Get an online consultation with our specialist right now! You can ask any question you are interested in. For a more accurate answer, attach the MRI results
Online consultation
Due to its anatomical structure, the joint can perform a wide variety of movements in any plane, it is susceptible to injury, and the most common injury is shoulder dislocation .
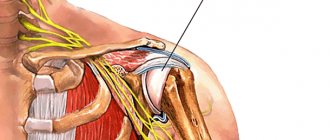
The joint has a spherical shape. Formed by the glenoid cavity of the scapula and the head of the humerus. It is important to note that the area of the articular surface of the scapula is significantly less than the area of the head of the humerus. If you imagine a bull's eye (the head of the shoulder) that rolls on a plate (the glenoid cavity of the scapula), then the bull's eye is very large, and the plate is very small (ratio 1X4).
Significantly increasing the stability of the head in the scapula cavity is the articular labrum, which increases the area of contact of the humeral head with the scapula.
Mechanism of injury
The shoulder is a complex structure that belongs to the ball and socket joints. It provides a significant range of movements of the upper limb in various planes. Features of the functions of the joint and its anatomical structure are factors that provoke the formation of dislocation.
It is an injury in which the head of the humerus comes out of the glenoid cavity. The main mechanism for the development of injury is excessive mechanical impact with stretching or rupture of reinforcing ligaments.
Causes of shoulder dislocation
We have already mentioned that the shoulder joint is characterized by great mobility. A person most often “operates” precisely this part of the skeleton. He is very vulnerable, and most often he is struck by a disease such as dislocation. Its frequent cause is the provision of a general force effect, the movement itself is inverting or twisting in nature. To lead to injury, it must be performed with a simultaneous violation of the range of all possible joint movements.
There are other reasons and factors:
- Excessive movement directed at this part of the skeleton is diagnosed in 12% of cases, and this type of health disorder is called “joint hypermobility.”
- Posterior or anterior varieties appear for various reasons, but most often due to the fact that the glenoid cavity is strongly inclined.
- If the scapular glenoid cavity has a small capacity, the cause changes noticeably, and the risk factor for dislocation increases.
- A common cause is hypoplasia of the glenoid cavity, that is, mostly its lower region changes, and many other physiological changes also occur.
- Often people are forced to repeat the same type of movements, and because of this, the ligaments and joint capsule are repeatedly stretched. Among the patients, in this case, most often are athletes (swimmers, handball players, etc.)
A particularly high risk is associated with excessive range of motion. In medicine, this type of movement is called “generalized hypermobility.” There are a number of reasons related to the anatomical features of the joint structure. Then you should conduct research in advance and avoid traumatic situations.
Shoulder dislocation. Kinds
Shoulder dislocation.
Types Dislocation of the shoulder joint is a polyetiological injury. This means that its development is provoked by a significant number of different causative (etiological) factors, which, for ease of diagnosis, were divided into several main groups:
- Excessive mechanical impact - pronounced extension or abduction of the arm, exceeding the stabilization capabilities of the ligaments, leads to damage (usually in the form of sprain) of the ligamentous apparatus and the exit of the humeral head. Typically, factors leading to excessive stretching occur in individuals with fairly high mobility and loads on the upper limbs (athletes, representatives of professions requiring physical effort).
- Weakening of the ligamentous apparatus of the shoulder, which may be congenital (the result of changes in the functional state of certain genes) or acquired (a consequence of chronic inflammation or degenerative processes) of origin. In this case, dislocation of the humerus can develop even against the background of normal loads.
- A combination of increased load on the shoulder with weakening of its ligamentous apparatus, which leads to habitual popping in the future.
Determining the cause that led to the prolapse of the humeral head is a priority measure for determining further treatment and diagnostic tactics, as well as preventing injury in the future.
Conservative therapy
The primary measure of conservative treatment for habitual shoulder dislocation is modification of the patient’s life and behavior. The load on the shoulder joint is temporarily limited to ensure sufficient restoration of the ligamentous apparatus. If there is a significant inflammatory reaction, non-steroidal anti-inflammatory drugs are prescribed.
In the future, physiotherapeutic procedures are used. These include magnetic therapy, mud baths, electrophoresis with drugs. An alternative modern option for conservative therapy is the intra-articular injection of platelets containing “growth factors”. They stimulate the processes of restoration of the fibers of the ligamentous apparatus. The effectiveness of conservative therapy is assessed several months from the start of its implementation.
Kinds
Depending on the impact of the main causative factor, traumatic and pathological dislocation are distinguished. Traumatic exit of the humeral head is divided into 2 types according to the age of development:
- Acute (first) shoulder release, which usually has a traumatic origin.
- Habitual shoulder release, developing as a result of pathology with weakening of the ligaments or improper treatment of the primary injury.
Separately, congenital miscarriage is distinguished, which can also be the result of a complicated course of labor and improper extraction (forced removal from the birth canal) of the fetus.
Rotator cuff injuries
Rotator cuff tendon damage can occur for several reasons:
- degenerative changes;
- narrowing of the space between the acromion and the head of the humerus;
- injury;
- chronic traumatization.
Degenerative changes are associated with poor circulation of the rotator cuff tendons, the aging process and tissue wear, as well as qualitative changes in the collagen fibers in the tendons.
Narrowing of the space between the acromion and the head of the humerus (impingement syndrome) occurs due to the special structure of the acromion process or after injury. The tendon of the supraspinatus muscle, passing through this space, falls into a vice, as it were, and is gradually compressed.
Typical injuries are a fall on the shoulder joint or on an outstretched arm, a sudden lifting of a heavy object, or a sudden movement of the arm to the side.
Frequent microtraumas of the shoulder joint area occur in people with heavy physical labor and throwing athletes. Typical professions include those whose work involves prolonged hand position at level 900 and above. These are, for example, hairdressers, dentists, electricians, carpenters, painters.
Symptoms of a rotator cuff tear.
Small tears or partial damage may be asymptomatic. But most often the leading symptom is pain. When an injury occurs, pain occurs sharply, and with repeated stress it intensifies gradually and increases over time. The greatest intensity of pain is determined when the arm is abducted in an arc from 600 to 1200. Periodically, the pain intensifies at night and leads to sleep disturbance.
During the examination, a decrease in muscle strength of the injured limb can be detected. Painful sensations limit the range of motion in the shoulder joint and lead to the development of contracture (stiffness).
Conservative treatment
Partial injuries to the rotator cuff tendons can occur on the articular surface, on the acromion side, or within the tendon. It is advisable to start treatment with conservative methods. The main task is to eliminate the cause of the pathological process and stop inflammation. The patient needs to reduce his physical activity. The doctor prescribes anti-inflammatory drugs, physiotherapy, and exercise therapy. In the absence of confirmation of a full-thickness tear, it is possible to administer subacromial corticosteroid drugs to relieve pain and reduce inflammation.
Recently, much attention has been paid to the possibility of tissue regeneration. As a modern alternative method of non-surgical strengthening of the soft tissue structures of the shoulder, intra-articular injection of platelet-rich plasma (PRP) in combination with shock wave therapy (SWT) is used. Conservative treatment is also considered as a preparatory stage before surgery.
Operation
A full-thickness tear can affect one tendon or several. Massive injuries of the rotator cuff in some cases are characterized as irreparable and require open surgery to plastically replace tendon defects or move other muscles to the rupture zone.
Bioabsorbable implants Titanium implants
For the majority of ruptures, modern arthroscopic suture technologies are used. Arthroscopy is performed under endotracheal anesthesia, which can be combined with conduction anesthesia of the brachial plexus nerves. On the operating table, already under anesthesia, the patient is placed in the “beach chair” position. Arthroscopic intervention involves making 4-5 5mm punctures around the perimeter of the shoulder joint, into which a camera and microsurgical instruments are inserted. With their help, the tendon is decompressed, the subaromial space is cleaned and expanded. The tendon suture is performed after installing special screws (anchors) with non-absorbable threads attached to them into the head of the humerus. Using threads, the tendons are stitched and fixed in the head of the humerus.
The best results of surgical treatment of a rotator cuff tear are observed within up to 3 months from the moment of injury.
Shoulder dislocation
Shoulder dislocation
The main clinical symptom of humeral head dislocation is pain. At the first dislocation it has significant intensity. Immediately after the injury, the shape of the shoulder joint changes (deformation) with the formation of a bulge in the area where the head emerges.
Inflammatory signs develop, the skin becomes red (hyperemia) and swollen. With a complicated injury, if blood vessels and nerve trunks have been damaged, bruising often appears and numbness develops, which spreads to the skin of the upper limb.
The first dressing after arthroscopic Latarjet surgery.
The video shows the patient's first dressing after surgery. Small skin punctures, low trauma, moderate pain, and the ability to move the arm from the first day after surgery are the undeniable advantages of the arthroscopic intervention technique over the standard open method.
36 days after arthroscopic Latarget surgery.
36 days after arthroscopic Latarget surgery.
After Latarjet, first dressing
After Latarjet, X-ray control – the position of the bone block is ideal
First aid
Correct provision of care at the prehospital stage determines the effectiveness of treatment and recovery in the future, as well as the prevention of complications. It involves immobilizing the arm bent at the elbow (it is better to use a scarf for this), as well as reducing the inflammatory reaction by applying cold to the skin of the injury area.
After completing such measures, you should definitely seek qualified medical help as soon as possible. It is not recommended to perform self-reduction of a dislocation at home, as this can cause serious complications.
Diagnostics.
Diagnosis of a dislocation includes a detailed examination of the patient, palpation of the damaged joint and the appointment of x-rays in two projections of the damaged joint. Using the obtained x-ray, the doctor identifies the type of dislocation, whether there is a fracture, and determines the method of reduction. In more serious cases, the doctor may prescribe computed tomography and magnetic resonance imaging to clarify the diagnosis. If there are serious injuries, consultation with a surgeon is necessary.
What to do if these symptoms occur?
If the patient has every reason to believe that he has a dislocation, then the first step is to contact a specialist. You cannot adjust the joint yourself, as this can lead to dire consequences: even greater trauma to the joint tissue, nerve damage, loss of motor function and sensitivity of the upper limb. Only a specialist can correctly assess the injury and prescribe the appropriate course of treatment. The sooner the victim is seen, the easier it is to solve the problem and the greater the chance of avoiding complications. As the day passes, muscle contraction will occur, making it more difficult to act promptly on the affected area. When transporting the patient to a doctor's appointment, the limb should be fixed in the position in which it was dislocated. You should not perform a reduction if the victim cannot return it to the reverse position on his own. To reduce pain, apply a cold compress to the injury site. To make an accurate diagnosis, it is necessary to explain in detail how exactly the incident happened.
Physiotherapy
Experts strongly recommend undergoing physical therapy procedures for dislocations. Since it allows you to restore motor function, as well as strengthen muscle tissue that was damaged by injury. This procedure is absolutely harmless and cannot cause harm to the patient. Physiotherapy is an effective procedure that has the following effects:
- aimed at relieving swelling at the site of injury;
- significantly reduces pain;
- is able to resolve blood clots that have formed in tissues;
- improves blood circulation;
- organs and tissues receive oxygen in full;
- The healing process takes place much faster.
Paraffin treatments also have a positive effect. Typically, physical therapy is prescribed a few days after the injury occurs.
Pathology of the tendon of the long head of the biceps
Pathology of the long head of the biceps tendon often accompanies other conditions, such as: SLAP injury, impingement syndrome, ruptures of the supraspinatus and subscapularis tendons. However, even an isolated violation of the integrity of the biceps tendon can lead to dysfunction of the upper limb and requires surgical treatment.
The human biceps muscle consists of a long head, which is attached to the upper segment of the articular surface of the scapula, and a short head, which is attached to the coracoid process of the scapula. The short head bears the main load, while the long head gives the characteristic contour to the arm. When the tendon of the long head of the biceps is completely ruptured, a characteristic clinical picture occurs. The long head falls down, as a result the contour of the shoulder is deformed. This symptom is named after the famous cartoon character Popeye due to its resemblance to the hands of a sailor.
Persistent pain syndrome is supported by partial damage to the integrity of the tendon, the development of chronic tendonitis, and tendon instability in the intertubercular groove. It is difficult for the patient to perform rotational movements in the shoulder joint, push-ups and pull-ups. Pain localized in the anterior part of the joint is often accompanied by clicking sounds.
Treatment begins with conservative methods similar to SLAP injuries. To quickly relieve inflammation, a therapeutic blockade is often used. To the tendon area
An anesthetic solution with Diprospan is injected under ultrasound control. The effect is achieved quite quickly, however, in order to prevent relapse, compliance with the treatment regimen and physiotherapeutic treatment is necessary.
If conservative treatment is ineffective, the question of surgical intervention is raised. The development of technology has left no room for open surgery in this matter - all manipulations are performed under the control of an arthroscope through punctures.
The techniques used are varied and combined during the operation: debridement of the tendon (i.e., grinding of it and surrounding tissues), correction of concomitant pathology, subacromial decompression. Tenodesis of the long head of the biceps tendon is recommended for young active patients and athletes. This manipulation is performed at different levels of the intertubercular groove using arthroscopic implants. After fixation to the head of the humerus, the intra-articular part of the tendon is excised. For elderly patients, the method of choice is tenotomy - cutting off the tendon from its attachment to the scapula. This is a simpler method, but no less effective. However, in the postoperative period, Popeye's symptom may develop, about which the patient must be warned in advance.
If there is a complete rupture in a young patient, the first thing to think about is surgical treatment. The essence of the operation is to isolate the torn tendon and fix it to the anterior surface of the head of the humerus (tenodesis) in the intertubercular groove. The operation can be performed either arthroscopically or through an incision.
Health-improving gymnastics complex
Perhaps the most important element of the recovery process is physical activity. The set of classes is aimed at quick and effective recovery of the injured organ after surgery. Health-improving gymnastics will help tone muscle tissue, improve blood circulation, and also stabilize the condition of the shoulder joint.
The very next day after realignment of the shoulder joint, the patient needs to begin health-improving procedures. Since the dislocated joint is completely immobilized, it is necessary for blood to flow into it. Therefore, it is recommended to conduct passive therapeutic exercises:
- with the hand of the injured limb you need to make circular movements in different directions;
- apply compression with the same limb, but at the first stage you cannot use weighting objects - this can cause injury;
- try to tense the muscles, while the joint itself should remain motionless.
After day 20, you can do slightly more complex exercises. By this time, the tissues and ligaments should gradually become stronger. In this case, the lesson is already carried out without a fixing bandage.
All movements are performed with the injured hand:
- the lesson must begin with a warm-up in order to tone the muscles and prepare them for a more complex load;
- in the first exercise it is necessary to tilt the shoulder joint forward, this leads to flexion of the ligaments;
- in the second exercise it is necessary to move the joint back, this is necessary to straighten the ligaments.
When performing the complex, you must adhere to a moderate pace. There is no need to rush, as you can accidentally damage the organ. The lesson should last no more than half an hour, but the entire set of exercises must be performed about 5 times a day. If performed systematically, the effect of the exercises will occur much earlier, and the damaged joint will quickly restore its functionality.
After 30 days, the patient usually removes the bandage if there are no complications, and the recovery process occurs according to the treatment. When performing a gymnastic set of exercises, it is necessary to be careful and not make sudden movements so as not to harm your hand. Most often, doctors prescribe the following exercises:
- it is necessary to perform active actions with the shoulder joint back and then forward;
- in order to improve blood flow, you need to work with your fingers, so it is imperative to perform exercises on flexion and extension of the lower part of the limb;
- It is also necessary to include in the lesson an exercise for raising and lowering the arm - this will allow you to develop the shoulder joint;
- the patient should perform exercises to rotate the limbs;
- It is recommended to raise your arms to the sides, as well as behind your back.
Physical activity can be gradually increased, but the exercises should not cause discomfort or pain. If this happens, then it is necessary to exclude this exercise until the recovery process is completed. All classes must be carried out daily, then the result will be noticeable. And the person will be able to quickly restore lost motor function. However, you must remember that you cannot strain the shoulder joint too much; all exercises must be done in moderation.