The main manifestation of a postoperative hernia is the appearance of a tumor-like protrusion along the line of the postoperative scar and on its sides.
With sudden movements and physical stress, the hernia increases and painful sensations appear. In the lying position, the hernia decreases or disappears.
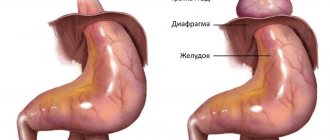
As the name implies, a postoperative hernia, or ventral hernia, develops as a consequence of surgery on the abdominal organs.
The appearance of postoperative hernias is associated with thinning of the muscles and connective tissue in the area of the postoperative scar, due to which the internal organs (intestines, greater omentum) protrude through the defects of the surgical scar beyond the abdominal wall under the skin.
The cause of the appearance of a postoperative hernia may be technical errors when applying a suture, non-compliance with recommendations for postoperative rehabilitation, as well as the individual characteristics of the patient (weakness of connective tissue, obesity, diabetes, etc.)
Why surgery is needed
The only reliable way to get rid of the pathology is an operation with the installation of a mesh prosthesis - tension-free hernioplasty. All other methods of treatment (medicines, exercise therapy, traditional methods) are powerless. Such a hernia occurs due to insufficient conditions for the formation of a postoperative scar:
- Insufficient preoperative preparation (for emergency interventions).
- Defect in surgical technique (poor quality suture material, excessive tissue tension, broken suture, etc.).
- Long-term drainage or packing of the abdominal cavity.
- Violation of the postoperative regime (physical stress, diet violations, refusal to wear a bandage, etc.).
- Connective tissue pathologies.
- Diseases accompanied by tension in the abdominal wall (intestinal diseases, pneumonia, bronchitis, etc.).
Scar tissue defects can only be eliminated through surgery. Therefore, you should not delay your visit to the doctor; even the smallest hernia is dangerous due to strangulation and the development of life-threatening conditions, including blood poisoning.
How does a hernia of the anterior abdominal wall manifest?
First of all, this is a cosmetic defect, that is, a noticeable visual protrusion. The “weakest” places of the anterior abdominal wall are the umbilical ring, inguinal canal, Spigelian line, and linea alba. The hernia consists of several parts:
- hernial orifice;
- hernial sac;
- contents of the bag;
- outer soft tissue shells of the bag.
A hernia causes pain and discomfort, and some patients feel as if something has come out or experience a sensation of tearing. Other symptoms:
- feeling of pressure on the anterior abdominal wall;
- pain and burning;
- feeling of weakness;
- the bulge may appear when coughing, sneezing, straining and disappear when lying down;
- When straining, coughing, or lifting heavy objects, the pain intensifies.
Cost of treatment of postoperative hernias
The prices indicated in the price list may differ from the actual prices. Please check the current cost by calling +7 495 104 8605 (24 hours a day) or at the GMS Hospital clinic at the address: Moscow, st. Kalanchevskaya, 45.
| Name | Price |
| Hernia repair of postoperative ventral giant hernia | RUB 300,006 |
| Hernia repair of postoperative ventral hernia | RUB 180,005 |
Dear Clients! Each case is individual and the final cost of your treatment can only be found out after an in-person visit to a GMS Hospital doctor. Prices for the most popular services are indicated with a 30% discount, which is valid when paying in cash or by credit card. You can be served under a VHI policy, pay separately for each visit, sign an agreement for an annual medical program, or make a deposit and receive services at a discount. On weekends and holidays, the clinic reserves the right to charge additional payments according to the current price list. Services are provided on the basis of a concluded contract.
Plastic cards MasterCard, VISA, Maestro, MIR are accepted for payment. Contactless payment with Apple Pay, Google Pay and Android Pay cards is also available.
Western standards of treatment (evidence-based medicine)
Continuous staff development
Regular interaction with leading Russian and foreign medical institutions
Modern medical equipment and advanced diagnostic and treatment methods
Unified standard of service
We work around the clock 24/7/365
Make an appointment We will be happy to answer any questions Coordinator Oksana
Advantages of tension-free hernioplasty
In the hernia treatment center GMS Hospital, the non-tension hernioplasty method is used for the treatment of postoperative hernias, which has the following advantages:
- The use of meshes made of inert polymeric materials eliminates the lack of tension of the own tissues.
- No inflammatory or allergic reactions.
- The surrounding tissues and fascia are not injured.
- At the site of the sewn-in endoprosthesis, blood circulation is not impaired.
- No pain or discomfort when moving.
- Minimal postoperative period.
- Full recovery takes 3-6 weeks.
The operation does not require complex or lengthy preparation and can be performed under any anesthesia, which is especially important if the patient is contraindicated for general anesthesia.
Hernioplasty of large hernias
In patients with long-standing large incisional hernias, the volume of the abdominal cavity may decrease over time. The relapse rate in these patients reaches 53%.
In the surgical treatment of this category of patients (those with large ventral and postoperative hernias), it is not possible to achieve good results using standard surgery.
For abdominal wall plastic surgery in this category of patients, anterior or posterior components separation technique (ACST and posterior components separation technique – PCST) is used, both open and endoscopic. Separation of the components of the abdominal wall allows you to increase the volume of the abdominal cavity and avoid the development of serious complications in the postoperative period.
Basic techniques for separating abdominal wall components
Patients requiring the use of these techniques should be operated on in specialized departments.
Anterior technique – OM Ramirez operation (I, II)
Ramirez I
Ramirez II
Posterior technique – Novitsky operation
Types of postoperative hernias
An incisional hernia can appear after either emergency or elective surgery. Depending on their size, they are divided into small (up to 4 cm), medium (5-15 cm), large (25-36 cm) and giant (more than 40 cm in diameter). Based on location, the following types of ventral hernias are distinguished:
- Medial - located in the center of the body.
- Lateral – lateral hernias.
- Single and multi-chamber.
- Reducible and irreducible.
Depending on the listed criteria, a hernia repair technique is selected.
Signs and symptoms
The main sign of a hernia is protrusion along the line of the postoperative scar or on its sides. At the initial stage, such protrusions are reducible and are not accompanied by painful sensations. The following symptoms are added:
- Pain in the scar with any exertion (walking, coughing, sneezing, sudden movements, lifting weights).
- Dyspeptic disorders - flatulence, constipation, nausea, vomiting.
The occurrence of any of the listed signs is a serious reason to see a doctor. Postoperative hernias are often complicated by pinching, coprostasis, and intestinal obstruction. The sooner the pathology is eliminated, the faster you will return to your normal rhythm of life.
Preparation, recovery period and possible contraindications
The preparation plan includes not only an analysis of the patient’s complaints and the clinical picture of the disease, but also clarification of concomitant ailments and determination of the state of general health. The attending physician will tell you in detail about the specific actions preceding surgery.
After surgical removal of a postoperative abdominal hernia without strangulation, the recovery period is minimal and amounts to 3–5 days. In this case, it is not necessary to be in a hospital; it is only important to follow the doctor’s instructions at home.
Contraindications to laser endoscopy for postoperative abdominal hernia are:
- previous diseases of the abdominal organs;
- oncology;
- pregnancy and lactation;
- acute infectious diseases;
- severe pathologies of the cardiovascular system;
- serious disorders of psycho-emotional health.
Diagnostics
Diagnostic measures include surgical examination with palpation and a number of laboratory and instrumental studies:
- Abdominal ultrasound
- Irrigoscopy
- Survey X-ray
- Herniography
- Blood and urine tests
To clarify some parameters, it may be necessary to prescribe MSCT or MRI of the abdominal cavity, colonoscopy and other examination methods.
You have questions? We will be happy to answer any questions Coordinator Tatyana
Treatment methods
To eliminate the protrusion, a herniotomy operation is performed. In our Center we operate on postoperative hernias of any complexity. Depending on the characteristics of the disease and the general condition of the patient, the operation is performed using one of the following methods:
- Laparoscopic tension-free hernioplasty is an intervention using endoscopic technologies, in which excision of the hernia and implantation of a mesh endoprosthesis is carried out through several small punctures.
- Open tension-free hernioplasty - hernia repair and suturing of a mesh implant is performed using open access through a small incision.
The Hernia Treatment Center at GMS Hospital employs surgeons with many years of experience in successful hernia repair operations. The use of materials from leading manufacturers allows us to efficiently eliminate both small and large complicated hernias with high results and without the risk of relapse of the disease.
Postoperative ventral hernia - symptoms and treatment
For the surgical treatment of PIH, a huge number of different methods have been proposed, differing mainly in the technique of closing and strengthening the hernial orifice (hernioplasty).[24] All methods of PIH hernioplasty can be divided into two groups: plastic using local tissues and plastic using additional plastic materials. A combination of these methods is also possible.
Hernioplasty with local tissues
There are several methods of hernioplasty using local tissues:
- aponeurotic methods of hernioplasty;
- muscular-aponeurotic methods of hernioplasty;
- muscular methods of hernioplasty;
- plastic surgery using a hernial sac.
Despite the high risk of relapse, plastic surgery with local tissues takes place in surgical practice. Most often, these methods are used in children and young women.
Plastic surgery of the hernial orifice using additional plastic materials
Plastic surgery using preserved dura mater
Among homoplastic techniques, the most relevant was the use of the dura mater, and many surgeons, especially in Russia, used preserved dura mater for plastic surgery, especially for large and giant PIH.[2] Dura plastic surgery was widely used in the clinic of K. D. Toskina, where this plastic surgery has been used since 1972. Good results can be noted, for example, in 252 operations it has only 1.8% relapses and 5.6% wound complications. In modern herniology, this technique is not used, since the problems associated with the preparation and storage of implants have been joined by the problem of HIV infection and hepatitis.
Plastic surgery using autoderma
Due to the ease of implementation and less trauma (compared to the use of autofascia), only autodermal plastic surgery remains relevant among autoplastic techniques. These methods and alloplasty with the use of artificial prostheses form the basis of modern plastic surgery using additional plastic materials. The first experience of using skin for hernioplasty belongs to G. Simon in 1881. The skin was cut around the hernial protrusion, the inner edges were stitched together, and the hernial sac with a sutured skin flap was immersed by suturing the outer edges of the skin incision. This technique was accompanied by a large number of relapses and specific complications, such as the formation of dermoid cysts. With autodermal plastic surgery, an important point is the fixation of the skin flap with some tension, as well as early activation of patients. This degeneration of the skin flap was actively used by supporters of autodermal plastic surgery to widely promote this method. One of the main problems remains the problem of complications of the wound area and graft engraftment. Another obstacle was that the skin flap degenerates not into dense aponeurotic tissue, but into scar-like loose connective tissue, which has much less resistance to physical stress. The use of autodermal plastic surgery in the treatment of large hernias with intestinal and/or ligature fistulas is generally inappropriate.[12]
Use of synthetic material
Since the 40s of the 20th century, a new stage in herniology began, associated with the synthesis of high-molecular polymers suitable for implantation into the tissues of the human body. The development, implementation and use of modern polymer materials have significantly expanded the possibilities of prosthetic hernioplasty of PIH of almost any size.[10] Currently, prosthetic hernioplasty is the basic treatment method for patients with PIH. However, with prosthetic hernioplasty, the question arises about specific complications - seromas, due to prolonged exudation of the reactive fluid in the area of the prosthesis.[18] The incidence of complications may depend on many factors, ranging from the prosthesis used to the method of its implantation. Today, in addition to the surgeon’s technique, it is necessary to take into account the characteristics of synthetic polymer materials to increase the efficiency of prosthetic methods, since complications associated with low quality prostheses can ruin even the most advanced surgical technique. The use of materials such as nylon, foam rubber, polyvinyl alcohol, fluoroplastic and many others has increased the frequency of infiltrates, seromas and suppurations, long-term non-healing fistulas, and sequestration of grafts.[14] Some authors have written about the carcinogenicity of plastics when they remain in the body for a long time.[3][17][24] Considering all of the above, the synthetic material for hernioplasty must be chemically inert, durable, elastic, convenient for sterilization and affordable; the prosthesis must not have carcinogenic or pro-inflammatory properties.
With the development of laparoscopic herniology, an additional requirement has recently emerged - the ability to form a barrier to the development of adhesions from the abdominal cavity. JP Amid (1997) identifies four types of synthetic materials:
Type No. 1 - total microporous endoprosthesis (atrium, Marlex, Prolene, Trelex). The micropore diameter of this type is more than 75 microns. Macrophages, fibroblasts, capillaries, and collagen fibers freely penetrate through these pores.
Type No. 2 - total microporous prosthesis (Gore-Tex; surgical membrane and double network) with a micropore size of less than 10 microns.
Type No. 3 - macroporous endoprosthesis with a multifilament component (Teflon, Mersilene, Dacron, woven polypropylene network).
Type No. 4 - materials with submicroscopic pores. Type 4 materials are practically unsuitable for plastic surgery, but in some cases they are used in combination with type 1 prostheses for intra-abdominal implantation. In cases of infection of the material when the porosity of its fibers is less than 10 microns, the dentures have to be completely removed, since leaving it leads to the formation of a chronic focus of infection. The properties described above are found in braided and twisted threads, as a result of which a good prosthetic material should consist of monofilament threads. The main material that meets the requirement is polypropylene, the study of which showed no signs of rejection, carcinogenicity or resorption over time. On its basis, monofilament polypropylene mesh Marlex, bifilament polypropylene mesh Prolene, multifilament polypropylene mesh Surgipro, which are still used today, were created. Also, the pore diameter of the material determines the speed and quality of its implantation into the body tissue. It has been proven that with a pore size of more than 75 microns, the implant grows throughout its entire thickness with collagen fibers and fibrocytes within a month, while with smaller pores, histiocytic infiltration prevails and, as a result, weaker fixation of the synthetic material in the body tissues.
The use of Marlex and Prolene prostheses, whose pore sizes are 100 microns, has reduced the incidence of wound infectious complications compared to lavsan (mersilene) from 15% to 5%, and the formation of fistulas from 15% to 2%. It has been experimentally proven that the optimal pore size is 2-3 mm.[22] Prostheses made of polytetrafluoroethylene (Gore-Tex) are quite inert, comparable to polypropylene, but their adhesive properties are lower, which means they are less firmly implanted into the body tissue. In addition, their use is often complicated by chronic tissue infection. JJ Bauer et al. (2002) reports the use of Gore-Tex during operations for extensive hernias, the result was wound suppuration in 7.1% and recurrence of the hernia in 10.7% of patients; in one patient the prosthesis had to be removed. Therefore, Gore-Tex is used exclusively for laparoscopic hernia repairs, in which the likelihood of infection of the prosthesis is minimized due to the tense carboxyperitoneum.[10]
A more delicate connective tissue scar allows the use of so-called “lightweight” meshes (Vipro, Vipro-2, Ultrapro), that is, meshes with a reduced amount of polypropylene per unit area of the prosthesis, which reduces the intensity of the inflammatory reaction. Currently, polypropylene meshes PMS (6-11 cm), PMM (15-15 cm), PML (30-30 cm), PMH, produced by are widely used; polypropylene mesh SPMM-35 (7 13 cm), SPMM-66 (15 15 cm), SPMM-135 (22 33 cm), produced by the TYCO corporation, as well as monofilament polypropylene mesh produced by St. Petersburg. [22] Use of other synthetic materials materials is undesirable, since it increases the risk of chronic infection of the prosthesis, which inevitably requires its complete removal.
About 1 million mesh implants for hernia repair are used annually in the world. In some countries, up to 90% of all hernias are operated on using polypropylene mesh prostheses.[22]
Among the methods of prosthetic hernioplasty, two large groups can be distinguished: “tension-free” methods and combined ones. The essence of tension-free repair is to use the patient’s own tissues to close the hernia defect without complete adaptation (contact) of the edges of the hernia defect in combination with a mesh prosthesis. In this case, the grid can be placed and fixed in various ways, according to the onlay, inlay, online+inlay, sublay principles. With combined prosthetic plasty, the hernia defect is eliminated completely by local tissues, by matching and layer-by-layer complete adaptation of its edges (tension plasty), due to which the normal topographic-anatomical structure of the abdominal wall and its function is restored, and is additionally strengthened by a prosthesis, which can be positioned according to the on-lay principle or sublay. Based on the above, many herniologist surgeons call tension plasty radical, and non-tension plasty palliative. However, a complete, layer-by-layer comparison of the topographic-anatomical structure of the abdominal wall in extensive and giant hernias, unfortunately, is not always possible.
Non-tension methods of prosthetic hernioplasty
The essence is plastic surgery of the hernial orifice with exogenous material without any adaptation of the edges of the defect. There are a large number of different methods of tension-free hernioplasty, differing both in the methods of placing the prosthesis and in the methods of their fixation. The main methods of tension-free hernioplasty:
- over the muscular aponeurotic frame (or the second name is “onlay”): with this type of plastic surgery, the defect in the aponeurosis is closed edge to edge, an endoprosthesis is placed on the suture, after peeling off 4-6 cm in different directions of the subcutaneous fatty tissue, and sutured to aponeurosis;
- under the muscular aponeurotic frame (retromuscular, preperitoneal, another name is “sublay”): with this method, after fixing the prosthesis to the peritoneum, the opened sheaths of the rectus abdominis muscles are sutured together edge to edge;
- With the “inlay” technique, hernioplasty of the abdominal wall is performed with an endoprosthesis without covering it with aponeurosis tissue. This can only be done in cases where it is impossible and dangerous to compare the edges of the hernial orifice due to the risk of developing compartment syndrome.
In the nineties, various methods were proposed for the repair of giant hernias:
- In 1990, the Ramirez method appeared, which consisted of dissecting the aponeurosis of the external oblique muscle on both sides, which is necessary to reduce the hernial orifice.
- In 1996, the Devlin method appeared, in which the mesh graft is placed and fixed using the “onlay” method, while it is necessary to achieve minimal tension on the edges of the hernia defect.[12]
Combined methods of prosthetic hernioplasty
In cases of using “combined methods” of plastic surgery, closure of the hernial defect includes one of the above methods of aponeurotic plastic surgery using only local tissue, and the prosthesis is fixed above or below the aponeurosis. The choice of one or another plastic method is made by the surgeon individually, depending on the type and size of the hernia, the condition of the local tissues, the patient’s age and the presence of concomitant pathology.
Based on the experience of surgical treatment of 188 patients with extensive and giant hernias, V.G. Lubyansky et al. (2008) found that patients before surgery had dysfunction of the abdominal-caval pump associated with destruction of the anterior abdominal wall and decreased mobility of the dome of the diaphragm. Part of the intestine is located outside the abdominal cavity. All this causes low intra-abdominal pressure, which, in turn, leads to obstructive and restrictive lung diseases. When reconstructing the anterior abdominal wall, the work of the abdominal-caval pump is restored, this ensures an increase in the speed of venous blood flow in the femoral vein and is the basis for the prevention of thromboembolic complications.
The above determines the advantage of using combined methods of prosthetic hernioplasty of ventral hernias over non-tension hernias, which consists in eliminating the preoperative pathological relative position of the anatomical structures of the anterior abdominal wall and restoring the physiological properties of the abdominal press. To prevent inhibition of intestinal motility, elevation of the diaphragm and displacement of the chest organs, which can lead to disruption of cardiac activity, breathing and the development of abdominal compartment syndrome, clear indications for one or another type of operation are determined. Of particular importance is the preoperative preparation of patients and timely prevention of cardiopulmonary complications in the early postoperative period. According to V.N. Egieva and D.V. Chizhova (2004), the use of combined plastic surgery results in up to 20% of disease relapses.[22] Most domestic and foreign authors note from 15 to 35% of relapses during prosthetic hernioplasty of extensive and giant PIH.
Endovideosurgical techniques for prosthetic hernioplasty
New horizons in herniosurgery are opened by minimally invasive laparoscopic techniques, which make it possible to eliminate many of the disadvantages of traditional hernioplasty. A revolution in hernioplasty in 1993 was made by Karl LeBlanc, who proposed a new method of laparoscopic hernioplasty, in which a mesh endoprosthesis was installed intraperitoneally and its fixation was carried out laparoscopically. This tactic in the world literature is called IPOM (intraperitoneal onlay mesh). The IPOM technique involves closing the hernia defect using special mesh endoprostheses, the distinctive feature of which is a two-layer structure. One side of the mesh is coated with a special solution that does not cause adhesion upon contact with internal organs, the second, on the contrary, has adhesive properties in order to connect with the peritoneum as firmly as possible. The mesh is suspended using non-absorbable ligatures in the abdominal cavity and fixed around the perimeter using tackers. The original LeBlanc technique had metal tackers. However, with the classical IPOM technique, the risk of the formation of postoperative seromas and granulomas of the hernial sac increases, so this technique is modified.
Advanced techniques in surgery of umbilical and ventral hernias with the Ventralex ST endoprosthesis
To perform an operation using this technology, an umbilical or ventral hernia must not have been previously operated on and the hernia orifice size must not exceed 6 square meters. see. Surgical intervention is performed through a small herniotomy incision and another additional trocar access of 5 mm. Under endotracheal anesthesia, a 5 mm trocar is installed on the left flank. Afterwards, a herniotomy incision of up to 1.5-2 cm is made in the area of the protrusion and the hernial sac with its contents is resected. Removing the contents of the hernial sac is safe, since laparoscopy was performed before and it was found that there is no risk of damage to internal organs. The Ventralex endoprosthesis is inserted into the abdominal cavity, resembling a mushroom in shape, which, as mentioned earlier, has two surfaces - a fixing and a protective one. After installation of the Ventralex endoprosthesis, laparoscopy is performed again to check the quality of the installation of the prosthesis. Afterwards, several skin sutures are applied, and the operation is completed.
Treatment of umbilical and ventral hernias using this method has a number of advantages:
- minimal trauma;
- duration of intervention - 15-20 minutes;
- there is virtually no pain after surgery;
- rapid rehabilitation (discharge from hospital after 24-48 hours);
- pronounced cosmetic effect.
According to many authors, the rate of complications after laparoscopic hernioplasty ranges from 2 to 26%, and the rate of relapse of the disease varies from 0 to 17%. One of the main concerns when using laparoscopy to treat PIH is the presence of a prolonged adhesive process in the abdominal cavity. When installing ports, there is a high probability of damage to the abdominal organs involved in the adhesive process.
Operations for postoperative hernia
The purpose of the intervention is to excise the hernia formation and postoperative scar, return the anatomically normal position to the internal organs and strengthen the peritoneum with a synthetic implant. This intervention requires a lot of experience from the doctor, and GMS Hospital employs just such surgeons - competent, with excellent command of modern surgical techniques.
Treatment of postoperative hernia at GMS Hospital
At the GMS Hospital hernia treatment center, advanced hernia repair methods are used for the treatment of postoperative hernias - tension-free repair with mesh implants. The use of endoscopic techniques and materials from leading manufacturers ensures maximum therapeutic results and a speedy recovery. When choosing an intervention technique, our doctors consider all factors - the type, location, size of the hernia, general health, the presence of complications and concomitant diseases, and only after a thorough analysis they select the most effective intervention tactics.
There is no need to risk your health and try to cure a hernia using traditional methods - make an appointment with a GMS Hospital surgeon by phone or online and get a detailed consultation with a leading specialist who will tell you everything about the disease and its treatment method.
Do you want to get rid of a hernia quickly and permanently?
You're lucky to have found us. Contact us for advice.
- We will conduct an in-depth diagnosis of the condition of your abdominal cavity
- We will select for you the optimal treatment method from the entire range of modern high-tech surgical techniques
- Our highly qualified specialists - candidates and doctors of medical sciences - will perform the operation using the latest technologies, expensive specialized equipment and materials
- Your stomach will become healthy and beautiful, and traces of the intervention will be completely invisible to prying eyes
- We will carry out follow-up examinations and monitor your abdominal condition for six months to ensure there is no recurrence (free of charge)