The term “chronic cor pulmonale” refers to changes in the heart muscle caused by lung diseases. This excludes cases of pathology complicating diseases of the heart and large vessels (mitral stenosis, cardiosclerosis after a heart attack, congenital defects, dilated cardiomyopathy).
In diagnosis, an indispensable condition must be a primary violation of the structure of the lung tissue and its functions. The prevalence of the recorded pathology among the adult population allows us to place it in third place after ischemic and hypertension diseases.
In the International Classification of Diseases (ICD-10), types of chronic pulmonary heart disease are included in the general class of cardiovascular diseases. Codes I26, I27, I28 differ in etiological factors. All cases are united by the gradual formation of overload of the right side of the heart due to the development of high blood pressure in the pulmonary circulation.
Causes
Depending on the causes, the WHO Expert Committee has developed a classification of chronic pulmonary heart disease. Diseases are divided into 3 groups:
- group 1 - diseases associated with impaired passage of air through the alveoli, these can be mechanical obstacles (bronchial asthma), inflammatory lesions (tuberculosis, chronic bronchitis, bronchiectasis, pneumoconiosis), replacement of lung tissue with fibrous tissue (systemic lupus erythematosus, sarcoidosis, eosinophilic infiltration ), a total of 21 nosologies are included;
- group 2 - diseases that impair ventilation of the lungs by affecting the auxiliary mechanisms of breathing (skeletal skeleton of the chest, ribs, muscles), this includes curvature of the spine, adhesions in the pleural cavity, chronic diseases associated with impaired neuromuscular conduction (poliomyelitis) , artificial hypoventilation after surgical interventions on the chest organs;
- group 3 - vascular lesions of the lungs (arteritis, thrombosis and embolism, compression of the main vessels by a tumor, aortic aneurysm and others).
All risk factors for underlying disease accelerate and negatively affect the heart.
What happens in the body
In patients of groups 1 and 2, all changes develop due to spasm of small arterioles in the lung tissue as a reaction to insufficient oxygen supply. In group 3, in addition to spasm, there is a narrowing or blockage of the vascular bed. The pathogenesis of the disease is associated with the following mechanisms.
- Alveolar hypoxia (lack of oxygen in the alveoli) - scientists associate vascular spasm in response to hypoxia with disturbances in sympathoadrenal regulation. There is a contraction of vascular muscles, an increase in angiotensin-converting enzyme (ACE), calcium in the blood, and a decrease in relaxation factors of the pulmonary vessels.
- Hypercapnia - an increase in the concentration of carbon dioxide in the blood does not directly affect the vascular wall, but through acidification of the environment and a decrease in the sensitivity of the respiratory center of the brain. This mechanism enhances the production of aldosterone (adrenal hormone), which retains water and sodium ions.
- Changes in the vascular bed of the lungs - compression and emptying of capillaries due to developing fibrous tissue is important. Thickening of the muscular walls of the pulmonary vessels contributes to the narrowing of the lumen and the development of local thrombosis.
- An important role is played by the development of anastomoses (connections) between the bronchial arteries, belonging to the systemic circulation, and the pulmonary vessels.
- The pressure in the systemic circle is higher than in the lungs, so the redistribution goes towards the pulmonary vascular bed, which further increases the pressure in it.
- In response to hypoxia, blood cells that carry hemoglobin and erythrocytes change. Their number increases simultaneously with platelets. Favorable conditions for thrombus formation are created and blood viscosity increases.
All taken together leads to increased load on the right ventricle, hypertrophy, and then failure of the right heart. An enlarged right atrioventricular orifice contributes to insufficient closure of the tricuspid valve.
How does CHF develop?
Congestive (chronic) heart failure is a condition that affects the heart's ability to pump blood throughout the body. Affecting one or both sides of the heart, the disease can cause:
- fatigue and shortness of breath;
- swelling of the feet and ankles;
- accumulation of blood and fluid in the lungs.
Weakened heart muscle, heart valve disease, or chronic hypertension (high blood pressure) are common causes of heart failure. The most common cause of heart muscle weakness is damage due to myocardial infarction (MI). A MI is a life-threatening condition that occurs when an artery supplying blood to one or more heart muscles becomes blocked. The result is damage to the heart muscle and a decrease in the heart's pumping ability, which is described as heart failure.
High blood pressure, elevated fat and cholesterol levels, and smoking damage and clog the arteries supplying the heart muscle.
CHF significantly reduces the quality of life of patients with COPD.
Clinical course
Soviet pulmonologists B. Votchal and N. Palev proposed a clinical description of the stages of development of the pulmonary heart:
- in the initial (preclinical) stage - there are no symptoms of hypertension in the pulmonary circulation, hypertension is possible temporarily with an exacerbation of pulmonary disease;
- in the second stage - there is right ventricular hypertrophy, but all signs are compensated; instrumental examination reveals stable pulmonary hypertension;
- third stage - accompanied by decompensation (pulmonary heart failure), there are symptoms of right ventricular overload.
Clinical manifestations
At the early stage of the disease, the manifestations of chronic pulmonary heart disease do not differ from the typical symptoms of major pulmonary diseases. They intensify with exacerbation and are treatable.
Shortness of breath is a consequence of oxygen deficiency, but it also accompanies inflammation of the lung tissue, emphysema. The intensity does not always correspond to the degree of hypoxia.
Changes in the phalanges occur due to impaired nutrition of the periosteum
Tachycardia is a nonspecific symptom; the heart rate increases in various diseases that are associated with an activated sympathetic nervous system and increased release of adrenaline.
Chest pain is not similar to angina. They are believed to be caused by insufficiency of the coronary vessels, which have to feed the thickened muscle of the right ventricle. Spasm of the arteries of the heart and intoxication of the myocardium with inflammatory products are also important.
Increased fatigue and weakness occur when the shock capacity of the heart decreases. Peripheral tissues of various organs, including the brain, lack blood supply.
Heaviness in the legs, swelling - in addition to myocardial weakness, an increase in the permeability of the vascular wall plays a role. Swelling occurs on the feet and legs. They intensify in the evening and subside during the night. In the third stage, they spread to the thighs.
The feeling of heaviness and pain in the right hypochondrium is caused by an enlarged liver and stretching of its capsule. In a severe form of the disease, ascites simultaneously appears and the abdomen “grows” rapidly. This symptom is more pronounced in elderly patients with concomitant atherosclerosis of the abdominal arteries.
A cough with a small amount of sputum is more associated with the underlying pathology of the lungs.
Manifestations of encephalopathy - chronic lack of oxygen and excess carbon dioxide cause pathological disorders in the brain, disrupt vascular permeability, and promote edema. Patients have 2 possible symptoms:
- increased excitability, aggressive behavior, euphoria, development of psychosis;
- lethargy, lethargy, indifference, drowsiness during the day, insomnia at night.
In severe cases, seizures occur with loss of consciousness or dizziness, cold sweat and decreased blood pressure.
Classification
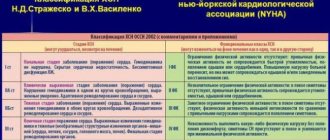
Today there are several classifications, including such authors as B. E. Votchal (pulmonary heart disease) and N. R. Paleev (pulmonary hypertension in COPD). They are successfully combined, and three stages are distinguished.
- Stage I - transient - an increase in pulmonary arterial pressure is observed during physical activity, often the condition is caused by an exacerbation of the inflammatory process in the lungs or worsening bronchial obstruction
- Stage II - stable - pulmonary arterial hypertension is now observed not only during exercise, but also at rest, and is not associated with exacerbations of pulmonary pathology
- Stage III - pulmonary hypertension is stable, circulatory failure also develops
Diagnostics
In people with chronic cor pulmonale, the diagnosis can be suspected by their appearance: in the compensation stage, dilated skin vessels appear in the cheek area (blush) and on the conjunctiva (“rabbit eyes”). Cyanosis is found on the lips, tip of the tongue, nose, and ears.
When examining the fingers, changes in the nail phalanges are visible: they become flat and widened (“drumsticks”). Unlike heart failure, the arms and legs remain warm to the touch.
Swollen veins in the neck indicate the formation of stagnation at the level of the veins of the systemic circulation, more pronounced at the height of inspiration
When auscultating the heart, the doctor hears:
- characteristic changes in tones above the pulmonary artery;
- in the stage of decompensation - a murmur indicating insufficiency of the right atrioventricular valve;
- a lot of different types of wheezing in the lungs against the background of altered breathing.
The x-ray reveals a typical bulging of the contours of the pulmonary artery, an enhanced tissue pattern, and an expansion of the zone of lymphatic vessels. This indicates an increase in pressure in the pulmonary circle. In the decompensation stage, the heart shadow expands to the right.
Echocardiography assesses the strength of the right ventricle, the degree of dilatation, and overload. Due to increased pressure, the wall of the interventricular septum bends to the left.
Respiratory functions are measured with special devices, and the spirogram is deciphered by a doctor in the functional diagnostics office.
The study of pressure in the pulmonary artery is carried out in complex diagnostic cases. A reliable sign of hypertension in the pulmonary circle is considered to be a resting pressure of 25 mm Hg. Art. and higher, and with load - over 35.
Research methods
- Spirometry is a test of pulmonary function that will show changes characteristic of COPD, and can also show impaired pulmonary function in CHF.
- Tests such as a chest x-ray, computed tomography (CT) scan, or magnetic resonance imaging (MRI) may show signs of CHF or COPD.
Often with CHF, the heart looks enlarged. When CHF worsens, fluid accumulates in or around the lungs, which can be seen on chest imaging.
Imaging tests may show changes in the lungs consistent with COPD, including thickening, inflammation, and bullae (air-filled spaces in the lungs that compress healthy tissue).
- Echocardiography (ultrasound of the heart) is an ultrasound examination of the structure, structure and mechanical activity of the heart. Using the echo, your doctor can examine the structure of your heart, the blood flow in your coronary (heart) arteries, and the pumping function of the heart muscle itself.
If cardiac function is reduced (often described as low ejection fraction), this may indicate CHF. An echo is not part of the diagnosis of COPD.
Functional classes
During the examination, it is necessary to establish the functional class of manifestations of cor pulmonale.
- Class 1 - the main symptoms are diseases of the bronchi and lungs, hypertension in the pulmonary circle is detected only with instrumental examination and stress tests;
- Class 2 - in addition to the listed symptoms, there is respiratory failure due to narrowing of the bronchi;
- Class 3 - respiratory failure is severe, followed by cardiac failure. Constant shortness of breath, tachycardia, dilatation of the neck veins, cyanosis. Studies reveal persistent hypertension in the pulmonary circulation;
- Class 4 - decompensation, all clinical manifestations are pronounced, there are congestion, respiratory and heart failure of the third degree.
Doppler examination allows you to quantify the pressure in the pulmonary artery, measure the reverse flow of blood (regurgitation) from the right ventricle into the atrium
Symptoms
Initially, the disease does not manifest symptoms. But patients often have pronounced manifestations of the underlying lung disease. This may be fatigue during physical activity, shortness of breath.
Gradually, as the pressure in the right ventricle increases, physical symptoms are manifested by systolic pulsation in the sternum, a loud pulmonary component of the second heart sound, murmurs of functional insufficiency of the 3-leaf valve and the pulmonary valve. A little later, the gallop rhythm of the right ventricle (third and fourth heart sounds), which intensifies with inspiration, hepatomegaly, swelling of the jugular veins (with a dominant wave a, in the event that there is no blood regurgitation due to tricuspid valve insufficiency), swelling of the legs are also noted.
Treatment
Treatment of chronic pulmonary heart disease should begin with the prevention of exacerbations of respiratory diseases, especially colds and flu, with the timely use of antiviral and antibacterial treatment.
Mode Changes
Patients are advised to limit physical activity. Do not visit mountainous areas, since in high altitude conditions even a healthy person experiences oxygen deficiency. And in patients with pulmonary diseases, a reflex vascular spasm occurs and the degree of tissue hypoxia deepens.
Women should be aware of the negative effects of birth control pills.
It is necessary to stop smoking and even staying in a smoky room.
Directions of therapy
All treatment methods are aimed at eliminating or weakening the existing mechanisms of pathology, these include:
- treatment of the underlying pulmonary disease and compensation of lost respiratory function;
- decreased vascular resistance in the pulmonary circulation and unloading of the right ventricle;
- restoration of normal blood composition, antithrombotic therapy.
Oxygen treatment
Oxygen is supplied in a humidified form through a mask, cannulas in the nasal passages, and some clinics use oxygen tents with special air saturation conditions. For a therapeutic effect on chronic pulmonary heart disease, the oxygen level in the inhaled air must be at least 60%.
Therapy is carried out for an hour up to 5 times a day and more often.
Oxygen supply can reduce all symptoms of the disease caused by hypoxia
How to lower pulmonary artery pressure
To reduce pressure in the pulmonary artery, medications of different groups are used:
- calcium antagonists (possible swelling and redness of the face, headache, feeling of heat, decreased blood pressure);
- α-adrenergic blockers - dilate blood vessels, reduce the ability of platelets to stick together (the side effects are the same, increased irritability and weakness are possible);
- inhaled nitric oxide (has no side effects);
- diuretics - medications with a diuretic effect unload the general bloodstream, facilitate the work of the heart (control of the potassium content in the blood is required);
- group of prostaglandins - selectively act on small blood vessels (side effects such as nasal congestion, increased cough, increased blood pressure, headache).
The drugs Heparin and Pentoxifylline are necessary to improve blood flow and antithrombotic action.
In case of severe heart failure, cardiac glycosides are prescribed very carefully.
Patients with symptoms of decompensation are treated in a hospital. Observation and clinical examination are carried out by a local therapist and pulmonologist.
Modern approaches to the treatment of cor pulmonale
Cor pulmonale (CP) is hypertrophy of the right ventricle that develops in diseases affecting the function or structure of the lungs, or both, except in cases where changes in the lungs are the result of a primary lesion of the left side of the heart or congenital heart defects.
Etiology
According to the WHO classification proposed in 1960, all diseases leading to the development of drugs are divided into three groups:
1. Diseases that primarily affect the passage of air in the lungs and alveoli.
This group includes 21 nosologies: chronic bronchitis, bronchial asthma, emphysema, tuberculosis, pneumoconiosis, bronchiectasis, sarcoidosis, eosinophilic granuloma, berylliosis, chronic diffuse interstitial fibrosis, systemic lupus erythematosus, etc.
2. Diseases that primarily affect chest movements:
kyphoscoliosis and other chest deformities, pleural fibrosis, chronic neuromuscular diseases (for example, poliomyelitis), alveolar hypoventilation, including idiopathic, as well as the condition after thoracoplasty.
3. Diseases that primarily affect the pulmonary vessels:
primary pulmonary hypertension (PPH), polyarteritis nodosa, other arteritis, thrombosis and embolism (including parasitic) of the pulmonary vessels, compression of the pulmonary artery trunk and pulmonary veins by mediastinal tumors, aneurysm, etc.
Pathogenesis
The main link in the pathogenesis of LS is a decrease in the total cross-section of the pulmonary vessels.
Moreover, in patients belonging to groups 1 and 2 of diseases according to the WHO classification, this occurs due to
spasm of small pulmonary arteries
in response to alveolar hypoxia.
This phenomenon was first described in 1946 by Von Euler and Liliestrand. In patients belonging to group 3, narrowing of the pulmonary arteries occurs not only due to vasospasm, which is not preceded by alveolar hypoxia, but also due to narrowing or blockage of their lumen as a result of thrombosis and embolism
, necrotizing arteritis (PLH, systemic vasculitis).
A decrease in the total cross-section of the pulmonary vessels leads to an increase in the total pulmonary vascular resistance and an increase in pressure in the pulmonary circulation.
Under these conditions, the right parts of the heart and, first of all, the right ventricle, experience pressure overload, and subsequently, with the development of tricuspid valve insufficiency, volume overload.
This leads to hypertrophy and dilatation of the right heart
.
As the disease progresses, compensation may fail— right ventricular failure
, which is the terminal stage of this condition.
Diagnostics
Diagnostics of drugs
, as a rule, does not present any difficulties and
consists in identifying hypertrophy and dilatation of the right heart in patients with the listed diseases.
The main methods to determine the enlargement of the right heart are electrocardiography, chest radiography, echocardiography (EchoCG).
Treatment
Treatment of patients with LS is complex.
It is aimed at reducing pressure in the pulmonary artery (PA), eliminating pulmonary and heart failure, which can be achieved by timely and adequate treatment of the disease leading to its occurrence.
Treatment of specific diseases complicated by the development of drugs is described in more detail in the corresponding monographs. This article will discuss approaches to the treatment of drugs themselves.
General recommendations
General recommendations for patients with drugs include adherence to a work and rest schedule
with the exception of excessive physical activity, especially in patients with signs of circulatory failure.
Colds and, above all, flu should be avoided,
which can lead to a significant deterioration in the clinical condition of patients with chronic bronchopulmonary diseases and PLH. Staying at high altitudes can also lead to a worsening of the condition, as it increases vasoconstriction in response to alveolar hypoxia that develops in the mountains. When choosing a method of contraception, women with PLH should keep in mind that birth control pills can cause pro-coagulative changes in the blood coagulation system and, as a result, lead to aggravation of the condition.
Calcium antagonists
This group of drugs is one of the main ones in the treatment of patients with pulmonary hypertension (PH) and drugs. The main purpose of prescribing vasodilators is to reduce pressure in the pulmonary circulation and prevent circulatory failure. First of all, drugs from the group of a-blockers (phentolamine, prazosin) were used in patients with drugs, then hydralazine, sodium nitroprusside, nitroglycerin. All of these drugs led to a significant decrease in pulmonary arterial pressure and total pulmonary vascular resistance, and an increase in cardiac output.
However, a number of reasons have limited the widespread use of these drugs in patients with LS.
First of all, this is the systemic arterial hypotension they cause, which does not allow prescribing high doses of drugs necessary to adequately reduce pressure in the pulmonary circulation. In addition, with long-term administration of some vasodilators (for example, sodium nitroprusside), tolerance develops, requiring a constant increase in their dose. This group of drugs is one of the main ones in the treatment of patients with pulmonary hypertension (PH) and drugs.
It is obvious that the “ideal” vasodilating drug for the treatment of PH should reduce the resistance of the vessels of the pulmonary circulation much more actively than the large one.
These requirements are best met by
calcium antagonists
from the dihydropyridine group.
The first representative of this class of drugs, nifedipine
, when compared with hydralazine and the phosphodiesterase inhibitor amrinone, most significantly reduced pressure in the PA without causing such a pronounced drop in systemic pressure (S. Rich et al., 1983).
This allowed the authors to suggest that nifedipine may cause selective dilatation of pulmonary vessels.
Later Prof.
V.Yu. Mareev et al. (1990) found similar results. In a comparative study of the effect of short-term administration of nifedipine, nitroglycerin, prostaglandin E1, captopril and prazosin on central hemodynamic parameters in patients with PLH, it was revealed that nefidipine significantly reduces pressure in the PA
, acting on the vessels of the pulmonary circulation to a greater extent than on the vessels of the systemic circulation. circle.
In further work (S. Rich, 1985) it was shown that the use of nifedipine is effective not only with short-term administration, but also with long-term therapy - up to 2 years or more.
Prescription of nifedipine in the maximum tolerated dose (up to 240 mg/day) led to a significant decrease in PA pressure in half of the patients with PLH, who are considered the least promising group in terms of treatment.
In 1992, data from a prospective observation of 64 patients with PLH for 5 years were published (S. Rich et al.): 23% of patients were on constant therapy with high doses of nifedipine throughout the entire period. At the same time, there was a significant improvement in their clinical status and survival (94% remained alive at the end of the observation period) in comparison with “non-responders” and those who responded to nifedipine therapy but were not treated (only 36% of patients from this group remained alive at the end of the observation period). end of the observation period).
The main mechanism of action of nifedipine is the relaxation of vascular smooth muscle due to a decrease in the intracellular movement of calcium ions during contraction.
Nifedipine is available in various forms. In addition to short-acting nifedipine, which is currently used extremely rarely - for carrying out acute tests, stopping hypertensive crises, its prolonged forms have been created, in which a gradual slow release of the drug occurs over 24 hours. This makes it possible to prevent or at least significantly reduce the severity of such adverse reactions as tachycardia, systemic hypotension, redness of the face, legs, swelling of the feet, which limits the use of the drug in adequate doses.
In addition to dihydropyridine calcium antagonists, which include nifedipine, benzothiazepines (diltiazem) can be used to treat patients with drugs. The advantages of the drugs include the absence of tachycardia when used, the disadvantages are a weaker vasodilator effect compared to dihydropyridines.
In recent years, new calcium antagonists – amlodipine and isradipine – have been introduced into clinical practice. The drugs have proven themselves to be highly effective drugs for the treatment of both systemic hypertension and PH.
It should be noted that the tactics of prescribing calcium antagonists in patients with LS are somewhat different from those in the treatment of other diseases
and consists in observing the basic four rules.
Rule one:
the dose of drugs should be “titrated”, starting with small dosages and gradually increasing them, bringing them to the maximum tolerated.
For nifedipine, initial doses are 20–40 mg/day; every 3–5 days the dose is increased by 20 mg/day.
Isradipine: initial dosage 2.5–5 mg/day, every 3–5 days the dose is increased by 2.5–5 mg/day.
Diltiazem: initial dose 30–60 mg/day, every 3–5 days the dose is increased by 30 mg/day.
Rule two:
select the dose of the drug taking into account the level of pressure in the PA: with systolic pressure in the pulmonary artery (SPAP), determined during catheterization of the right heart or echocardiography study, less than 50 mm Hg: nifedipine - 40-60 mg / day, isradipine - 7 .5–10 mg/day, diltiazem – 120–180 mg/day; with MPAP from 50 to 100 mm Hg: nifedipine – 80–120 mg/day, isradipine – 10–12.5 mg/day, diltiazem – 180–240 mg/day; with MPAP more than 100 mm Hg. Art.: nifedipine – 120–180 mg/day, isradipine – 12.5–15 mg/day, diltiazem – 240–360 mg/day.
Rule three:
take a differentiated approach to emerging side effects when prescribing calcium antagonists: while systemic hypotension and severe tachycardia can be considered serious adverse reactions requiring dose adjustment, side effects such as redness of the extremities, face, feeling of heat, swelling of the ankles should not cause panic from attending physicians.
Rule four: do not expect an immediate effect from calcium antagonists, since only in a quarter of cases can rapid improvement be observed, developing within a few days from the start of therapy; in other cases, noticeable clinical improvement is observed, as a rule, only after 3-4 weeks.
There are a number of reports on the effective administration of long-acting nitrates in patients with drugs. Most often these are patients with chronic obstructive pulmonary diseases and concomitant ischemic heart disease. The disadvantages of drugs, in addition to frequent headaches, include rapidly developing tolerance to them. Molsidomine does not have this undesirable effect.
, which can be successfully used in this group of patients. The dose of the drug for the treatment of patients with drugs is 8–16 mg/day.
Prostaglandins
Another group of drugs used in patients with drugs are prostaglandins.
The prerequisite for their introduction into clinical practice was research carried out in the 70s, which showed that prostaglandins play an important role in maintaining vascular tone both under normal conditions and in various forms of PH.
The first prostaglandin proposed for the treatment of PH was prostaglandin E1
, which is a short-acting vasodilating agent.
Reports of its use began to appear in the early 80s, and initially this drug was used primarily for conducting an “acute” test to determine the possibility of further therapy with vasodilators. Theoretically, prostaglandin E1 is an ideal drug for these purposes.
It has a short half-life of about 3 minutes, which allows you to quickly titrate the dose of the drug to the desired value and, if necessary, stop the test almost immediately. Unfortunately, a clear relationship between the “response” to the administration of prostaglandin E1 and the effect of therapy with other vasodilating drugs (for example, calcium channel blockers, hydralazine) was not identified. A number of patients who had a significant decrease in PA pressure in the acute test did not respond to long-term therapy with other vasodilators and, conversely, “non-responders” to the use of prostaglandin E1 “responded” to therapy with other vasodilating drugs. This allowed the study authors to conclude that the mechanism of action of prostaglandin E1 and other vasodilators is somewhat different.
Since the mid-80s, prostaglandin E1 has been used to treat patients with PH. A positive quality of the drug is that 70% of it is inactivated in the lungs and, when administered intravenously, the drug enters the systemic circulation in a negligible amount, without causing noticeable systemic hypotension. In addition, the drug has a pronounced antiplatelet effect, which makes it even more attractive for the treatment of patients with drugs and PH
, many of which are prone to thrombosis. At the same time, a significant disadvantage of prostaglandin E1 is the need for its constant intravenous administration to maintain vasodilation.
Therefore, for long-term infusion, a special portable pump is used, connected to a Hickman catheter, which is located in the jugular or subclavian vein. Complications with long-term administration of prostaglandin E1 are usually associated with disruption of the infusion system (for example, thrombosis or infection of the catheter), damage to the pump, or interruption of the infusion due to a variety of reasons. Doses of the drug
, used in patients with PH, range from 5 ng/kg/min to 100 ng/kg/min.
The Russian Cardiology Research and Production Complex uses the following drug dosage regimen: the initial dose is 5–10 ng/kg/min, then gradually increases to 30 ng/kg/min
. With this prescription, maximum pulmonary vasodilation can be achieved with a minimum number of adverse reactions, which include systemic hypotension, cardiac pain of an unspecified nature, headaches and abdominal pain, redness of the face and extremities, nausea.
It should be noted that prostaglandin E1 is prescribed to patients with PH, as a rule, only as monotherapy.
At the same time, its
combination with other vasodilators
, in particular calcium antagonists, may be justified, given the difference in the mechanisms of their vasodilating effect.
We have proposed a regimen of course use of prostaglandin E1
, administered in a daily dose of 60 mcg against the background of constant use of calcium antagonists. When this combination was used for 21 days, more than half of the patients experienced an improvement in clinical status. At the same time, adverse reactions (in particular, systemic hypotension) were mild and did not lead to drug discontinuation.
Recently, another drug from the group of prostaglandins has been used - prostacyclin.
.
Recommended doses are 2–24 ng/kg/min. It is a slightly more active vasodilator than prostaglandin E1, having almost the same advantages and disadvantages as the latter. But the exorbitant cost of prostacyclin does not allow its widespread use. In general, prostaglandins are currently used in patients with drugs who are intolerant to calcium antagonists or when they are ineffective.
Some authors call prostaglandin therapy a “bridge” to transplantation. There are cases where the constant administration of prostaglandins lasted up to 5 years, although on average the maximum period of their continuous use does not exceed several months.
Nitric oxide (II)
Recently, nitric oxide (II) (NO) has been introduced into clinical practice for the treatment of PH. Its vasodilating effect is based on the activation of guanylate cyclase in the smooth muscle cells of the pulmonary vessels, which leads to an increase in the level of cyclo-GMP and a decrease in intracellular calcium levels.
NO is used in the form of inhalations. With this method of administration, this substance quickly combines with hemoglobin, which prevents NO from entering the systemic circulation and the development of arterial hypotension. Therefore, NO can be considered a selective vasodilator, acting exclusively on the vessels of the pulmonary circulation.
NO is the gold standard for acute testing to identify responders and nonresponders to vasodilator therapy.
It compares favorably with prostaglandins in its shorter period of action, ease of administration (inhalation through a face mask or nasal catheter), almost complete absence of side effects, and low cost. To carry out an acute test, inhalation of NO in increasing concentrations is used. As a rule, the maximum drop in pressure in the LA is observed after the initial dose is applied after 2 minutes.
Long-term administration of NO is also being introduced into clinical practice.
. For this purpose, special portable inhalation systems have been created. Treatment is carried out over several weeks, but there are reports of longer-term administration of the drug - up to 1-2 years.
It should be noted that only 25–50% of patients with PH “respond” to vasodilator therapy, that is, they can achieve a decrease in PA pressure and an increase in cardiac output without significant systemic hypotension.
There are the following criteria for “response” to vasodilating therapy during acute tests:
:
• more than 20% reduction in pulmonary vascular resistance;
• more than 20% decrease in pulmonary vascular resistance, accompanied by a drop in the ratio of pulmonary vascular resistance to total vascular resistance;
• increased cardiac output (>10%) together with a decrease in mean pulmonary artery pressure;
• more than 30% reduction in pulmonary vascular resistance combined with more than 10% reduction in pulmonary artery pressure.
Of course, conducting an acute test has some limitations, which were already mentioned earlier, but nevertheless, with its help it is possible to predict quite accurately whether it would be advisable to prescribe vasodilators in a particular patient.
It is currently impossible to say definitively what causes the “non-response” to vasodilating therapy in patients with LS. The most reasonable are two points of view.
According to the first, refractoriness to vasodilators occurs in cases where irreversible changes in small pulmonary vessels predominate, such as intimal fibrosis, plexogenic and dilated lesions.
The second point of view, confirmed by our research data, is that “non-response” to vasodilating therapy can occur in patients with severe disturbances in the hemostatic system, when procoagulative changes come to the fore, and vasospasm does not play a leading role.
Most often these are patients with pulmonary artery thrombosis and PPH. In such patients, it seems advisable to add anticoagulants to the basic therapy with vasodilators. Literature
1. Belenkov Yu.N., Chazova I.E., Samko A.N. and others. The use of the calcium antagonist isradipine in patients with primary pulmonary hypertension // Cardiology. – 1995; (7): 9–13.
1. Belenkov Yu.N., Chazova I.E., Samko A.N. and others. The use of the calcium antagonist isradipine in patients with primary pulmonary hypertension // Cardiology. – 1995; (7): 9–13.
2. Mukharlyamov N.M. Pulmonary heart. – M. Medicine, 1973; 264.
3. Chazova I.E., Zhdanov V.S., Veselova S.P., Mareev V.Yu. Pathology of primary pulmonary hypertension // Arch. pathology. 1993; (3): 77–80.
4. Chazova I.E., Mareev V.Yu. Primary pulmonary hypertension: questions that require answers // Ter. archive. 1994; (3): 77–80.
5. Bardsley P., Evely R., Howard P. Hypoxic cor pulmonale. A review // Herz. 1986; (11): 155–68.
6. Pulmonary circulation / Ed. A. Fishman. – USA. Philidelphia: Univ. Pennsylvania press, 1990; 551.
7. Pulmonary hypertension / Eds. E. K. Weir, J. T. Reeves. – USA, NY, Futura, 1984; 442.
8. Rubin L. Primary pulmonary hypertension // Chest. 1993; (104): 236–50.
9. Vender R. Chronic hypoxic pulmonary hypertension. Cell biology to pathophysiology // Chest. 1994; (106): 236–43.
Nifedipine –
Corinfar (trade name)
(ASTA Medica)
| Applications to the article |
| Rules for prescribing calcium antagonists in patients with cor pulmonale: • drugs should be prescribed from a small dose, gradually increasing it, bringing it to the maximum tolerated; • select the dose of drugs taking into account the level of pressure in the pulmonary artery; • differentiated approach to emerging side effects; • immediate effects should not be expected from calcium antagonists. |
| The main purpose of prescribing vasodilators for cor pulmonale is to reduce pressure in the pulmonary circulation |
| Drugs of choice for the treatment of cor pulmonale: • calcium antagonists; • prostaglandins; • nitric oxide (II) (NO) in the form of inhalations. |
Forecast
The mortality rate of patients from chronic pulmonary heart disease remains high: 45% of patients survive in the decompensation stage for about two years. Even with intensive therapy, their life expectancy is no more than four years. Lung transplantation gives 60% of patients survival over the next two years.
The disease is very difficult to treat. Any person has the opportunity to rid himself of bad habits and take care of his health in a timely manner. The appearance of cough, shortness of breath and other symptoms requires immediate medical attention.



![Table 2. Hemodynamic definition of PH (adapted from [2] with modifications)](https://ms-pi.ru/wp-content/uploads/tablica-2-gemodinamicheskoe-opredelenie-lg-adaptirovano-iz-2-s-izmeneniyami-330x140.jpg)