Symptoms of hypothalamic syndrome
Metabolic disease:
- Change in body weight (increase or decrease);
- The appearance of stretch marks (stretch marks) on the skin in the thighs, armpits, back, buttocks;
- Pungent odor of sweat;
- Increased concentrations of certain substances in blood tests (glucose, thyroid hormones, insulin, ALT, AST, GGT, prolactin).
Striae on the skin
Vascular symptoms:
- Increased or unstable blood pressure;
- Vascular spasms;
- Palpitations and discomfort in the heart during physical activity and stress;
- Decreased physical endurance.
Psychovegetative symptoms:
- Persistent decrease or mood swings, depression;
- Insomnia or drowsiness;
- Fatigue;
- Headache;
- Increased appetite and thirst;
- Decreased or increased sexual desire.
Medical Internet conferences
Menstrual dysfunction in the structure of hypothalamic syndrome of puberty in girls
Rysmukhambetova K.A.
Scientific supervisor: candidate of medical sciences, assistant Trushina O.V.
Federal State Budgetary Educational Institution of Higher Education Saratov State Medical University named after. IN AND. Razumovsky Ministry of Health of Russia
Department of Obstetrics and Gynecology, Faculty of Pediatrics
Relevance . Hypothalamic syndrome of puberty (HSPP), which is based on reversible functional disorders of the hypothalamus as a central structure that regulates all parts of homeostasis, is characterized by a polymorphism of clinical manifestations in the form of metabolic disorders, neurovegetative and psychoemotional disorders, and dysfunction of the endocrine glands. The prevalence of GSPP in the teenage population among girls reaches 131.1 per 1000. An unfavorable prognosis with the progression of GSPP is due to the risk of transition to the manifestation of metabolic syndrome and the formation of multidirectional disorders of reproductive function.
Purpose of the study . To study the features of menstrual function in adolescent girls with hypothalamic dysfunction.
Materials and methods . A retrospective analysis of the medical records of 300 patients aged 14-17 years (average age 15.1±1.4 years) with HSPP, who underwent a primary examination at the Saratov Regional Children's Clinical Hospital, was carried out. Group I (n=100) included girls with hypomenstrual syndrome, group II (n=100) included patients with abnormal uterine bleeding, group III (n=100) included girls with a regular menstrual cycle.
Research results . The onset of puberty between the ages of 10 and 13 years was observed in the majority of patients (72.0%; 57.0%; 83.0%), in other cases - before the age of 10 years (28.0%; 43.0%; 17.0%). Girls with an inverted version of puberty were more common in group I (21.0%; 18.0%; 12.0%). The age of menarche for the majority occurred between 12 and 15 years (78.0%, 86.0%, 89.0%). Menarche before the age of 12 years was more common than at the age of over 15 years (21.0% and 1.0%; 11.0% and 3.0%; 9.0% and 2.0%). Obesity of the 3rd degree was more common in group I than in groups II and III (69.0%; 14.0%; 4.0%). All patients had autonomic dysfunction. Girls with initial hypersympathicotonia were less common in group I than in groups II and III (37.0%; 82.0%; 11.0%). In response to the influence of a physiological stressor, hypersympathicotonic patterns were most often noted (82.0%; 73.0%; 56.0%). Thus, multidirectional dysfunctions of the reproductive system among patients with HSPP are interrelated with the degree of lipid metabolism impairment and the nature of autonomic dysfunction. An interdisciplinary personalized approach to treatment and rehabilitation measures for young patients with HSPP will preserve their reproductive potential.
Examination for hypothalamic syndrome and diagnosis
The treatment will hit the target if the causes of the disease are established. Therefore, we pay great attention to diagnostics.
MRI of the brain and pituitary gland. We often find hydrocephalus with increased intracranial pressure, traces of trauma or oxygen deprivation of the brain. Pituitary microadenomas are less common.
Hormonal and biochemical blood tests. Tests will help determine exactly how the metabolism is disrupted. And then we will learn how to deal with the problem faster and easier.
Ultrasound of the liver. Enlargement and fatty infiltration of the liver (fatty hepatosis) are characteristic of disorders of carbohydrate and fat metabolism.
Ultrasound of the thyroid gland. Our most common finding is thyroid nodules. Hormonal blood tests help us interpret their significance.
Examination of the adrenal glands using ultrasound or MRI may be necessary if the content of adrenal hormones in a blood test deviates from the norm.
A heart study (echo-CG, ECG, daily monitoring of ECG and blood pressure) will provide information about the causes of increased blood pressure and suggest ways to correct it.
In recent years, articles on the problem of hypothalamic syndrome have been unfairly rarely published in the medical literature. At first glance, it may seem that this pathology does not require serious attention from a doctor, and its treatment in most cases is limited to diet and the prescription of vitamins. In fact, this point of view is completely unfounded. The social significance of hypothalamic syndrome is determined by a number of factors.
These include the young age of the patients, the rapidly progressing course of the disease, and pronounced neuroendocrine disorders, often accompanied by a decrease or loss of ability to work. The disease poses an even greater problem due to its impact on a woman’s reproductive function, leading to the development of secondary polycystic ovary syndrome, endocrine infertility and serious obstetric and perinatal complications. At the same time, many specialists, including gynecologists and endocrinologists, have a vague understanding of modern principles of treatment of hypothalamic syndrome, sometimes making gross and unforgivable mistakes. That is why the report presented by Honored Doctor of Ukraine, Professor, Doctor of Medical Sciences Svetlana Ivanovna Zhuk within the framework of the scientific and practical conference “Topical Issues of Endocrine Gynecology” (February 6-7, Kiev) could not remain without our attention.
– Hypothalamic syndrome of reproductive age, also known as diencephalic or neuroendocrine syndrome, is a symptom complex that occurs when the hypothalamic region of the diencephalon is damaged and is characterized by autonomic, endocrine, metabolic and trophic disorders.
It should be noted that the term “hypothalamic syndrome” is more correct, since in the diencephalic region of the diencephalon, in addition to the hypothalamus, other subcortical structures are localized, including the thalamus, epithalamus, and subthalamus.
It is currently generally accepted that the cause of the development of hypothalamic syndrome is the so-called hypothalamic stress that occurs after artificial or spontaneous abortions, after a pathological course of pregnancy and/or childbirth.
In healthy women, after childbirth or abortion, homeostasis gradually normalizes. Hypothalamic-pituitary-adrenal relationships and the gonadotropic function of the pituitary gland are normalized, and ovulatory cycles in the ovaries are restored. However, in a certain group of women, adaptation fails, hypothalamic stress develops, and subsequently hypothalamic syndrome.
As for the classification of hypothalamic syndrome, the division according to the etiological principle, clinical picture and nature of the course of the disease, according to its severity, is of practical importance.
Depending on the etiological factor, primary (due to central nervous system injuries and neuroinfection), secondary (associated with obesity) and mixed hypothalamic syndrome are distinguished. There are four clinical forms of the disease: with a predominance of obesity, symptoms of hypercortisolism, neuroendocrine disorders or neurocirculatory disorders. The diagnosis indicates the severity of the disease (mild, moderate, severe) and the nature of its course (progressive, regressive or recurrent).
The clinical picture of hypothalamic syndrome is dominated by the following syndromes:
• vegetative-vascular – 32%,
• metabolic and endocrine disorders – 27%,
• neuromuscular – 10%.
More rarely, thermoregulation disorders and other symptoms are observed (about 4%).
The presence of hypothalamic syndrome may be indicated by a combination of several signs: obesity (BMI more than 30 kg/m2), anovulatory ovarian hypofunction, menstrual irregularities of the hypomenstrual type, moderate hypertrichosis, proliferative processes of the endometrium, a tendency to hypertension, so-called diencephalic symptoms (headache, fatigue, hyperthermia, polyuria), hyperglycemia or impaired glucose tolerance, dyslipidemia. The pathogenesis of hypothalamic syndrome is not fully understood. No doubt
its connection with the pathological course of pregnancy and childbirth (or abortion). Adipose tissue also plays an important role in the pathogenesis of hypothalamic syndrome. It provides extragonadal synthesis of androgens and estrogens, the level of which clearly correlates with BMI. Thus, with an increase in BMI by 1 kg/m2, an increase in testosterone levels by 0.06 mmol/l is observed. In turn, an increase in this indicator leads to increased extragonadal synthesis of estrogens, which play an important role in the pathogenesis of hyperplastic processes in the endometrium. Visceral obesity makes a significant contribution to the development of insulin resistance, and subsequently diabetes mellitus and cardiovascular pathology. In recent years, the medical literature has increasingly emphasized the important role of obesity and insulin resistance in the pathogenesis of diseases of the female reproductive system, such as menstrual irregularities, infertility, polycystic ovary syndrome, and endometrial hyperplasia.
During the hypothalamic syndrome, two phases are distinguished (V.N. Serov, T.I. Rubchenko). In the first phase, ovarian function is disrupted, the synthesis of sex hormones and growth factors changes, and the menstrual cycle is disrupted. As a rule, after losing body weight due to diet and/or drug therapy, a woman’s menstrual function and fertility are restored.
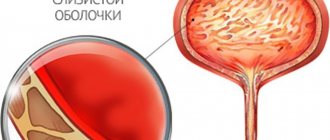
In the second phase, morphological changes in ovarian tissue begin and the ovulation process is disrupted. Subsequently, chronic anovulation leads to cystic atresia of the follicles, hyperplasia of theca and stromal cells, and the formation of secondary polycystic ovaries. Polycystic ovaries in hypothalamic syndrome (according to ultrasound) are enlarged in size, have a smooth surface, a thickened whitish capsule, through which multiple small follicles with a diameter of 2-4 mm are visible.
Most symptoms of hypothalamic syndrome are nonspecific, therefore, in the presence of the above signs, differential diagnosis with a number of other pathological conditions is mandatory. A thorough analysis of anamnestic data and the dynamics of the disease is necessary. The patient's examination plan should include the determination of luteinizing hormone, prolactin, follicle-stimulating hormone, testosterone, estradiol, cortisol, thyroid-stimulating hormone, thyroxine. Fasting glucose levels are measured in all patients and, if necessary, a glucose tolerance test is performed. Organic changes in the diencephalic region, primarily tumor processes, can be identified by radiography of the skull with a projection onto the sella turcica.
The examination complex is supplemented by electroencephalography or Dopplerography of cerebral vessels, ultrasound examination of the pelvic organs, thyroid gland and adrenal glands.
Patients with hypothalamic syndrome are managed by a gynecologist together with an endocrinologist and a neurologist. Important directions in the treatment of this pathology are the sanitation of foci of infection, normalization of work and rest, diet therapy and normalization of body weight.
In case of predominance of neuroendocrine syndrome, regulators of neurotransmitter metabolism are prescribed: diphenin 100 mg 2 times a day (regulates dopaminergic metabolism), bromocriptine 2.5-5 mg per day (regulates dopaminergic metabolism, normalizes the synthesis and release of not only prolactin, but also adrenocorticotropic hormone, LH, FSH). These drugs are prescribed for a course of 3-6 months.
In most cases, it is necessary to prescribe medications that improve cerebral circulation and bioelectrical activity of the brain, for example Cavinton_forte, 1 tablet 3 times a day for 1-2 months. An important component of treatment is vitamin therapy.
Acupuncture can be used as an alternative method.
Dehydration therapy plays a certain role in the treatment of hypothalamic syndrome. The patient can be prescribed Veroshpiron at a dose of 50-75 mg/day.
The course of treatment ranges from 2 weeks to 6 months depending on the clinical picture. Veroshpiron has not only a diuretic and antihypertensive effect, but also has an antiandrogenic effect (inhibits the synthesis of androgens in adipose tissue).
During the period of normalization of body weight and correction of metabolic disorders, it is recommended to protect against pregnancy, which in case of hypothalamic syndrome can be complicated by severe late gestosis. The choice of contraception in this category of patients is largely determined by the pathogenesis of the disease. Since disorders of the reproductive system occupy an important place in the picture of hypothalamic syndrome, the most rational choice in this case would be microdosed combined oral contraceptives (COCs), for example Lindinet 20, or gestagens (dydrogesterone) (V.I. Kulikov, V. I. Serov, 2007), which will have not only a contraceptive, but also a therapeutic effect.
The choice of a specific drug is based on the characteristics of the clinical picture of the disease, FSH and LH levels, and the LH/FSH ratio. First of all, you should pay attention to drugs that contain microdoses of ethinyl estradiol (20 mcg in 1 tablet), provide minimal hormonal load per dosing cycle, have 100% bioavailability, are not metabolized in the liver and, which is extremely important for hypothalamic syndrome, are metabolically neutral.
For oligomenorrhea, normal or slightly reduced estradiol levels and an LH/FSH index of less than 2, it is recommended to prescribe dydrogesterone 10 mg 2 times a day from the 16th day of the menstrual cycle for 10 days. The course of treatment is at least 6 months.
With oligomenorrhea against the background of severe
hypoestrogenism (LH/FSH index more than 22.5), it is recommended to take microdose COCs. The optimal choice for patients with hypothalamic syndrome may be the drug Lindinet 20, which is prescribed for at least 3-6 months.
We have been using this drug in our practice for a long time and have appreciated its high effectiveness and excellent safety profile.
It is Lindinet 20 that meets most of the criteria for choosing a contraceptive for hypothalamic syndrome. It is a metabolically neutral drug and does not affect body weight, blood pressure and glycemic levels. In this regard, Lindinet 20 can be prescribed even to women suffering from mild forms of diabetes. Very often, when treating hypothalamic syndrome, doctors make serious mistakes. Firstly, this is the prescription of hormonal drugs to regulate the menstrual cycle without adequate prior treatment of dysfunction of the diencephalic structures of the brain and normalization of body weight in case of obesity. Secondly, this is the use of high-dose COCs containing more than 30 mcg per tablet. It is absolutely unacceptable to prescribe dexamethasone, which only aggravates existing metabolic disorders associated with elevated cortisol levels.
According to a number of authors, Lindinet 20 is also an effective means for the prevention of hypothalamic syndrome (V.I. Krasnopolsky, O.F. Serova, V.A. Tumanova, N.V. Zarochentseva, 2005). Microdosed COCs (Lindinet 20) for the prevention of neuroendocrine disorders are indicated for the following categories of women:
• with a short period of breastfeeding;
• those who are obese;
• at early puberty;
• with thyroid dysfunction;
• having a history of concussion;
• with neuroinfections;
• who have a pathological course of pregnancy and childbirth.
Thus, treatment of hypothalamic syndrome should be individual, comprehensive and long-term.
Microdosed COCs occupy a special place in the therapeutic regimen of this category of patients. Thus, the drug Lindinet 20 can be recommended both for patients with hypothalamic syndrome and for women after childbirth who have no contraindications to hormonal contraception, in order to prevent postpartum neuroendocrine syndrome and protect against pregnancy. The drug can be used for a long time, right up to planning the next pregnancy, ensuring reproductive health in the intergenetic interval.
Prepared by
Natalya Mishchenko
“Do’s” and “Don’ts” for hypothalamic syndrome
Can:
- Physical education with a gradual increase in loads under the control of blood pressure and heart function;
- Diet with limited carbohydrates and fat;
- A regular daily routine that allows you to get enough sleep.
It is forbidden:
- Physical education without correction of high blood pressure;
- Living with high blood pressure (symptomatic arterial hypertension can persist and develop into hypertension);
- Allow body weight to grow (reducing excess weight will be more difficult than avoiding it);
- Irregular daily routine, lack of sleep (less than 7-8 hours).
Introduction
Hypothalamic puberty syndrome (HPPPS) is a complex endocrine pathology of adolescence, characterized by functional disorders in the hypothalamic-pituitary-adrenal-ovarian system [2]. This syndrome usually occurs in girls 1–3 years after menarche. Predisposing factors are psycho-emotional trauma, chronic foci of infection, frequent viral diseases, previous surgical interventions, and excessive mental stress [1, 4].
Adrenogenital syndrome
Adrenogenital syndrome occurs as a result of dysfunction of the adrenal glands and manifests itself in the form of virilization - the development of male characteristics.
Depending on the origin, there are two forms of adrenogenital syndrome:
- Congenital. Occurs as a result of hereditary disorders. Manifests itself in the form of changes in the external genitalia according to the male type. Sometimes in a maternity hospital the sex of a child is mistakenly determined to be male.
- Acquired. It is a consequence of excessive development of the adrenal cortex or (less commonly) its tumors. The girl develops masculine characteristics. There is no menstruation, the mammary glands decrease in size, a male-type physique is noted, hair growth on the face and in other uncharacteristic places.
Hypothalamic obesity
The nervous and endocrine systems “speak” different languages, but work together. There is a small organ in our body that perfectly “understands” both and serves as the main intermediary in their work. This is the hypothalamus. On the one hand, it is connected with key centers of nervous regulation - the cerebral cortex, amygdala, hippocampus, cerebellum, brainstem, and spinal cord. On the other hand, it regulates the functioning of the pituitary gland - the endocrine system. Control over the intake, processing and “targeted use” of food is also essential without the participation of the hypothalamus. Moreover, both from the “nervous” (feelings of hunger and satiety) and from the humoral (regulation of lipid, carbohydrate metabolism, etc.) mechanisms. It is not without reason that the hypothalamus is involved in disturbances of energy metabolism of any type.
Obesity is always a consequence of the dominance of energy “income” over “expense”. There are many reasons for this disharmony. But no matter which of them the disorders “start” with, over time a pathological cause-and-effect tangle is formed, covering a variety of regulatory mechanisms.
Hypothalamic obesity is a diagnosis when organic and/or functional lesions of the hypothalamus act as the primary trigger. As a result, there is an increase in the mechanisms of appetite stimulation (for example, an increase in the production of neuropeptide Y) and a suppression of the “feedback” system that inhibits it (for example, a decrease in the sensitivity of cells to the “controller” of energy metabolism - the hormone leptin). In addition, a shift in equilibrium also occurs due to a decrease in energy expenditure. Thus, the pathological basis for gaining excess weight is a simultaneous violation of both the flow of energy (food) into the body and its consumption.
The functioning of the hypothalamus can be disrupted by:
- congenital anomalies;
- tumors of the hypothalamus itself and organs associated with it anatomically and/or functionally (for example, hypothalamic hamartoma, craniopharyngioma, meningioma, etc.);
- head injuries and surgical interventions (including due to a persistent increase in intracranial pressure);
- infectious diseases of the central nervous system (for example, encephalitis, meningitis);
- systemic pathologies (for example, sarcoidosis, histiocytosis);
- congenital or acquired anatomical defects (for example, aneurysm).
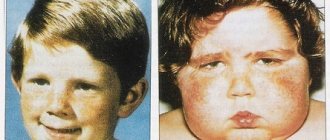
Signs of hypothalamic obesity
A characteristic feature of this type of obesity is a very rapid rate of weight gain, usually accompanied by a pronounced increase in appetite.
Hypothalamic obesity (HO) is also manifested by multiple changes in most organs and systems. This is explained by the direct and/or indirect participation of the hypothalamus in their work.
GO is accompanied by:
- changes in eating behavior;
- lethargy, drowsiness;
- imbalance of hormones of the reproductive system and disorders of its functioning (infertility, menstrual disorders, decreased potency);
- symptoms of malfunctions of the autonomic nervous system (impaired sweating, increased blood pressure, headache, etc.)
- endocrine disorders (hypothyroidism, type 2 diabetes);
- changes on the skin;
- visual impairment, etc.
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Appointment with an obstetrician-gynecologist with ultrasound examination (primary) | 4 200 |
| Endoscopic ovarian resection | 95 000 — 125 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Treatment of endocrine obesity
First of all, it is necessary to eliminate the root cause of obesity - specific hormonal dysfunction. For example, using hormone replacement therapy. Otherwise, the principles of treatment are similar to those given above.
A huge role is played by the patient’s motivation to get rid of the disease and awareness of its psychological causes. Therefore, psychotherapeutic assistance is not excluded.
Traditional medicine methods (instead of or together with classical ones) can also be used in the treatment of people suffering from obesity. Acupuncture, classical and resonant homeopathy, osteopathy, qigong therapy and herbal medicine have a holistic effect on a person, helping his body find and implement the optimal way to overcome the disease.
Make an appointment