Date of article writing: 03/30/2020 Quantity
()
Causes of degeneration Types of pathology Symptoms of the disease Diagnosis Treatment methods Laser treatment of retinal dystrophy with MAKDEL devices Efficacy and results of treatment Contraindications Recommendations from ophthalmologists To avoid retinal degeneration, it is recommended
Hardware treatment of dystrophic diseases of the posterior segment of the eye should be carried out strictly according to the doctor’s recommendation and is always an addition to the main treatment (for example, anti-VEGF therapy). It is not recommended to conduct laser conservative treatment sessions without a preliminary examination by an ophthalmologist.
Retinal dystrophy is a whole group of irreversible diseases in which organic changes occur in the tissues or structures of the eyeball.
Causes of degeneration
Various factors can provoke the development of dystrophy:
- hereditary predisposition;
- age-related changes;
- myopia;
- inflammatory eye diseases;
- pathologies of the vascular system of the eyes;
- viral infections;
- injuries;
- ophthalmological operations;
- vitamin deficiency (especially vitamin A deficiency);
- smoking;
- alcohol abuse;
- intoxication of the body;
- chronic stress.
Degenerative retinal lesions are diagnosed in 40% of cases in nearsighted people, and in 8% in farsighted people. In people with normal vision, such problems are quite rare (in 2-3% of cases).
The risk group includes people suffering from diabetes, obesity, hypertension, atherosclerosis, and heart disease.
Macular degeneration of the retina - “dry form”
Age-related macular degeneration (AMD) or involutional central dystrophy, senile macular degeneration. This is the name of a degenerative disease of our retina, which leads to decreased central vision.
The main cause of the disease is the irreversible aging process of the entire human body, including its eye organs. Also, retinal dystrophy can be a consequence of trauma, previous inflammatory or infectious diseases, developed myopia, and sometimes this is due to the negative influence of heredity.
Smoking, diseases of the cardiovascular system, and radiation can provoke the development of the disease.
Types of pathology
Dystrophy can be congenital or acquired . The congenital form is not completely curable and constantly progresses, significantly worsening visual acuity. To slow down degeneration, it is necessary to strictly follow medical recommendations.
Acquired dystrophy is divided into:
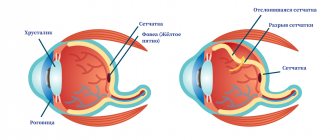
- Central, or macular (macular degeneration) - affects the central part of the retina (macula), which is responsible for image accuracy and the ability to distinguish small details. As a result, central vision is impaired, but peripheral vision is not changed. In this case, problems arise when reading, writing, drawing, and driving a car.
- Peripheral - develops on the periphery of the retina. Does not affect visual acuity, but can lead to retinal rupture and detachment.
Symptoms and causes of muscular dystrophy
The causes of muscular dystrophy lie in a chromosomal mutation. The X chromosome is affected, but each form of the disease has its own characteristics and is characterized by a unique set of mutated genes. Moreover, they all contribute to a decrease or complete cessation of the synthesis of dystrophin, a protein necessary for muscles to function normally.
It is this protein that is responsible for their growth and recovery, although its content is very small - only 0.002% of the total amount of proteins in muscles. The lower the amount of dystrophin, the more the disease progresses and the severity of the symptoms.
Among the main symptoms accompanying all forms of pathology, it is worth noting the following signs:
- muscle weakness that progresses over the years;
- falls, clumsiness, changes in gait (a person begins to waddle and cannot control his gait);
- problems with speech, breathing, swallowing, chewing food, coordination of movements;
- muscle pain – the lower leg especially suffers;
- difficulties with memory, concentration, learning;
- cramps and contractures.
If you find yourself with the symptoms listed above, make an appointment with a neurologist at a medical clinic.
Make an appointment The application is preliminary. An operator will contact you to confirm your appointment.
Your application has been accepted, our specialists will contact you shortly. Thank you for contacting the medical
Symptoms of the disease
Clinical manifestations may vary depending on the type of pathology.
But there are also common signs:
- blurred or distorted image, curved lines;
- deterioration or loss of color perception;
- difficulty reading and working with small objects;
- inability to distinguish between a moving and a stationary object;
- disorientation at dusk;
- the appearance of dark spots or bright flashes before the eyes;
- letters falling out when reading.
In severe cases, complete loss of vision is possible.
How do you know if you have retinal degeneration?
One of the dangerous features of retinal dystrophy is the complete absence of symptoms in the early stages. As it progresses, you may notice:
- general decrease in vision;
- decreased vision in low light, at dusk;
- the appearance of black dots, “floaters” before the eyes;
- curvature of the contours of objects;
- clouding, blurriness of the image, which may be episodic;
- deterioration in perception, identification of colors and their shades;
- the appearance of flashes of light, “lightning” before the eyes.
It is best to have regular eye examinations at a professional clinic, such as our medical one. In this case, degenerative processes of the retina can be detected in the early stages and their development can be successfully stopped or slowed down.
Diagnostics
To diagnose degenerative changes, the ophthalmologist conducts a comprehensive examination:
- visometry - checking visual acuity using a table;
- perimetry - study of the visual field;
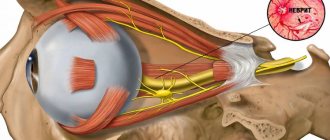
- ophthalmoscopy – examination of the fundus of the eye;
- Ultrasound of the eyeball;
- fluorescein angiography of blood vessels;
- electrophysiological study - determining the performance of the optic nerve and retinal nerve cells;
- coherent optical tomography – shows the smallest changes in tissues;
- lab tests.
What are PCRD and PVKHRD?
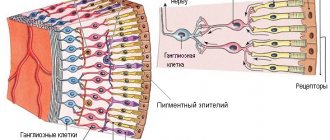
PCRD – peripheral chorioretinal dystrophy
This type of dystrophy directly affects the retina of the eye and its choroid (choroid). PCRD is considered a favorable type of dystrophy, since it does not carry any risks for the formation of a severe complication - retinal detachment. The most striking representative of the PCRD family is cobblestone dystrophy, which is harmless single or multiple foci of chorioretinal atrophy scattered along the periphery of the retina.
PVCRD – peripheral vitreochorioretinal dystrophy
In comparison with PCRD, PCRD is considered an unfavorable type of dystrophy, since in the pathological process, in addition to the retina and choroid, the vitreous body (lat. corpus vitreum), which is tightly fused to the area of chorioretinal dystrophy, is involved. It is believed that under conditions such as heavy lifting, sudden shaking of the body or head, childbirth, the vitreous body can provoke retinal rupture, thereby increasing the risk of retinal detachment. But, fortunately, in reality everything is not as scary as they used to think. Most PCVDs are harmless and simply require dynamic monitoring. There are types of PVCRD, the danger of which in most cases is greatly exaggerated. These include 2 types of dystrophies: lattice dystrophy (or “lattice”) and “snail track”. It is these two types of dystrophy that ophthalmologists constantly argue about.
"lattice" dystrophy
“snail track” dystrophy
Treatment methods
For retinal dystrophy, treatment is possible using conservative methods:
- eye drops;
- intraocular administration of drugs;
- oral medication (angioprotectors, vasoconstrictors, glucocorticosteroids, diuretics);
- hardware effects (photostimulation, laser stimulation, magnetic stimulation, electrical stimulation, electrophoresis, phonophoresis, photodynamic, microwave and ultrasound therapy).
The ophthalmologist selects the optimal method of therapy individually for each patient, taking into account the cause and prevalence of degenerative processes, the severity and rate of progression of the disease. But in most cases, laser treatment of retinal dystrophy is the most effective, which is widely used in their practice by specialists from leading ophthalmological clinics.
In severe cases, surgery may be required:
- laser coagulation - cauterize damaged areas to other parts of the eye, which helps prevent retinal detachment;
- revascularization – increase the lumen of blood vessels:
- vasoreconstruction – restore blood vessels using grafts;
- vitrectomy – the vitreous body is removed and replaced with a special material.
Diabetic retinopathy of the eye
Eye complications are common in diabetes and can lead to partial or complete loss of vision. However, much can be done to avoid such a sad outcome. Cataracts, for example, occur twice as often in diabetics as in healthy people, but can be successfully treated with surgery. The most severe eye complication of diabetes is diabetic retinopathy. This is a progressively developing damage to the retina, the thinnest light-sensitive inner layer of the eye, which perceives objects and objects around us like photographic film in a camera. Timely and adequate treatment of diabetic retinopathy using laser coagulation can significantly reduce or prevent the risk of blindness. But diabetic retinopathy, as it develops, may not manifest itself as decreased vision for a long time, and when it is detected, treatment is often delayed or becomes impossible. In other words, if you have diabetes, you can have vision-threatening retinopathy and not realize it for a long time.
The only way to reduce the risk of vision loss due to diabetes is regular examination by an ophthalmologist who has the facilities and capabilities to study the condition of your retina in detail. People suffering from type I diabetes mellitus, i.e. Those who use insulin are at risk of losing vision several times more than those with type II diabetes. The earlier diabetes occurs, the more severe the retinopathy, and over the years the risk of vision loss is higher. The first signs of diabetic retinopathy, even with successful control and treatment of the disease, appear several years after the actual onset of diabetes.
For a patient with diabetes, two annual examinations by an ophthalmologist are sufficient, although in some cases, such as pregnancy or a long course of the disease, they are required more often.
Diabetic rhinotherapy - diagnosis.
An examination to assess the risk of diabetic blindness should include: testing visual acuity, dilating the pupil with eye drops and a detailed examination of the fundus using a biomicroscope. The role of optical coherence tomography in the early detection of signs of diabetic retinopathy, in particular diabetic macular edema, is also invaluable.
Our Center has all the necessary conditions for timely detection of diabetic eye disease and its effective treatment. Ophthalmologists strongly recommend contacting the Center for examination and consultation if you know that you have diabetes.
Laser treatment of retinal dystrophy using MAKDEL devices
For retinal dystrophy, laser treatment is often carried out using the MAKDEL-08 device. During operation, the device projects a high-quality speckle structure (the eye perceives it as a picture of chaotically moving dots) onto the retina, which helps improve the general condition of the visual system.
MACDEL-08 “Speckle”
More details
Unlike similar devices, MAKDEL-08 produces a narrow spectral band, which ensures speckle stability. In addition, the laser radiation is higher, which can significantly reduce the exposure time.
Treatment is carried out in courses of 10-12 procedures lasting 3-5 minutes. It is recommended to repeat therapy 2-3 times a year.
Forms of muscular dystrophy
Muscular dystrophy is characterized by progressive symmetrical muscle atrophy. The disease in all its forms and manifestations takes a long time. Muscle weakness in this case is due to the lack of an important protein - dystrophin. It is important for humans as it connects the muscle fiber skeleton with the extracellular matrix.
The absence of dystrophin causes constant fatigue, gait disturbances, problems with swallowing and coordination of movements. In total, there are more than 30 forms of the disease. They differ in character, severity, and symptoms.
9 most common ones:
- Duchenne muscular dystrophy. This is the most common form of pathology among children. Mostly only boys suffer from it. In addition to problems with coordination of movements and walking, patients often fall, walk on tiptoes or wobble, and suffer from mental retardation. Usually detected at the age of 2-3 years. The muscles gradually change in size, become weaker, and cannot perform their functions. In most cases, by the age of 12-13 years the patient requires a wheelchair. The life expectancy of such people usually does not exceed 20 years.
- Becker muscular dystrophy. The symptoms in this case are approximately the same as in the previous form. But here the symptoms are more mild, and the progression of the pathology is slowed down. This form of dystrophy is diagnosed in childhood and adolescence and affects only men. The average life expectancy of such patients is only 10 years longer than with Duchenne disease.
- Myotonic disorders. This is the most common form of the disease among adults and is diagnosed in childhood or adolescence. Such disorders affect not only the muscles of the arms and legs, they negatively affect the heart, nervous and hormonal systems, vision, and gastrointestinal tract. The disease often progresses slowly.
- Humoscapulofacial myopathy. The pathology affects the muscles of the face, shoulder blades, arms and legs. The diagnosis is usually made in childhood and occurs in both boys and girls. The disease develops slowly, but is characterized by a sharp deterioration and periods when the person’s condition improves. Typically, most patients with this diagnosis are able to work and move independently, although they have problems with walking, chewing and swallowing.
- Erb-Roth muscular dystrophy affects both boys and girls. It is usually diagnosed in childhood. Most patients live to be 40 years or more. Symptoms first develop in the thighs and then spread to the arms and legs.
- Congenital pathology. This muscle dystrophy is diagnosed in newborn age. It occurs in both girls and boys. This form of the disease exists in two variants: myosin deficiency dystrophy and Fukuyama disease. Both of them are severe and have pronounced symptoms. The child remains disabled forever, suffering from seizures and pathological changes in the brain.
- Distal dystrophy. This form is a rare disease that manifests itself in adulthood. The progression of the pathology is slow, which gives people a chance to lead a normal lifestyle and live to old age. The muscles of the limbs suffer the most from it.
- Dystrophy of the muscles of the eyeball and pharynx. Usually diagnosed at the age of 40-50 years. Causes problems with swallowing and chewing food, weakness of the eye muscles and related symptoms. In the later stages it causes suffocation and spasms, and relapses of pneumonia.
- Emery-Dreyfus muscular dystrophy. The disease is quite rare, but different from other forms. It appears in adolescence among boys. It affects the limbs and causes pathological changes in the heart even in girls who are only carriers of the gene and do not suffer from severe symptoms. Usually such patients can live to adulthood.
It is noteworthy that this is a hereditary disease that can appear at any age. Most often, the first symptoms are detected during preventive examinations by specialists in early childhood. According to statistics, boys suffer from the pathology more often than girls.
The prognosis for such patients depends on many factors. Someone lives with the disease for years, only maintaining their condition and slowing down the progression of muscle atrophy. Others quickly lose the ability to lead a normal lifestyle, cannot walk independently and often need a wheelchair.
Recommendations from ophthalmologists
After completing the course of therapy you must:
- use sunglasses when outdoors;
- When reading, writing, working at the computer, use high-quality lighting and take regular breaks;
- perform special exercises;
- enrich your diet with foods that are good for your eyesight;
- take vitamin and mineral complexes;
- avoid excessive physical activity;
- give up bad habits (smoking, alcoholic drinks).
Symptoms
Each form of muscular dystrophy has its own specific clinical picture, but there are also a number of common symptoms characteristic of this group of diseases:
- gradual decrease in muscle fiber tone;
- absence of pain syndrome;
- maintaining sensitivity of the affected areas;
- change in gait;
- frequent falls due to weakness of the leg muscles;
- change in muscle size;
- constant fatigue;
- gradual atrophy of skeletal muscles;
- loss of acquired physical skills in children.