven depth - when the iris and sclera are simultaneously damaged);
- Hypotension;
- The occurrence of hemorrhage;
- Tears along the pupillary edge, the shape of the pupil is changed;
- Tear and separation of the iris;
- Dislocation or subluxation of the lens;
- Traumatic cataract.
Penetrating wounds are diagnosed when even one absolute sign is identified.
X-ray examination of a bullet wound
The goal is to determine the damage itself and its volume, assess the presence of bone fragments, their displacement relative to the fracture zone, identify foreign bodies, determine their quantity, their relationship to anatomical structures, diagnose gunshot osteomyelitis, arthritis, and gas infection.
Using SCT, you can obtain comprehensive diagnostic information about the extent of the damage, find and identify the exact localization of any foreign body (for example, shot, fragments) in absolutely any part of the body. In case of extensive lesions (limbs, torso), it is possible to conduct a detailed scan of the entire body at once and, using the scans obtained, determine not only the presence of bullets and shrapnel, but also give a detailed description of damage to bones, joints, internal organs, answer the question of the presence of internal hidden bleeding, development of pneumothorax, hydrothorax, and so on. SCT is especially indispensable for wounds with shot of various diameters, when the number of foreign bodies can reach several dozen.
First aid
In order to provide first aid, it is extremely important for doctors to know the distinctive signs of penetrating eye lesions. So, without fail, it is necessary:
- Apply a sterile bandage to the victim and inject an antibiotic and tetanus toxoid intramuscularly.
- If possible, immediately send the victim to a specialized hospital, strictly lying down.
It is strictly forbidden to remove foreign bodies yourself (with the exception of particles on the surface of the eye tissue).
Lesions of the sclera and cornea
Penetrating lesions of the cornea are accompanied by a violation of its integrity. In this case, the wound can be localized centrally, equatorially or meridionally. The shape of wounds can be linear, patchy with smooth or torn edges, gaping, with tissue damage. Injury to the cornea quite often leads to leakage of intraocular fluid, then the anterior chamber loses its depth. Often, such injuries are accompanied by separation of the iris and its loss, damage to the lens (provoking cataracts) or the vitreous body (hemophthalmos occurs).
Treatment. The main goal of surgical treatment of penetrating corneal lesions is the maximum restoration of its anatomical structure to preserve the function of the organ.
To do this, deep sutures can be applied to 2/3 of the thickness of the cornea with a distance from the wound edge of 1 mm (nylon 10.00). After 1.5-2 months, these sutures are removed. Treatment of star-shaped wounds is carried out using the purse-string suture technique (a circular suture is made through the corners of the wound, tightening in the center), and additional interrupted sutures are applied to areas extending from the wound center. Prolapse of the iris requires its reduction and reposition, which is carried out after complete removal of impurities and treatment with an antibacterial solution.
The occurrence of traumatic cataracts after damage to the lens is treated by cataract extraction, replacing the anatomical lens with an intraocular lens. In the case of a crushed corneal wound without the possibility of matching its edges, a corneal transplant is recommended.
Complications
Post-traumatic synostosis (pathological fusion of “neighboring” bones) with significant dysfunction occurs due to comminuted fractures and the formation of massive calluses in adjacent bones (for example, the radius and ulna). In this regard, it is extremely important to identify and remove fragments that are located in the interosseous space.
A “false joint” from a gunshot fracture is formed more often than with ordinary fractures. This is due to insufficient bone formation and lack of normal consolidation due to wound infection.
Lesions of the sclera and iris-scleral region
Such injuries are almost never isolated, and their severity is determined by concomitant prolapse of the internal membranes, as well as hemorrhages.
Corneal-scleral lesions may be accompanied by loss/strangulation of the iris, ciliary body, and the occurrence of hyphema and hemophthalmos. Scleral lesions are usually accompanied by deepening of the anterior chamber, loss of the vitreous body or inner eye membranes; hyphema and hemophthalmos occur. Particularly serious damage to the sclera with tissue defects is associated with subconjunctival tears.
Treatment. Primary surgical treatment is performed under general anesthesia. Their main goal is to restore intraocular structures and the tightness of the eyeball. It is necessary to conduct an inspection of the scleral wound, trying to accurately determine the direction of the wound channel, its depth, as well as the degree of damage to the intraocular structures. These factors are decisive for the nature of surgical treatment. Based on the results of the audit, treatment is performed through the entrance wound or through additional incisions.
If the ciliary body or choroid falls out or is pinched in a wound, they are set back and sutures are placed after irrigation with an antibiotic solution to prevent inflammatory reactions or the development of infection.
Infection of a wound of the cornea and sclera causes acute iridocyclitis, endophthalmitis with the accumulation of foci of pus in the vitreous body, and in complicated cases - panophthalmitis with purulent inflammation of the eye structures.
All penetrating lesions require massive local treatment, which includes therapy with anti-inflammatory and antibacterial drugs and symptomatic treatment and raising the immune status of the eye.
Publications in the media
A gunshot wound is a particular type of combat surgical injury that occurs when the body is exposed to wounding projectiles from small arms and explosive ammunition. Regardless of the type of injury, a person who has received a combat surgical injury is called a wounded person.
Classification • By type of wounding projectile •• Bullet •• Fragmentation •• Mine-explosive • By quantity and location •• Isolated •• Multiple •• Combined • By severity •• Light •• Moderate severity •• Heavy •• Extremely severe • Should differentiate certain concepts of combat surgical trauma: mine-explosive wound and mine-explosive injury •• Mine-explosive wound (MBW) is the result of direct impact on the body of explosive ammunition in the affected area by a shock wave, accompanied by tissue destruction or separation of limb segments •• Mine -explosive injury - shielded damage that occurs when the main damaging factors of an explosion are exposed to the human body located in a shelter (the bottom of armored vehicles, a ship, etc.) • A wound caused by one wounding element within one anatomical area is isolated • A wound caused by several wounding elements within one anatomical area is called multiple • Injury to two or more anatomical areas (head, neck, chest, abdomen, pelvis, spine, limbs) is called combined.
Wound ballistics and morphology • The destructive effect of any firearm projectile whose flight speed exceeds 300 m/s is based on the formation of a temporary pulsating cavity (PPC) with zones of excess pressure along the periphery. The number and maximum amplitude of cavitations depend on the magnitude of the kinetic energy and shape of the wounding projectile, as well as on the stability of its flight. The kinetic energy of a wounding projectile is determined primarily by its flight speed and, to a lesser extent, by its mass. Accordingly, it is necessary to differentiate between wounds inflicted by low-velocity wounding projectiles (a bullet from a Makarov pistol, shot, etc.) and injuries received by high-velocity wounding projectiles (bullets from automatic rifled weapons). The energy given off by a wounding projectile when passing through tissue determines the nature of the damage and the morphology of the gunshot wound. • The morphological substrate of a gunshot wound is a gunshot wound that has an entrance, exit (if the wound is through) openings and a wound channel. The wound channel in many cases has a complex configuration and contours. In accordance with the anatomical and functional changes within the wound canal, three zones are distinguished: •• the zone of the immediate wound canal (or avulsion during MVR) •• the zone of primary necrosis •• the zone of secondary necrosis (formerly molecular concussion).
• The wound channel has an irregular broken course due to primary and secondary tissue deviation and is filled with tissue detritus, foreign bodies, blood clots, free bone fragments and those associated with the periosteum and muscles. The zone of primary necrosis is represented by tissues damaged as a result of deviation of the runway. The zone of secondary necrosis is represented by tissues damaged as a result of exposure to AFFF, as well as from secondary disorders of microcirculation and nervous trophism. The boundaries between these zones are very blurred and change depending on the stage of the wound process. This makes it difficult to carry out comprehensive local treatment in the early stages after injury. • A gunshot wound is always primarily contaminated with microbes. As a result of the phenomena of antagonism and synergy, a microbial association is formed in the wound, capable of vegetating and multiplying - wound microflora. Depending on the adequacy of the treatment and the capabilities of the body’s protective and adaptive forces, this microflora either contributes to the secondary cleansing of the wound or becomes a potential source of wound infection. The clinical picture of a gunshot wound is determined by the degree of damage to specific organs and systems, as well as the development of early and late complications (shock, blood loss, wound infection, traumatic disease).
Treatment. Injuries to specific organs are treated according to the principles adopted in the relevant medical specialties (neurosurgery, ENT, maxillofacial surgery, thoracic surgery, proctology, etc.). Local treatment of the gunshot wound itself, regardless of location, is carried out according to military field surgery schemes. The main element of local treatment of a gunshot wound is surgical debridement. • Surgical treatment is a surgical intervention (operation) aimed at removing non-viable tissue, preventing or treating purulent-infectious complications and creating favorable conditions for wound healing. Surgical treatment of a wound consists of three main elements: dissection of the wound, excision of all non-viable tissue (this removes tissue that is clearly necrotic or their viability is questionable) and restoration of the anatomical relationships in the wound. In accordance with the objectives, surgical treatment of the wound can be primary or secondary ••
Primary surgical treatment (PST) is the first surgical intervention performed according to primary indications for tissue damage itself. When a limb is torn off, amputation is performed according to the PSO type, without performing plastic surgery or suturing the stump. Depending on the timing of PSO, it is early (1st day), delayed (2nd day) and late (3rd day) after injury •• Secondary surgical debridement is a surgical intervention aimed at treating complications that have developed in the wound. The most common complications are progressive tissue necrosis and wound infection. Secondary surgical treatment of the wound may be the first operation on a wounded person if complications have developed in a previously untreated wound, or the second in cases where PSO has already been performed on the wound. • All gunshot wounds are divided into two groups: those subject to surgical treatment and those not subject to surgical treatment. Small superficial wounds, through bullet wounds with narrow entry and exit holes in the absence of signs of damage to a large blood vessel, and multiple small superficial blind wounds are not subject to surgical treatment. • The application of a primary suture as the final stage of surgical treatment of a gunshot wound is unacceptable. It can only be applied to wounds of the face, scalp, scrotum and penis, penetrating chest wounds with open pneumothorax and after laparotomy (only to the skin), joint wounds (only to the capsule). • Treatment of gunshot injuries to the extremities consists of the following elements: general treatment (pain relief, anti-shock, antibacterial and restorative therapy, compensation for blood loss, etc.); local surgical treatment (PHO, external osteosynthesis); local conservative treatment. Local treatment involves regional intra-arterial infusion, dressings, and anti-inflammatory blockades. The blockade is carried out by introducing into the circumference of the wound a solution: 100 ml of 0.25% procaine, HA (90 mg of prednisolone), protease inhibitors (30,000 IU of aprotinin), broad-spectrum antibiotics. Abbreviations: TPP—temporary pulsating cavity, MVR—mine-explosive wound, PSW—primary surgical treatment (PST).
ICD-10 • Y22 Injury resulting from a discharge from a handgun of unspecified intent • Y23 Injury from a discharge from a rifle, shotgun, or large caliber firearm of unspecified intent • Y24 Injury from a discharge from another and unspecified firearm of unspecified intent
Injuries involving foreign bodies
Consistently collected history information is of great importance when a foreign body is suspected of remaining in the eye for developing treatment tactics. Due to a foreign body, corneal infiltrates may develop and post-traumatic keratitis may occur, leading to partial opacification of the cornea.
Extensive hyphema or hemophthalmos accompanying corneal injuries do not always make it possible to determine the course of the canal and the localization of the foreign body. Especially when it has passed the sclera beyond its visible part, it is almost impossible to identify the entrance hole.
The introduction of a large object leaves behind a gaping wound in the cornea or sclera, causing prolapse of the choroid, retina, and vitreous body of the patient's eye.
Diagnostics. Foreign bodies in the cornea, anterior chamber, lens, iris, vitreous body or fundus are determined during biomicroscopy and ophthalmoscopy.
To determine a foreign body that has penetrated inside the eye, X-ray localization is used using the Komberg-Baltin method, using an eye marker. This is an aluminum indicator prosthesis, which has a radius of curvature comparable to the radius of the cornea and a thickness of 5 mm. There is an 11mm hole in the center of the marker. At 0.5 mm from the edge of the central hole, reference points are marked on mutually perpendicular meridians. The indicator is installed after local anesthesia with alcaine and is positioned so that the visible marks are oriented towards the limbus at 12-3-6-9 o'clock.
Baltin-Polyak meters are used to interpret X-ray images. They are superimposed on top of photographs of three projections of the eye. Based on the direct projection taken, the meridian of the foreign body and its distance to the ocular axis are determined. Lateral and axial projections show the distance from the foreign body to the limbus in the direction of the equator along the sclera. The method is preferable for visualizing small metallic foreign bodies while maintaining the turgor of the eye tissues, without persistent hypotension due to gaping wounds of the outer membranes. It makes it possible to determine the depth of the foreign body to plan the scope of surgical actions.
In the anterior region, the location of the foreign body is well determined by non-skeletal radiography using the Vogt method. It can only be performed 8 days after injury.
But modern research methods are considered the most informative - ultrasound (A-B) scanning and computed tomography. These methods make it possible not only to find out the location of an object inside the eye, but they also identify complications arising from its penetration.
Treatment. Intraocular foreign bodies should be removed immediately. If it is localized superficially, certain instruments are used - needles, tweezers, spears. Removing deeply penetrated foreign bodies involves making linear cuts and removing it: with a magnet, if it is metal, or with a needle, if it is not magnetic.
The fragment of the anterior chamber is removed as follows: an incision is made above the foreign body and the tip of the magnet is inserted inside. The foreign object in the lens is removed with a magnet when the anterior chamber is opened. But if it is not magnetic, then it must be removed along with the lens.
Amagnetic foreign bodies are removed from the eye with serious difficulties. If they are identified in the area of the anterior part of the eye, the so-called anterior path is used to eliminate them.
Until recently, objects that had passed to the posterior part of the eye were removed only by the diascleral route - by making an incision in the sclera. Today, experts give primacy to the transvitreal route, when a magnetic tip or instrument for grasping an amaganite object is inserted through an incision in the ciliary body.
If a traumatic cataract or hemophthalmos occurs, at the first stage cataract extraction or vitrectomy is performed, and then the foreign body is removed under control. In the case of penetrating eye injuries, drug therapy is also required to prevent inflammation, the development of infection, hemorrhagic complications, secondary glaucoma, etc.
Gunshot damage.
WELCOME USERS OF AIR-GUN.RU
ATTENTION!!! Some materials used in this article may be contraindicated for pregnant women, the faint of heart, and the mentally ill... if you are one of them, please close the article and do not read.
We all love weapons... pneumatic, firearms, cold steel... and we all know very well that weapons are initially designed to kill. We won’t go into details.....but first of all, weapons maim and kill, and only then everything else)) In this article I want to talk about gunshot wounds. Types, signs, features, etc. This article may seem too harsh to some, but this is the “harsh” truth of life.
To write this article, materials from various sources were used, mainly lectures on forensic medicine.
So, let's begin……
FIREARMS.
A firearm is a specially designed and manufactured device intended to mechanically engage a target at a distance with a projectile that receives directional movement due to the energy of a powder or other charge.
Gunshot damage is damage caused by a shot from a firearm.
Firearms are divided into types (civilian, service, military), by barrel length (long-barreled, medium-barreled and short-barreled), and by barrel rifling (rifled, smooth-bore). A weapon with an internal bore diameter of 5–6 mm is called a small-caliber weapon, a medium-caliber weapon is 7–9 mm, and a large-caliber weapon is 10 mm or more.
A military weapon cartridge consists of a firearm projectile (bullet), a cartridge case, a powder charge and a primer. A cartridge for a hunting weapon consists of a brass, plastic or cardboard sleeve, a projectile covered with a wad, gunpowder covered with a cardboard spacer and wad, and a primer. The projectile in a hunting cartridge can be shot, buckshot, or special bullets. Hunting cartridges are loaded with black powder. Wads are made of felt, cardboard, plastic, etc. Caps in hunting cartridges are similar to combat ones.
Damaging factors of a shot
The damaging factors of a shot are divided into basic (bullet, shot, buckshot, wad, fragments of an exploding projectile) and additional (pre-bullet air, powder gases, soot, powder particles, microparticles from the barrel, primer, gun lubricant).
When a bullet impacts any object, secondary projectiles can form: fragments of an obstacle, fragments of clothing, fragments of bones. In some cases, the muzzle end and moving parts of the weapon, the butt, and fragments of an exploding weapon may be affected.
Due to its high speed and, therefore, high kinetic energy, a firearm projectile is capable of causing damage in any part of the external ballistic trajectory. Additional factors can cause damage only at a certain distance when leaving the barrel of a weapon. If the damage is caused within the reach of additional factors of the shot, the shot is said to be close, and beyond their influence, when the damage is caused only by the bullet, it is said to be not close.
Characteristics of a gunshot wound
In case of a gunshot injury, through, blind and tangential bullet wounds can form.
A through bullet wound is a wound that has an entrance and exit gunshot wound connected by a wound channel. Penetrating wounds arise from the action of a bullet with high kinetic energy, or when thin parts of the body or only soft tissue are wounded.
A typical entrance gunshot wound is small in size, round in shape, in its center there is a skin defect (minus tissue), which has the shape of a cone, the apex facing inward, the edges are uneven, with short radial tears in the surface layers of the skin, not extending beyond the wound zone, surrounding the defect. If a bullet is inserted into the body at an angle close to a straight line, then the width of the impact belt along its entire perimeter is the same and amounts to 1–3 mm. If a bullet is inserted into the body at an acute angle, then the belt will be wider on the side of the bullet’s flight, since in this place the contact area between the skin and the bullet is greatest. The belt of edema looks like a dark narrow strip along the edge of the skin wound. The outer diameter of the settling belt is approximately equal to the caliber of the firearm. The surface of the settling belt is contaminated with the metal of the bullet surface. Hence other names: pollution belt, metallization belt, wiping belt.
Exit gunshot wounds are more variable in shape, size and nature of the edges. They usually do not have a deposition band and a metallization band. The defect in the area of the exit wound is either absent or has the shape of a cone, with the apex facing outward.
The main distinguishing feature of an entry gunshot injury on the flat bones of the skull is a chip of the internal bone plate, forming a funnel-shaped defect, open in the direction of the bullet’s flight. The exit gunshot injury is characterized by a chip of the outer bone plate.
When a through wound is formed, it is necessary to differentiate the entrance hole from the exit hole. Differential diagnosis should be based on a comparative assessment of the entire set of morphological characteristics.
A blind wound is a bullet wound in which the gunshot remains in the body. Blind wounds are usually caused by bullets with low kinetic energy due to their low initial speed, unstable flight, design features leading to rapid destruction of bullets in tissues, large distance to the target, preliminary interaction of the bullet with an obstacle, damage to a large array of dense and soft tissues in the body , internal rebound, for example in the cranial cavity.
Tangential bullet wounds occur when the bullet does not penetrate the body and forms an open wound channel in the form of an elongated wound or abrasion. The entrance end of the wound is rounded, with a skin defect and small radial tears of the skin that do not extend beyond the semicircular deposition. The greatest depth of the wound is at its entrance end. The general shape of the wound is in the form of a groove, thinning towards the exit end.
Damage to tissue is accompanied by the bullet transferring part of its energy to them. The resulting sharp vibration of tissue increases damage along the wound channel and causes new ones in places remote from it. This effect is more pronounced when a bullet passes through a full stomach or brain (hydrodynamic effect).
Passing through clothing, skin and other formations, the bullet moves knocked out tissue along the wound channel. There is a “drift” of tissue into places unusual for the location.
Damage caused by bullets fired from modern samples of hand-held small-caliber combat firearms has certain morphological features: blind wounds are formed more often than with shots from medium-caliber weapons, a gunshot wound may contain many metal fragments of a destroyed fragmented bullet, exit gunshot wounds can be very extensive, and often represented by one or several small lesions. These damage features depend on the ability of bullets fired from these types of weapons to transfer all or almost all of their kinetic energy to the affected tissues. This is due to the high initial velocity of the bullet combined with its low stability in flight, since the center of gravity of the bullet is shifted towards its tail. As a result, the head of the bullet in flight makes rotational movements of large amplitude.
Types of shots
Shot at close range
When shot at close range, tissue damage is caused by the main and additional damaging factors.
Additional factors of a shot within close range have different effects depending on the distance between the muzzle of the weapon and the target. In this regard, a point-blank shot is distinguished, when the muzzle of the weapon at the moment of the shot is in contact with the surface of clothing or a damaged part of the body, and three conditional zones, when the muzzle at the moment of the shot is at some distance from the target object.
I – zone of predominant mechanical action of powder gases.
II – zone of pronounced action of shot soot, powder grains and metal particles.
III – zone of deposition of powder grains and metal particles.
In the first zone of a close shot, the entrance gunshot wound is formed due to the explosive and bruising effect of the powder gases and the penetrating effect of the bullet. The edges of the wound may have tears. If there are no breaks, then the wound is surrounded by a wide ring-shaped deposition (the bruising effect of gases). The action of powder gases in zone I is limited to skin damage and does not extend into the depth of the wound channel. Around the wound there is intense deposition of dark gray, almost black soot and powder grains. The area where soot and powder grains are deposited increases as the distance from the muzzle of the weapon to the target at the time of the shot increases. According to the area of soot deposition, the thermal effect of powder gases may manifest itself in the form of shedding of vellus hair or clothing fibers. Around the entrance wound, when using ultraviolet rays, splashes of gun lubricant can be detected in the form of multiple luminescent small spots. The length of zone I depends on the power of the weapon used: for a Makarov pistol this zone is about 1 cm, for a Kalashnikov assault rifle with a caliber of 7.62 mm - up to 3 cm, for a rifle - about 5 cm, AK-74U - up to 12–15 cm.
In zone II of a close shot, the wound is formed only by the bullet. Soot, powder grains, metal particles, and splashes of gun lubricant are deposited around the entrance wound. As the distance from the muzzle of the weapon barrel to the target object increases, the area of deposition of additional shot factors increases, and the intensity of the color of the soot decreases. For many modern handguns II, the close shot zone extends to 25–35 cm. Soot and powder grains fly in the direction opposite to the direction of the shot, settling within a radius of 30–50 cm, and sometimes 100 cm.
In zone III of a close shot, the wound is formed only by the bullet. Powder grains and metal particles are deposited around it. When fired from a Makarov pistol, these particles can be detected at a great distance - up to 150 cm from the muzzle, from a Kalashnikov assault rifle - up to 200 cm, from a rifle - up to 250 cm. On a horizontal surface, particles are found at a distance of up to 6-8 m. As the distance increases, the number of powder grains and metal particles reaching the target becomes smaller and smaller. At extreme distances, as a rule, single particles are detected.
Shot at point blank range
When fired at point-blank range at a right angle to the surface of the body, the pre-bullet air and part of the powder gases, acting compactly, pierce the skin, expand in all directions in the initial part of the wound channel, peel off the skin and forcefully press it to the muzzle end of the weapon, forming a bruise in the form of imprint, stamp. Sometimes skin breaks occur. Along with the powder gases, soot, powder and metal particles rush into the wound channel. Penetrating into the wound channel, powder gases interact with the blood and form oxy- and carboxyhemoglobin (bright red color of tissue). If powder gases reach hollow organs, then, expanding sharply, they cause extensive ruptures of internal organs.
Signs of being shot at point-blank range:
1) the entrance hole on clothing and skin is star-shaped, less often angular or round in shape;
2) a large skin defect exceeding the caliber of a firearm projectile, as a result of the penetrating effect of powder gases;
3) detachment of the skin along the edges of the entrance gunshot wound, ruptures of the edges of the skin as a result of the penetration of powder gases under the skin and their explosive action;
4) an abrasion or bruise in the form of a stamp - an imprint of the muzzle end of a weapon (stamp mark) due to the insertion of skin on the barrel, peeled off by powder gases that have penetrated and expanded under the skin (an absolute sign);
5) extensive ruptures of internal organs as a consequence of the explosive action of powder gases that penetrated cavities or hollow organs;
6) ruptures of the skin in the area of the exit wound when thin parts of the body are damaged (fingers, hand, forearm, lower leg, foot) as a result of the explosive action of powder gases;
7) the presence of soot only at the edges of the entrance wound and in the depths of the wound channel due to the dense stop, making it impossible for them to penetrate into the environment;
 light red coloration of the muscles in the area of the entrance wound due to the chemical action of powder gases, which causes the formation of oxy- and carboxyhemoglobin.
light red coloration of the muscles in the area of the entrance wound due to the chemical action of powder gases, which causes the formation of oxy- and carboxyhemoglobin.
When fired at point-blank range at a certain angle to the body surface, some of the powder gases, soot, and powder particles have a damaging effect on the surface of the skin near the wound, which leads to the formation of one-sided skin tears and eccentric deposition of soot and powder particles near the edges of the entrance gunshot wound.
Shot wound
After a shot, the shot charge usually flies as a single compact mass over a distance of one meter, then individual pellets begin to separate from it, and after 2–5 m the shot charge completely disintegrates. The flight range of the shot is 200–400 m. The degree of dispersion of the shot shell determines the characteristics of shot damage at different shot distances.
A point-blank shot results in a significant amount of internal damage, such as complete destruction of the head. When fired at point-blank range, extensive skin defects, an imprint of the muzzle end of the 2nd barrel, soot in the depths of the wound channel and light red coloring of the muscles are observed. If the stop is loose and at a very close distance, skin burns from the pronounced thermal effect of black powder are observed.
When fired within one meter, one entrance gunshot wound with a diameter of 2–4 cm with uneven scalloped, sooty edges is formed. At a distance of one to 2–5 m, a main gunshot entrance hole of similar size and character is formed, around which there are separate round wounds with a small skin defect, roughened and metallized edges. As the shooting distance approaches 2–5 m, the number of such wounds increases. At distances exceeding 2–5 m, only isolated small round wounds are formed from the action of single pellets. Shot wounds, as a rule, are blind.
When fired with a shotgun cartridge, damage can be caused by wads, some of which (for example, felt ones) fly up to 40 m. Wads have a mechanical, and in some cases, a local thermal effect.
Automatic burst wounds
Due to the high rate of fire, the relative position of the weapon and the victim during the automatic burst practically does not change. When shot at close range, this can lead to the formation of connected (double or triple) wounds. Gunshot injuries caused by automatic burst bullets are characterized by a complex of the following distinctive features: multiplicity, one-sided and sometimes close to each other location of gunshot entrance wounds, their similar shape and size, parallel or slightly divergent direction of wound channels, as well as the properties of entrance wounds, allowing them to occur when fired from the same distance. When fired in a short burst at a distance close to the stop, the wounds are located next to one another; when fired in a long burst from a weapon that is not firmly fixed, they are scattered. Characterized by heavy bleeding
Blast injury
FOR ETHICAL REASONS, THERE ARE NO PHOTOS, I THINK EVERYONE CLEAR THE CONSEQUENCES.
An explosion is a pulsed release of a large amount of energy as a result of physical or chemical transformations of a substance.
In forensic medical practice, injuries from explosions of explosives are most often encountered. An explosion produces a detonation wave, which is a chemical process of converting a solid explosive into gaseous products.
Instantly expanding, gases create powerful pressure on the environment and lead to significant destruction. At a short distance from the center of the explosion, they have thermal and chemical effects. They are conventionally called explosive gases. Continuing to expand, they form a shock wave, at the front of which a pressure of up to 200–300 thousand atm is created. As you move away from the center of the explosion, the surface of the shock wave front gradually increases, and its speed and pressure decrease.
As a result of detonation, individual particles can be torn off from the mass of the explosive, which scatter with the shell and other elements of the explosive device at a separation speed of about 1000 m/s.
Explosive gases and a shock wave can destroy various barriers, forming fragments of secondary projectiles.
The damaging factors of an explosion include:
1) explosive gases, explosive particles, explosion soot;
2) shock wave;
3) fragments and particles of an explosive device - fragments and parts of the fuse, fragments of the shell of an explosive device;
4) special destructive agents: elements of mechanical action (balls, rods, arrows, etc.), substances of chemical action, substances of thermal action (phosphorus, napalm, etc.);
5) secondary projectiles - fragments of destroyed barriers, surrounding objects, parts of clothing and shoes, destroyed and torn off parts of the body.
Injuries resulting from these factors are called blast injuries.
Explosive gases act mechanically, thermally and chemically. The nature of the mechanical action depends on the size of the charge and the distance from the center of the explosion. Explosive gases destroy leather at a distance of 2 times the radius of the explosive charge, and textile fabrics at a distance of 10 radii of the explosive charge. The destructive effect is expressed in extensive defects and crushing of soft tissues.
Leather ruptures from the action of explosive gases are observed at a distance of 10, and textile fabrics - 20 radii of the explosive. The tearing action results in skin tears and soft tissue separation.
The bruising effect of explosive gases on the skin is observed at a distance of up to 20 charge radii. It manifests itself in the form of precipitation and intradermal hemorrhages, sometimes repeating the shape of the folds of the victim’s clothing.
The thermal effect of gases is expressed in the form of hair loss and rarely - superficial burns of the skin, and the chemical effect - in the formation of oxy-, sulfo-, met- and carboxyhemoglobin in destroyed soft tissues.
Explosive particles can have local mechanical (small abrasions, bruises, superficial wounds), thermal and chemical effects (burns). Carbon soot from an explosion usually impregnates the surface layers of the epidermis.
The consequences of a shock wave are similar to damage from blows with a blunt hard object with a wide flat traumatic surface. A pressure drop in the shock wave front of 0.2–0.3 kg/cm2 can lead to rupture of eardrums; 0.7–1.0 kg/cm2 can cause fatal damage to internal organs.
The lungs on the side facing the center of the explosion are most often affected. In the lung parenchyma, hemorrhages are observed mainly in the apical region, the hepatic surface and in the hilar zone. Under the pleura of the lungs, multiple point hemorrhages are visible, located in the intercostal spaces.
Passing from the air into the liquid media of the body, a shock wave, due to the high density and incompressibility of these media, can increase the speed of its propagation and lead to significant destruction. This phenomenon is called an inward explosion.
Fragments and parts of an explosive device have different energies depending on their mass and density, the power of the explosion and the distance from its center. Therefore, shrapnel damage is highly variable.
Depending on what factors had a damaging effect, three distances are distinguished:
1) very close (contact explosion or contact) - detonation products, shock wave and fragments act;
2) relatively close – damage is caused by the combined action of a shock wave and fragments;
3) not close - only fragments are effective.
Damage from secondary projectiles can occur at any of the three ranges.
THIS IS WHAT I FINISH, AND I SINCERELY WISH THAT THIS ARTICLE WILL NEVER BE USEFUL TO ANYONE) TO THE WHOLE WORLD. SHOOT THE BOTTLES!!!
5.30
October 15, 2013
Preparations for the treatment of penetrating wounds
To treat penetrating wounds, the victim must be placed in a specialized hospital. After an accurate diagnosis, tetanus toxoid 0.5 IU is prescribed subcutaneously and anti-tetanus serum 1000 IU. Drug therapy should include the following groups of drugs:
Antibiotics
- Aminoglycosides: gentamicin three times a day, 5 mg/kg IM, for up to 10 days; it is possible to prescribe tobramycin daily at 2-3 mg/kg IM or IV;
- Penicillins: ampicillin 250-500 mg IM or IV up to 6 times daily;
- Cephalosporins: cefotaxime 1-2g IM or IV up to 4 times daily; ceftazidime 0.5-2g;
- Glycopeptides: vancomycin 0.5-1g IV up to 4 times daily or orally 0.5-2g;
- Macrolides: azithromycin 500 mg orally, course 3 days;
- Lincosamides: lincomycin 600 mg IM up to 2 times a day.
Sulfonamide drugs
- Sulfadimethoxine: 1 g on the first day, then 500 mg daily for up to 10 days or sulfalene 1 g on the first day, then 200 mg daily for 10 days.
Fluoroquinolones
- Ciprofloxacin 250-750 mg orally twice a day for up to 10 days.
Antifungal agents
- NSAIDs: diclofenac 50 mg orally up to 3 times daily for 10 days or indomethacin 25 mg orally up to 3 times daily;
- Glucocorticoids: dexamethasone 2-3 mg under the conjunctiva for up to 10 days; triamcinolone 20 mg every week once 3-4 times.
H-receptor blockers
- Chloropyramine 25 mg orally three times a day for up to 10 days or loratadine 10 mg orally once for up to 10 days;
Tranquilizers
- Diazepam 10-20 mg IM or IV.
Injections of enzyme preparations
- Fibrinolysin parabulbar 400 units;
- Collagenase subconjunctivally 100 or 500KE into the lesion or through electro- or phonophoresis for up to 10 days.
Eye drops
If the condition is particularly severe and in the postoperative period, the frequency of instillations can be up to 6 times daily. It is reduced as the inflammation process subsides:
- Antibacterial solutions: Ciprofloxacin 0.3%, 1-2 drops;
- up to 6 times daily or Oftaxacin 0.3%, 1-2 drops up to 6 times daily or Tobramycin 0.3%, 1-2 drops up to 6 times daily;
- Antiseptic solutions: Piclosidine (Vitabact) 0.05%, 1 drop up to 6 times daily;
- Glucocorticoid solutions: Dexamethasone 0.1%, 1-2 drops up to 6 times daily or Hydrocortisone 1-2.5% ointment, put up to 4 times daily behind the lower eyelid;
- NSAID solutions: Diclofenac 0.1%, 1-2 drops up to 4 times daily or Indomethacin 0.1%, 1-2 drops up to 4 times daily;
- Solutions of combined drugs: Maxitrol, Tobradex;
- Mydriatic solutions: Cyclopentolate 1%, 1-2 drops three times a day or Tropicamide 0.5-1%, 1-2 drops up to 4 times daily in combination with Phenylephrine 2.5%, 1-2 drops three times a day;
- Stimulators of corneal tissue regeneration: Actovegin 20% ophthalmic gel, 1 drop for the lower eyelid three times a day or Dexapanthenol 5% ophthalmic gel, 1 drop for the lower eyelid three times a day.
The patient after severe damage to the organ of vision should be monitored by an ophthalmologist for life. His physical activity should be limited. In the long term, such patients are prescribed further surgical treatment aimed at restoring or maintaining visual functions and eliminating cosmetic defects.
Gunshot wounds of large joints
1.1 General characteristics and classification of gunshot wounds of large joints of the extremities
Gunshot wounds of large joints of the limbs during the Second World War (1941-1945), the war in Afghanistan (1979-1989), the war in the Chechen Republic (1994-1999), wars in the Far East of the 90s of the XX century and a number of local conflicts of recent decades occurred in 5.3 - 7.4% of all limb injuries.
Injuries to the knee joint were more common (24.5 – 33.9%). The severity of joint injuries is determined by the use of modern, high-energy weapons and significant destruction of soft tissue, blood vessels and nerves. More than 50% of the wounded are diagnosed with penetrating joint injuries, which significantly aggravates the course of the wounds[2,4,5]. In addition, in recent decades, both in the world in general and in the Middle East in particular, there has been an increase in the number of gunshot injuries among civilians. Despite the use of modern treatment methods, treatment outcomes for gunshot wounds of large joints of the extremities are often unsatisfactory. Thus, purulent-inflammatory complications, contractures and ankylosis of joints, “loose joints,” according to various authors, complicate the course of such wounds in 40–76%. The most severe injuries are to the knee and hip joints. During the Second World War, in the local wars of recent decades, every fifth wounded person with intra-articular fractures of the knee joint underwent hip amputation for health reasons, due to the development of severe forms of infectious complications [1,4]. To classify gunshot wounds to joints, it is generally accepted to use the Gustilo classification (Table 1)[7]
| GustiloGrade | Definition |
| I | Open fracture, clean wound, wound <1 cm in length |
| II | Open fracture, wound > 1 cm in length without extensive soft-tissue damage, flaps, avulsions |
| III | Open fracture with extensive soft-tissue laceration, damage, or loss or an open segmental fracture. This type also includes open fractures caused by farm injuries, fractures requiring vascular repair, or fractures that have been open for 8 hr prior to treatment |
| III A | Type III fracture with adequate periosteal coverage of the fracture bone despite the extensive soft-tissue laceration or damage |
| III B | Type III fracture with extensive soft-tissue loss and periosteal stripping and bone damage. Usually associated with massive contamination. Will often need further soft-tissue coverage procedure (ie free or rotational flap) |
| III C | Type III fracture associated with an arterial injury requiring repair, irrespective of degree of soft-tissue injury. |
Table 1
However, the classification of Shapovalov V.M. is more relevant from a practical point of view. and Tikhilova R.M. (2000) (Table 2) [5, 8]
| In relation to the joint cavity | through, blind and tangent |
| By type of wounding projectile: | bullet, fragmentation, mine-explosive, secondary projectiles. |
| According to the nature of the injury: | penetrating, non-penetrating, through, blind, tangent. |
| According to the degree of damage to soft tissue and bone: | pinpoint wound of soft tissue without bone damage; a soft tissue wound that does not require surgical treatment, with minor bone damage; extensive soft tissue defect with significant bone damage. |
| According to the nature of intra-articular injuries | - fractures with minor or moderate bone damage: types B, C1, C2 according to the classification of M. Muller et al (type I according to RBGustillo); – fractures with severe bone damage: complete comminuted intra-articular fractures with defects and damage to bone and cartilage tissue, with a high risk of bone necrosis and the development of contractures – types B3 and C fractures of the femoral head, as well as type C3 fractures of other large joints of the extremities (type II according to RB Gustillo). |
| For associated damage: | with damage to large blood vessels; with nerve damage. |
Table 2
1.2 Clinic and diagnosis of gunshot wounds of joints
Clinical manifestations of gunshot wounds to joints depend on the type of joint and the nature of the damage. Other things being equal, the most severe general symptoms are observed with injuries to the hip, knee and shoulder joints. When injured by high-velocity ammunition, both bullets and shrapnel, their fragmentation is typical after contact with the bone formations of the joint. In the future, these fragments play the role of foreign bodies, which significantly complicates and aggravates the postoperative course. Relatively mild joint injuries occur when a predominantly low-velocity bullet or fragment penetrates the joint cavity and gets stuck in the bone structure.
The clinical picture consists of general and local symptoms. Local manifestations are characterized by limited mobility, severe pain with the slightest movement, an increase in the size of the joints, resulting in increasing swelling and hemarthrosis. With extensive soft tissue defects in the joint area, leakage of synovial fluid is often noted.
The general condition of a victim with a gunshot injury to a joint can be very severe and accompanied by shock. It should be borne in mind that shock with injuries to the hip or knee joint occurs 2-2.5 times more often than with injuries to the joints of the shoulder or forearm. If, simultaneously with damage to the bone structures of the joint, the nerves or main blood vessels are damaged, the danger of rapidly increasing complications in the form of anaerobic infection, putrefactive infection, ischemic gangrene of the limb is very high.
Damage to large blood vessels during gunshot injuries to the joints of the upper extremities is observed in 3% of cases, of the lower extremities - 4.5%. The first place in these options is occupied by the knee, elbow and ankle joints. Peripheral nerves, on the contrary, are more often (about 12%) affected by injuries to the joints of the upper limb; for injuries of the hip, knee and ankle joints, the frequency of nerve injuries is about 6% [2,6].
It should be noted that the clinical picture of even a penetrating joint injury can be blurred, especially in patients with combined, combined or multiple injuries. Clinical manifestations of joint injury are observed in these cases in the form of purulent inflammation.
The inflammatory reaction of both periarticular tissues and the synovial membrane can develop either in the form of serous-fibrous inflammation, and if the diagnosis is not made in time and adequate treatment is not started, the development of a clinical picture of purulent inflammation and joint empyema is possible. After gunshot wounds of large joints, especially in the presence of foreign bodies, comminuted fractures (C2, C3 types), periarticular phlegmon, putrefactive or anaerobic panarthritis, and osteomyelitis of the epiphyses can develop.
The clinic of purulent complications of gunshot wounds of the joints is especially pronounced with empyema of the joint; intermuscular swelling and para-articular phlegmon, osteomyelitis of the epiphyses of the bones that make up the joint often develop. It becomes more pronounced, and the condition of the wounded becomes severe with capsular phlegmon and especially with osteomyelitis of the epiphysis (or epiphyses). With the development of such complications, the development of sepsis is very likely, which may require amputation of the limb.
From the point of view of diagnosis and monitoring of the wounded over time, it is necessary to resort to systematic punctures of the joint and examination of the wound discharge (cytological and bacteriological). In addition to a local examination of the wounded person, studying the direction of the entrance and exit holes, mobility, pain during active and passive movements, an X-ray examination is necessary in at least two projections. The X-ray picture of gunshot joint fractures is fundamentally different from that of peacetime fractures. The latter are mainly typical fractures, in classic places of the skeleton, with characteristic displacement of fragments; these are more or less stencil, all repeating within a narrow framework the same x-ray patterns. With gunshot joint fractures, the x-ray picture never repeats. For gunshot fractures, there are no typical places in the same bone and no favorite locations in any part of the skeleton - any point in the skeletal system can be damaged by a gunshot projectile. Even the displacement of fragments here is always different, because they are determined not so much by muscle traction and the localization of the fracture itself, but by the circumstances of the wound itself, such as, for example, the direction of flight of a bullet or fragment, the size of the latter, its manpower and the circumstances of the wound, the fall of the wounded, etc. . Generally speaking, the displacement of fragments in gunshot fractures is usually more pronounced than in a normal injury - individual large fragments rotate at a very large angle to the axis of the bone, and the fragment can even rotate in a circle, 180°, for example, with the convex side in the concave side.
The most valuable thing that radiographs provide is the determination of the presence or absence of a violation of the integrity of the bone elements of the joint - a fracture of the epiphyses, articular head, articular cavity. The main task of x-ray examination in the acute period of joint injury is to establish the presence or absence of a fracture or crack in the bone involved in the formation of the joint, as well as to determine the volume of the lesion, the extent of the injury, zone-osseous damage, i.e. the exact quantitative and qualitative characteristics of the joint injury (Fig. 1). Everything related to the so-called soft tissues is incomparably better and more fully assessed clinically than radiographically.
rice. 1
As for x-ray examination of injuries to each joint separately, now x-ray pictures have been studied in extremely detail. Classifications (groupings) of injuries to individual joints take into account the main clinical and anatomical-functional-radiological features of each of them, mainly the presence or absence of a fracture of one or another important articular element. So, for example, for the hip joint this is the acetabulum, femoral head, medial part of the femoral neck, greater trochanter, isolated or combined fractures of which determine the severity of the injury, choice of treatment method, outcome, etc. For the knee joint, the presence of a fracture of the internal and the external condyles of the femur and the proximal tibia, patella, etc. [6].
Computed tomography (CT), magnetic resonance imaging (MRI) and arthroscopic diagnostics play a major role in the diagnosis of gunshot wounds of joints at later stages of treatment.
1.3 General principles of treatment of gunshot wounds of joints
At the stage of first medical, first medical and qualified care for gunshot wounds of the joints, it involves temporarily stopping bleeding, applying an aseptic dressing to the wound, transport immobilization of the limb, administering painkillers and transporting the wounded. In case of significant blood loss, transfusions of crystalloid solutions, polyglucin, rheopolyglucin, plasma, and preserved blood are carried out. In all cases, antibiotics are administered intramuscularly.
At the stage of specialized orthopedic care, the most important role is played by adequate surgical treatment of the wound, reliable fixation of bone fragments, prevention of infectious complications and compensation of homeostasis disorders. Thus, with pinpoint wounds of joints and minor damage to soft tissues, especially with a through bullet wound, even with the presence of a fracture, it is often sufficient and justified to perform a puncture of the joint, evacuate the blood and administer antibiotics. Arthrotomy itself is dangerous due to the generalization of the process. If there is a large intra-articular body, extensive soft tissue damage, significant hematoma and swelling of a limb segment, especially if the wound is dirty or there are signs of suppuration, primary surgical treatment of the wound is indicated in compliance with the principles of reconstructive surgery - with osteosynthesis, suture of the great vessels and nerves and radical intervention in the indicated cases, up to resection of the joint or even amputation if it is destroyed.
In relation to the shoulder, elbow, wrist, and ankle joints, surgical tactics should, with rare exceptions, be as cost-saving as possible, including in case of crushed intra-articular fractures. Bone resections are performed according to strict indications, for example, with a progressive purulent process.
The correct choice of limb immobilization or osteosynthesis is of utmost importance. For minor injuries, it is possible to use a plaster cast or modern plastic orthoses. However, everyone knows its shortcomings. The most advanced way to immobilize a limb during intra-articular fractures is transosseous osteosynthesis with external fixation devices. There are few contraindications to transosseous osteosynthesis with devices: a state of shock, an acute purulent process in the joint, a generalized form of infection, suspected anaerobic infection.
When performing surgical treatment of gunshot wounds of types I and II according to RB Gustillo and the first type of intra-articular metaepiphyseal fractures, it is advisable to perform gentle surgical treatment of wounds, revision of the joint from minimal access, removal of tissue detritus and foreign bodies from it, precise reposition of bone fragments and restoration of joint congruence. Then, if necessary, stable fixation of bone fragments should be performed using interfragmentary compression with AO cancellous screws, and then “bridging” fixation of the fracture with anatomically modeled LCP plates using locking screws should be performed. At the final stage of the operation, the joint must be drained, followed by restoration of the integrity of its capsule and primary closure of skin wounds.
For gunshot wounds of joints of types IIIA and IIIB according to RB Gustillo, treatment tactics should include: gentle surgical treatment of wounds with careful treatment of soft tissues and preservation of all bone fragments, removal of foreign bodies, abundant washing of wounds and the joint cavity with antiseptics, restoration of joint congruence and low-traumatic osteosynthesis . The operation should be completed by flow-aspiration drainage of the damaged joint, restoration of the integrity of its capsule and primary closure of the wound with local tissues without tension.
The choice of fixation method in this group of patients is decided individually. In case of comminuted fractures and difficulties in restoring joint congruence using external fixation devices, osteosynthesis was performed with plates and screws, especially in cases of damage to the elbow and hip joints. When patients presented late and there was a high risk of developing infectious complications, preference was given to fixing intra-articular fractures with a pin-rod device, which in some cases was later replaced by immersion osteosynthesis. The main factors for determining the timing of replacement of the external fixation device with a plate with angular stability of the screws were the positive dynamics of healing of soft tissue wounds and the absence of signs of infection. Such operations were performed 20–24 days after the first intervention. If there was a bone defect in the area of the gunshot fracture, this stage of the operation was supplemented with free bone autoplasty and an iliac crest graft. Contraindications to sequential internal osteosynthesis were complicated wound healing, osteoarthritis, necrosis and soft tissue defects in the joint area. For the same reasons, pin-rod devices can be used to fix fragments until the fracture heals.
In case of comminuted intra-articular fractures with defects and damage to bone and cartilaginous tissues, corresponding to the second type of fractures according to the “orthopedic classification”, it is advisable to perform primary surgical treatment of wounds with maximum preservation of para-articular tissues and bone fragments without achieving ideal reposition. It should be especially noted that of this group of wounded, the majority require joint replacement surgery over the subsequent period. It is advisable to stabilize bone fragments in such wounded people using pin-and-rod devices in the mode of moderate distraction, passing transosseous elements paraarticularly, taking into account the topographic and anatomical features of the damaged joints. Such operations should be completed by restoring the integrity of the joint capsule and the soft tissue cover above it, as well as by flow-aspiration drainage.
Wounded with severe intra-articular type C3 fractures and concomitant injuries to the main arteries: femoral, popliteal, brachial, etc. These patients underwent osteosynthesis and restoration of the integrity of damaged arterial vessels through venous autoplasty.
It should also be noted that when performing immersion osteosynthesis with plates with angular stability of screws, the following principles must always be observed: accurate reposition of bone fragments in intra-articular comminuted fractures; stable fixation of bone fragments using interfragmentary compression with standard AO screws and “bridging” fracture fixation using locking screws; low-traumatic surgical approaches should be used; implants (plates) were placed epiperiosteally under the muscles, limiting their contact with the bone; screws were inserted in the metadiaphsar zone through skin punctures; At least three locking screws are inserted into the proximal and distal bone fragments.
To close soft tissue wounds, the following are used: primary suture without significant tension on the edges of the wound; primary delayed sutures or free skin autoplasty, skin grafting with complex flaps on a permanent feeding pedicle.
In wounded patients in whom, after clinical and radiological examination, delayed consolidation of bone fragments was diagnosed or positive dynamics of fracture healing were not observed, autologous bone grafting is performed to stimulate osteogenesis and prevent fatigue fracture of the implant.
1.4 Clinical examples of treatment of gunshot wounds of joints
1.4.1 Gunshot wounds of the hip joint
Clinical example 1. Patient G. IB No. 4442, 43 years old, was admitted to the trauma department of the Military Hospital of the Ministry of Defense of the Russian Federation on October 29, 2001. Diagnosis: Post-traumatic defect of the proximal end of the right femur with a complete absence of the hip joint and shortening of the right lower limb by 12 cm. From the anamnesis it was established that in March 1995 in Grozny, during combat operations, she received a shrapnel wound to the right hip joint. In the city hospital of Grozny, osteosynthesis of the fracture was performed with cerclage wire (Fig. 2), but in the postoperative period it was complicated by suppuration of the wound, resulting in gunshot osteomyelitis.
rice. 2
The patient was treated for osteomyelitis for 5 years. During this time she underwent 18 operations. The outcome of the treatment was the absence of the proximal end of the hip bone for 12 cm with a complete absence of the hip joint (Fig. 3).
rice. 3
Figure 4 shows the patient before surgery (the height of the bolster on which the sick leg stands is 12 cm).
rice. 4
The examination revealed that the patient had no evidence of a chronic purulent process. The patient is somatically safe. On November 1, 2001, an operation was performed - total endoprosthesis replacement of the right hip joint with an oncological endoprosthesis with cement fixation of the femoral and acetabular components. Due to a defect in the roof of the acetabulum, it was strengthened using autologous bone grafting from the iliac crest. During the operation, with the help of an oncological leg and lengthening rings, it was possible to eliminate the shortening and lengthen the leg by 12 cm (Fig. 5).
rice. 5
Figure 6 shows the patient after 14 days. after surgery – the length of the limbs is equalized. The postoperative period proceeded smoothly. The sutures were removed on the 14th day. Healing by first intention.
rice. 6
In Fig. 7, X-ray of the hip joint of patient G 10 years after surgery (2011). There are no signs of instability of the endoprosthesis components. The patient walks without additional support. I am satisfied with the results of the operation.
rice. 7
Clinical example 2. Patient F. IB No. 6914, 73 years old, admitted to the 2nd orthopedic department of the Scientific Research Institute of Traumatology and Traumatology on May 16, 2005. Diagnosis: Consequences of a gunshot wound to the right hip joint. The defect is pseudarthrosis of the proximal part of the right femur (Fig. 8).
rice. 8
Shortening of the right lower limb by 10 cm. Criminal injury, received in 2000. In subsequent years, 7 different types of osteosynthesis were performed (Fig. 9, 10, 11), which did not produce an effect and led to the development of a defect - pseudarthrosis of the proximal part of the right femur .
rice. 9
rice. 10
rice. eleven
During the time since the injury, there was no evidence of a purulent process in the fracture area. On May 19, 2005, an operation was performed - total endoprosthesis replacement of the right hip joint with an oncological endoprosthesis with hybrid fixation of the femoral and acetabular components (Fig. 12).
rice. 12
The removed bone fragments and fragments of the femur and hip joint are shown in Fig. 13. The postoperative period proceeded smoothly. The sutures were removed on the 14th day. Healing by first intention. The patient was observed for 7 years. There were no signs of instability of the endoprosthesis components.
rice. 13
1.4.2 Gunshot wounds of the knee joint
Clinical example 3. Patient A., 47 years old, was admitted to the orthopedic department of the Saratov Regional Clinical Hospital on August 6, 2007. Diagnosis: Consequences of a gunshot wound to the right femur in the lower third. Defect-pseudoarthrosis of the femur in the lower third (up to 13 cm). Necrosis of the femoral condyles. Right-sided gonarthrosis III stage. Severe combined contracture of the right knee joint (Fig. 14).
rice. 14
From the anamnesis it was established that in 2000 he received a severe gunshot wound to the right knee joint and the right femur in the lower third. For this reason, he underwent 8 osteosynthesis operations of various types, which did not bring any effect. August 07, 2007 surgery - arthrotomy, wound revision, removal of foreign bodies, condyles of the femoral right femur and patella. Replacement of the defect of the right knee joint and the lower third of the right femur with an oncological related knee joint endoprosthesis, manufactured by CITO-MATI (Russia) (Fig. 15).
rice. 15
Intra- and postoperative blood loss – up to 1000 ml. Shortening of the right lower limb by 13 cm was completely eliminated (Fig. 16). Observation of the patient for more than 5 years. The patient leads an active lifestyle. Works as a farmer. I am satisfied with the results of the operation.
rice. 16
1.4.3 Gunshot wounds of the shoulder joint
Clinical example 4. Patient G., 48 years old, was admitted to the orthopedic department of the Saratov Regional Clinical Hospital on 02/09/2009. Diagnosis: Consequences of a gunshot wound to the right shoulder joint and the upper third of the right humerus. Defect-pseudoarthrosis of the right humerus in the upper third (4 cm). Aseptic necrosis of the head of the right humerus. (Fig. 17).
rice. 17
From the anamnesis it was established that in December 2007 he received a severe gunshot wound to the right shoulder joint and the right humerus in the upper third. For this reason, he underwent several transosseous osteosynthesis operations, which had no effect. 11.02. 2009 surgery - arthrotomy, wound revision, removal of the head of the humerus and bone fragments, endoprosthetics of the right shoulder joint with an ESI endoprosthesis (Russia), tenolysis, restoration of the capsule of the right shoulder joint (Fig. 18).
rice. 18
In Fig. 19, patient G. for 10 days. after operation. The function of the limb is quite satisfactory. Observation of the patient for more than 4 years. The patient leads an active lifestyle. Works as a driver. I am satisfied with the results of the operation.
rice. 19
Clinical example 5. Patient K., 33 years old, was admitted to the orthopedic department of the Saratov Regional Clinical Hospital on January 16, 2012. Diagnosis: Consequences of a gunshot wound to the right shoulder joint. Aseptic necrosis of the head of the right humerus. Severe combined contracture of the right shoulder joint (Fig. 20).
rice. 20
From the anamnesis it was established that in March 2011 he received a gunshot wound to the right shoulder joint in combination with a severe chest injury and a severe closed craniocerebral injury. He underwent a number of operations on the head and chest. Treatment for a fracture of the shoulder joint is limited to primary surgical treatment of the wound. 01/18/2012 surgery - arthrotomy, wound revision, removal of the head of the humerus and bone fragments, endoprosthetics of the right shoulder joint with an ESI endoprosthesis with a bipolar head (Russia), tenolysis, restoration of the capsule of the right shoulder joint. (Fig. 21).
rice. 21
Immobilization of the limb with an abduction splint (30°) for 40 days. In Fig. 22, patient K. at 30 days. after operation. Observation of the patient for more than 1 year. The patient is engaged in intellectual work. I am satisfied with the results of the operation.
rice. 22
1.4.4 Gunshot wounds of the elbow joint
Clinical example 6. Patient K., 27 years old, was admitted to the orthopedic department of the Saratov Regional Clinical Hospital on May 15, 2006. Diagnosis: pseudarthrosis of the distal third of the left humerus after a gunshot wound, post-traumatic arthrosis of the left elbow joint of the third degree, combined contracture of the left elbow joint , foreign bodies (metal fragments) of the soft tissues of the left shoulder (Fig. 23).
rice. 23
The injury was received four years ago (a gunshot wound to the left shoulder). Surgical interventions were performed repeatedly, and long-term immobilization with plaster casts was carried out. Movements in the left elbow joint are “rocking” - within 10 - 15° (Fig. 24).
rice. 24
There is no neurological deficit. 05/18/2006 operation - total endoprosthetics of the left elbow joint with an ESI endoprosthesis (Russia) (Fig. 25).
rice. 25
The postoperative period proceeded smoothly. The range of motion in the elbow joint two months after endoprosthetics is quite satisfactory, muscle strength in the operated arm is sufficient, and no muscle atrophy is noted (Fig. 26). The follow-up time after surgery is 7 years. I am satisfied with the results of the operation.
rice. 26
Clinical example 7. Patient A., 27 years old, was admitted to the orthopedic department of the Saratov Regional Clinical Hospital on February 12, 2007. Diagnosis: Condition after a severe gunshot wound to the left elbow joint, defect-pseudoarthrosis of the left humerus (up to 7 cm) after a gunshot wound. (Fig. 27).
rice. 27
The injury was received 3 four years ago (gunshot wound to the left elbow joint), while hunting. Many osteosynthesis operations and long-term plaster immobilizations were performed. The movements in the left elbow joint are “rocking” - like a “dangling joint”. There is no neurological deficit. 02/14/2007 operation - total endoprosthetics of the left elbow joint with an ESI endoprosthesis (Russia) (Fig. 28).
rice. 28
The postoperative period proceeded smoothly. The range of motion in the elbow joint three months after endoprosthetics is quite satisfactory, muscle strength in the operated arm is sufficient, and no muscle atrophy is noted (Fig. 29). The follow-up time after surgery is 5 years. The patient leads an active lifestyle. Drives a car independently and does physical labor. I am satisfied with the results of the operation.
rice. 29
Thus, the treatment of gunshot wounds of large joints of the extremities, both in war and in peacetime, remains an urgent problem in traumatology and orthopedics. Modern firearm wounding projectiles are characterized by high damaging power. Therefore, the nature of the injuries is almost always severe and each time non-standard. In this regard, the nature of damage, even to the same joint, by the same wounding projectile, is always individual. This determines the choice of treatment tactics. Primary surgical treatment of a gunshot wound of the joint is the key point in the treatment and prevention of subsequent complications. It should be performed in the shortest possible period of time and contain the full scope of reconstructive measures, including vascular suture, restoration of nerves and tendons. It is generally accepted that at an early stage the method of choice is transosseous osteosynthesis. However, as the wound heals, inflammation stops and the general condition of the wounded person stabilizes, it is advisable to perform submersible reosteosynthesis using modern structures, both extraosseous and intramedullary, blocking. Numerous studies have proven that the outcomes of treatment of severe gunshot fractures of the extremities, even performed by experienced orthopedists, with the appropriate equipment, are unsatisfactory in 40–60% of cases. This is expressed in the development of false joints, defective pseudoarthrosis, stage 3-4 arthrosis, severe contractures and ankylosis. In this regard, there is often a need for endoprosthesis replacement of the affected joint. The use of modern implants for large joints, cementless and cemented fixation, allows for a long-term restoration of the joint anatomically, restoring its function for a sufficiently long period.
Literature:
- Akhmedov B.A., Tikhilov R.M. Surgical treatment of intra-articular gunshot injuries of large joints of the extremities // Traumatology and Orthopedics of Russia, 2008, No. 2, P.5-13
- Kapustin R.F., Gombalevsky D.V. Gunshot wounds of the extremities // Methodological recommendations, Minsk, 2004
- Solomin, L.N. Basics of transosseous osteosynthesis using the G.A. apparatus Ilizarova / L.N. Solomin. – St. Petersburg: MORSAR AV, 2005. – 544 p.
- Shapovalov, V.M. Combat injuries to the limbs: infrastructure of wounds and characteristics of the condition of the wounded during local wars / V.M. Shapovalov // Traumatology and Orthopedics of Russia. – 2006. – No. 2. – P. 301–302.
- Shapovalov V.M. Averkiev V. A. Modern principles of treatment of gunshot wounds of limb joints at the stages of medical evacuation // “State and prospects for the development of military traumatology and orthopedics” - proceedings of the Military Medical Academy, volume 248, St. Petersburg, 1999, pp. 210-218
- https://auno.kz/rentgenodiagnostika-zabolevanij-kostej/369-rentgenodiagno…
- Gustilo, RB Problems in the management of type III (severe) open fractures: a new classification of type III open fractures / RB Gustilo, RM Mendoza, DN Williams // J. Trauma. – 1984. – Vol. 24. – P. 742.
- Muller, M. The AO classification of fractures / M. Muller, S. Nasarin, P. Koch. – Berlin etc. :Springer_Verlag, 1987.