Home / Pediatrician / Treatment of dystrophy in children
Dystrophy is a pathological process when tissues lose or accumulate substances that are not typical for normal indicators. The disease is accompanied by cell damage, which leads to serious changes in the functions of various organs.
The metabolism and structure of cells and tissues are disrupted. Dystrophy is most often diagnosed in children under three years of age. The consequences are delayed physical, mental, psychomotor development, as well as metabolic and immune system disorders.
What is dystrophy?
Dystrophy is structural changes in a tissue or organ caused by metabolic disorders within cells.
The most common dystrophies of the following tissues occur in the human body:
- fatty degeneration;
- muscular dystrophy;
- dystrophy of the myocardium (heart tissue).
Methods for diagnosing retinal dystrophy
More information about the clinical picture of the disease is provided by an integrated approach, which the specialists of Dr. Trubilin’s clinic use in their work. A complete diagnosis includes the use of the following methods:
- Visual acuity study.
- Carrying out measurements of intraocular pressure.
- Checking the fundus with a dilated pupil.
- Non-contact examination using optical coherence tomography (OCT). The technique is used to identify the causes and consequences of retinal diseases. Profile equipment allows the diagnostician to see the smallest sections of the central part of the organ being examined. Based on the information received, it is easier to assess real visual acuity. Screening is carried out with a laser beam or IR illumination. At the end of the diagnostic procedure, the patient receives a two-dimensional or three-dimensional image of the fundus.
Modern technology makes it possible to detect the earliest manifestations of the disease, which opens up good prospects for preventing the progression of disorders. Patients are encouraged to use simple self-diagnosis methods. You need to pay attention to the following signs:
- deterioration in the quality of vision when trying to look at any object at a distance or at close range;
- decreased visibility when reading or writing texts, if the same glasses that were used earlier are used for this;
- the desire to turn on the light brighter, to make the lighting more intense in a room where previously, under exactly the same conditions, this was not required;
- the appearance of a feeling that there is an obstacle in front of one of the eyes, impairing visibility, the spot has a fuzzy outline and is transparent to light, it cannot be removed with your hands or washed with water.
Any changes in the perception of the surrounding space should alert you: distortion of contours, colors, brightness. These signs are a good reason to contact an ophthalmologist. Patients are also recommended to use the Amsler mesh in accordance with the recommendations of the attending physician. This diagnosis is carried out for each eye separately.
Classification of dystrophies
The following types of dystrophy are distinguished:
- congenital,
- acquired.
Congenital dystrophies are genetic in nature and appear in early childhood. Dystrophies in children are very difficult. These include, for example, a fairly common type of muscle dystrophy - Duchenne dystrophy.
Duchenne dystrophy is a genetic disease transmitted from mother to son (the gene is located on the X chromosome). The child develops normally in the first years of life; the disease manifests itself between 3 and 5 years. First, difficulties arise when climbing stairs, then when walking, and later the respiratory and heart muscles are affected. The prognosis is unfavorable; there is currently no treatment for this pathology.
The most common types of dystrophies are:
- general (body mass index less than 16);
- local (of any organ).
Local dystrophies, for example, include:
- liver dystrophy;
- heart dystrophy;
- eye dystrophy;
- nail dystrophy.
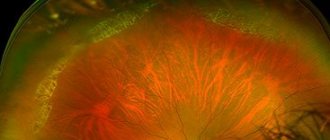
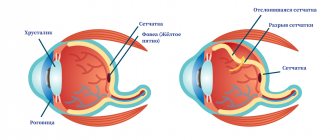
Retinal dystrophy is a whole group of diseases of varying severity. Some of them are quite harmless, while others lead to retinal detachment and blindness.
Retinal dystrophy can be congenital or develop with age. The reasons for their development have not been fully established, but among them are:
- severe myopia;
- diabetes;
- exophthalmos with thyrotoxicosis (an increase in the size of the eyeball with hyperthyroidism, as a result of which the vessels supplying the retina are compressed).
You can read more about hyperthyroidism in the Nutritionology blog.
Diagnostics
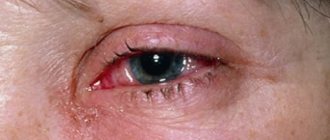
In terms of symptoms, corneal dystrophy does not differ from other ophthalmological diseases. Outwardly, it is similar to conjunctivitis, keratitis and other inflammatory processes: they are also accompanied by physical discomfort and decreased visual acuity. For a more accurate diagnosis, in addition to external examination and history taking, additional methods are used:
- biomicroscopy
- non-contact examination of the cornea using a slit lamp with multiple magnification; - pachymetry
- instrumental measurement of the thickness of the cornea over the entire surface of the anterior part of the eyeball; - visometry
is an instrumental assessment of visual acuity.
These methods are often sufficient to confirm the diagnosis, establish the type of pathology and determine the degree of its development.
Causes of dystrophy
The development of dystrophy is based on trophic disorders. Literally from the Greek the word “dystrophy” is translated as nutritional disorder. Congenital dystrophies are associated with mutations in certain genes; they are inherited by children from their parents and do not depend on external factors.
Acquired dystrophies are largely associated with environmental influences. For example, general dystrophy is the result of low nutrition or starvation. The cause of general dystrophy is often an eating disorder.
The mechanisms of development of local dystrophy are as follows:
- decreased blood flow to an organ or tissue;
- damage to the nervous system;
- mechanical injuries (for example, prolonged compression);
- action of physical factors (radiation);
- toxic effect.
A toxic effect is possible due to the action of substances:
- penetrating into the body from the environment;
- formed in the tissue itself as a result of the transition of one substance to another;
- synthesis in tissues of substances that normally should not be synthesized there;
- excessive entry into tissues of substances that in normal quantities do not have a toxic effect.
Demo lessons on the program “Nutriciology”
Get access
Main symptoms
Corneal dystrophy begins to manifest itself symptomatically quite quickly
: even with a small lesion, the patient feels discomfort in the eyes, reminiscent of fatigue from reading a book with small print for a long time, and a gradually increasing “fog” in the field of vision. As the disease progresses, these symptoms include:
- increased sensitivity to light;
- lacrimation;
- sensation of a foreign object in the eye;
- pain and cramps;
- redness of the cornea;
- visible swelling of the cornea;
- clouding of the eye (thorn).
The described symptoms are found in different combinations, and the intensity depends on the individual characteristics and type of pathology. Thus, the most severe symptoms are characterized by endothelial corneal dystrophy, while the marginal one does not clinically manifest itself until the cornea perforates.
Symptoms of dystrophy
Muscular dystrophy has the following symptoms:
- gradual painless decrease in muscle tone;
- reduction in muscle size (atrophy);
- decreased range of motion;
- loss of acquired skills in children (forgot how to hold a spoon, stand on one leg, etc.);
- severe weakness, fatigue, in young children - apathy, lethargy;
- frequent falls, instability, changes in gait;
- ordinary household load (climbing stairs, etc.) becomes prohibitive.
For other organs, manifestations of dystrophy are:
- reduction in size;
- structure changes;
- reduction in the volume of functions performed.
Progressive muscular dystrophies
Progressive muscular dystrophies (PMDs) are a heterogeneous group of inherited diseases characterized by progressive muscle weakness and skeletal muscle atrophy.
CLINICAL PICTURE
All PMD are characterized by muscle weakness of varying severity and muscle atrophy. The type of distribution of muscle weakness in PMD is one of the main diagnostic criteria. Each form of PMD is characterized by selective damage to certain muscles while sparing others nearby. In general, a typical myopathic symptom complex includes the following symptoms. • Symmetrical proximal muscle weakness of varying severity (muscle strength from 3-4 points in the early stages and up to 1-0 in the later stages of the disease), gradually developing muscle atrophy. • Govers' symptom: the patient, in order to rise from a squatting position, rests his hands on the floor, then rises, leaning his hands on his knees - “climbing on his own.” This early-onset symptom is caused by weakness of the muscles of the hips and pelvic girdle. • Difficulty walking up stairs - the patient helps himself with his hands. • “Duck” (waddling) gait associated with weakness of the pelvic girdle muscles. • Lumbar hyperlordosis, caused by weakness of the muscles of the pelvic girdle and back. • “Wing-shaped” scapula due to weakness of the serratus anterior muscle, as well as other muscles that fix the scapula. • Pseudohypertrophy of the calf muscles due to the development of connective tissue in them (muscle strength is reduced). • Walking on tiptoes due to Achilles tendon contractures. • Preservation of extraocular muscles, facial muscles. The myopathic symptom complex is most clearly identified in Duchenne and Becker PMD. • Duchenne PMD is characterized by an early onset of the disease (at 3-7 years), rapid progression, high CK levels, pronounced spontaneous activity according to needle EMG, and the absence of dystrophin in the muscles in immunohistochemical studies. As muscle weakness progresses, independent walking becomes difficult, and already at the age of 9-15, patients are forced to use a wheelchair, which provokes the development of kyphoscoliosis and osteoporosis. In the later stages, most patients develop dilated cardiomyopathy and weakness of the respiratory muscles. Intelligence is most often moderately reduced. • Clinical manifestations of Becker's PMD generally resemble those of the Duchenne form, but the course of the disease is milder: the onset occurs at a later age (from 2 to 21 years, on average 11 years), death occurs later (at 23-63 years ) . • Limb-girdle forms of PMD are also characterized by the development of a myopathic symptom complex. In terms of the age of onset of the disease, rate of progression and clinical manifestations, Erb's PMD resembles the Becker form, however, it is not characterized by cardiac pathology, in addition, the disease is noted in both boys and girls. In other limb-girdle forms, weakness of the facial muscles and cardiomyopathy are possible. • Landouzy-Dejerine PMD is characterized by severe weakness of the facial muscles (with the exception of a rare form without facial weakness), the symptom of “pterygoid” scapulae, weakness of the biceps and triceps brachii muscles with intact deltoid muscles, stepping. As a rule, the extraocular muscles (with the exception of one subtype) and the muscles of the tongue and pharynx, and the respiratory muscles remain intact. Some patients experience weakness of the pelvic girdle muscles (about 20% of patients are forced to use a wheelchair). Muscle atrophy is often asymmetrical. Many patients experience hearing loss, cardiomyopathy, or heart rhythm disturbances. • Emery-Dreyfus PMD is characterized by the presence of contractures (usually in the elbow, knee joints, and posterior neck muscles, due to which the head is slightly thrown back) and a scapulohumeral-peroneal distribution of muscle weakness and atrophy with preservation of the facial muscles. Cardiac arrhythmias and cardiomyopathy are common. The disease often debuts with contractures. • The main symptom of the ophthalmopharyngeal form is chronic progressive external ophthalmoplegia, followed by moderate bulbar syndrome. Subsequently, proximal muscle weakness develops in the arms and legs. • Distal myopathies are characterized by predominant weakness of the distal muscles. With Welander myopathy, the extensors of the hands are most affected; with Mioshi myopathy, the calf muscles are most affected: patients stand poorly on their toes and often stumble. With Govers' myopathy, tibial myopathy, the main symptom is stepping due to weakness of the peroneal muscle group, while Govers' myopathy is prone to further generalization: after 5-10 years, weakness of the hands and neck muscles is added, often about 1 toe and V on the arms . With tibial myopathy, which is common in Finland, isolated damage to the anterior tibial muscles is most often observed, and sometimes cardiomyopathy develops.
SYMPTOMS
With PMD Duchenne, Becker, limb-girdle forms, the most pronounced weakness is manifested in the lumbar-iliac muscles, muscles of the hips, deltoid, biceps and triceps muscles of the shoulder. Weakness in the distal muscles of the extremities is less pronounced. The facial muscles remain intact. Along with muscle weakness, hypotrophy of the affected muscles gradually develops, up to atrophy in the later stages. In this case, neighboring muscles can be completely clinically intact.
TREATMENT
Treatment should be carried out exclusively by a neurologist. Self-medication is unacceptable. There is currently no definitive treatment for PMD. The goal of treatment is to maintain muscle strength, prevent the development of contractures and joint deformities. Non-drug treatment Excessive physical activity, as well as insufficient physical activity, leads to an increase in muscle weakness. Daily exercise therapy helps maintain muscle tone and prevents the development of contractures. A physical therapy complex must include active and passive exercises, stretching exercises/contracture prevention exercises and breathing exercises. Active massage with muscle kneading can increase muscle weakness and fatigue, so a gentle massage is recommended. Patients tolerate physiotherapeutic treatment differently: some do not feel any improvement or even complain of increased muscle weakness. Surgical treatment In some cases, surgical treatment of contractures is possible, but it is necessary to remember the possibility of increasing muscle weakness during rehabilitation treatment (up to loss of the ability to walk). In some cases, implantation of a pacemaker is necessary.
Diagnosis and treatment of dystrophies
Because Most types of dystrophies are of genetic origin; diagnosis is made using a blood test for the presence of DNA mutations.
Help for such patients is provided in clinics specializing in the treatment of muscular dystrophies. Quite often a consultation with a neurologist is required. Particular attention is paid to the function of the lungs and heart, for which regular diagnosis of cardiopulmonary disorders is carried out.
Unfortunately, currently treatment for congenital muscular dystrophies is palliative and aimed at improving the quality of life. However, research institutes are constantly developing new promising treatment methods: muscle tissue transplantation, injection of antibodies, gene and hormonal therapy.
Dystrophies of individual organs can be treated quite successfully. Diagnosis and treatment are carried out by a highly specialized doctor, for example, an ophthalmologist or dermatologist. For treatment, local medicines containing vitamins and amino acids are used. Physiotherapeutic methods are used to improve blood flow.
Nutritional correction is also carried out. Nutrition plays a huge role; it must be complete and balanced. To create a diet, you can consult a dietitian or nutritionist.
Causes of the disease
Age-related macular degeneration, also called retinal dystrophy, is a chronic disease with a progressive course. Medical statistics over the past 10 years have shown that AMD is one of the top three diseases responsible for decreased vision and blindness in patients whose age exceeds 50-55 years.
It is difficult to single out a single cause of pathology. The anomaly is triggered by a number of factors, the most common of which are:
- Old age - an increase in risk is observed in the period from 50 to 80 years. However, in recent years, the disease has become significantly “younger”, as it increasingly began to appear in people of working age.
- Gender - the female half of society is more susceptible to degenerative changes in the retina. Men are 50% less likely to have such disorders.
- Genetic prerequisites - it is noted that AMD in direct relatives increases the risk of developing the disease.
- Pathologies of the heart and blood vessels - patients with changes in blood pressure, atherosclerosis of vascular structures and other similar disorders should be careful, since the risk of eye damage is very high.
- Excess ultraviolet radiation - prolonged exposure to the sun on unprotected eyes is as dangerous as prolonged exposure to laser or ionized radiation.
Additionally, among the provoking factors for the development of retinal dystrophy, experts indicate smoking, diabetes, poor nutrition with a lack of vitamins and nutrients. Poor ecology, injuries and eye surgeries can affect health.
Dental practice ORIS
Dear readers! I invite you to a consultation with a periodontist. Today we will talk about the manifestations of dystrophy in the oral cavity. Dystrophy is a violation of trophism, that is, tissue nutrition. Osteodystrophy is characterized by a weakening of the crystalline structure of the bone tissue of the jaws, hard tissues of the teeth, a decrease in its density and volume, replacement with fibrous tissue, and, as a result, a pronounced decrease in local immunity.
In the oral cavity, clinical signs of dystrophy are exposure of roots, formation of periodontal pockets and wedge-shaped defects, increased sensitivity and pathological abrasion of teeth.
When I, the periodontist ORIS, proceed to reveal the causes of these diseases, patients perceive my words with doubt: is everything really that big? Is everything really so closely connected? And can all problems really be “read” by their teeth? To understand the cause-and-effect relationships, let's step back and consider any work team. If the cleaner did the cleaning improperly or completely ignored it, the workers’ mood at the sight of dust and debris will be spoiled and depressed, and this will affect their performance and productivity. From dust and compressed air, oxygen starvation will develop, your head will hurt, and with it all problem areas (teeth, gums, joints, spine). Another example: your boss is angry! It's not good for anyone, is it? Increased nervous tension will lead to a powerful surge of adrenaline, a rise in blood pressure and will manifest itself as pain in the wisdom tooth, itching in the gums, and “threading” in multi-rooted teeth, because the oral cavity has a monosynaptic connection with the brain. That is, electrical impulses during periods of brain and nervous tension directly enter the nerve plexuses of the oral cavity, causing pain and discomfort. This is the body's protective reaction to stress. The principle is simple: if a person is in pain, he strives to eliminate and block all irritating factors - this is the instinct of self-preservation. EVERYTHING in the world is interconnected! And in the body, all organs and systems depend on each other and always act together. Remember the article “Immunity” .
Well, the reasons for the clinical manifestations of dystrophy in the oral cavity
lie in poor nutrition, physical inactivity, unbalanced physical activity, unbalanced bite, circulatory disorders, innervation, hormonal changes and disruptions, taking “dopings” and medications, and general diseases.
In each specific case, you need to understand and look for ways to solve the problem. Finding out the reasons requires time, the interest of the doctor and the patient in the final result, professional knowledge and strength, and restructuring the initial conditions will take years, dedication, discipline and motivation of patients.
You have severe periodontitis,
with pronounced atrophy (loss) of the bone tissue of the jaws (in the area of individual teeth the bone tissue is almost completely lost), with severe exposure (2/3 or more) of the roots, the presence of wedge-shaped defects, increased sensitivity and mobility of the teeth, an unbalanced bite, poor circulation and tissue trophism. Complex treatment of such a patient will be quite complex and lengthy, because it is vital to change the destructive, pathological “scenario” of oral cavity degradation! We must act actively and immediately - this is obvious, isn’t it?!
Here is another example of severe periodontitis with pronounced atrophy of the bone tissue of the jaws, exposure of the roots of the upper teeth - 2/3, lower - 1/3 of the length, wedge-shaped defects, unbalanced bite, mobility of all teeth of varying degrees, with impaired blood circulation and tissue trophism .
This clinical case is also not easy. In addition to professional difficulties, one has to overcome “pathological” principles of consciousness and worldview, prejudices and misconceptions, and previous negative experiences of patients. The more confused and neglected everything is, the more difficult it is to “restore order” to the oral cavity and give the patient a completely new quality of life! Don't let yourself go! Listen to our advice!
Today we will look at the common causes of dystrophy in the oral cavity, which you can eliminate.
The NUTRITION of modern people is depleted in proteins, microelements and vitamins; in most cases it cannot be called balanced. We informed you about the principles of proper nutrition in the article “Food Hygiene”. Remember it and pay attention to the weekly diet of families from different parts of the world and compare it with yours. Nutrition needs to be reviewed every new season of the year, making significant adjustments. It is necessary to carefully plan your diet every week and keep a food diary for analysis and control. Most often I hear: “My wife cooks deliciously, but it’s not healthy” or “Everyone has gastritis!”, “I’m already 50, and I don’t want to eat only grass!”, “My mother didn’t teach me to eat differently,” “Mom didn’t teach me to cook differently.”
My friends, your mother cannot teach you everything, but she gave you life and the opportunity to improve
non stop !!!
I dedicated an entire section of the Dental Health blog to PHYSICAL ACTIVITY . I will briefly express fundamental thoughts: your physical exercises will be effective, that is, healthy, only if: preliminary stress relief - alignment - according to the principles of Pilates; proper warm-up, with the preparation of all major joints; systematic progressive training methodology (from simple to complex); varied weekly physical activity (Pilates, cardio, strength training), cool-down with elements of stretching and yoga breathing practices. Don't allow physical inactivity into your happy life! Take walks in the fresh air every day and don’t forget to chew properly, as I taught and teach you! Remember my article “Experiment”.
GENERAL HEALTH
we must preserve and strengthen all life. This is our duty to the Motherland and duty to our family!
And the prevention of all diseases lies in nutrition, physical activity, and timely elimination of functional disorders so that they do not become organic. For example, sedentary work must be compensated by walking, swimming, fitness, otherwise osteochondrosis will develop, compression of the neurovascular bundles of the neck will occur and will lead to impaired blood circulation and trophism of the oral cavity, periodontitis, atrophy of the bone tissue of the jaws and, ultimately, loss of teeth! Bleeding gums and bad breath must be eliminated in time, before the inflammatory process affects the bone tissue of the jaws and weakens your immunity! Dental health reflects the real state of functioning of the organs and systems of the body, their balance and interaction. Don’t be like the bureaucratic management system: “I don’t see anything, I don’t hear anything, I won’t tell anyone anything.”
Change behavioral stereotypes, think, delve into it, help yourself under the strict guidance of a dentist.
Be active and proactive, understanding and hardworking!
DEFEND YOUR RIGHT TO A HAPPY LIFE!