- HIV infection
- Causes of AIDS
- How is AIDS not transmitted?
- Pathogenesis
- Symptoms of AIDS
- Forms of flow
- Pulmonary
- Gastrointestinal
- Cerebral
- Disseminated
- Undifferentiated
- Complications of AIDS
- Diagnostics
- AIDS treatment
- Prognosis and prevention
Acquired immunodeficiency syndrome - AIDS, the “plague of the 20th century” - was first identified in the 1980s in the United States. Then cases of death of young men due to pneumonia were recorded. More than 35 million people with AIDS are registered in the world.
HIV infection
AIDS - acquired immunodeficiency syndrome - is a consequence of the development of HIV infection, one of its main markers and is manifested by complete suppression of the immune system. The condition occurs approximately 5 years after infection. Any disease that occurs against the background of HIV can be fatal. Diagnostics is aimed at identifying HIV infection, checking the number of immunocompetent cells and antibodies to the virus. The goal of therapy is to suppress the pathogen through the use of antiviral drugs. It is mandatory to eliminate bacteria, fungi, and viruses that provoke the development of secondary pathologies.
Life expectancy and causes of death
Life expectancy from detection of HIV infection to death is approximately 9-11 years. This period depends on the treatment, the patient’s lifestyle, and early diagnosis. If the infection is detected early and the patient receives HAART, life expectancy is estimated at 20-50 years. Without treatment, patients live 6-19 months from the moment of AIDS diagnosis; most often, death occurs within a year. The use of HAART extends this period by several years.
Death occurs from opportunistic diseases and tumors. Over the past decade, the number of deaths among HIV-positive people from causes unrelated to AIDS has been increasing. With high-quality therapy, a person can be a carrier of a pathogen for decades, but not experience AIDS.
Causes of AIDS
Human immunodeficiency virus (HIV) is a type of retrovirus. It is found in blood, sweat, vaginal secretions, semen, breast milk, and tears. The infection is transmitted intravenously, from mother to fetus, or sexually. You can become infected with HIV from medical instruments (syringes, etc.) that are used multiple times, during blood transfusions, or when applying tattoos and piercings.
The risk group includes people who have been infected with HIV for more than 5 years, who do not receive proper treatment, injection drug users, pregnant women, people living in unfavorable conditions, people
Similar names do not always have the same meaning
HIV is the human immunodeficiency virus. It can be asymptomatic for a long time, but during periods of exacerbation the manifestations are quite powerful. The difference between HIV and AIDS is that with the former you can live an almost full life, but with its final stage, immunodeficiency syndrome, this becomes impossible. Any infection can cause quick death.
Modern medicine can prolong the life of a person who has been diagnosed with an immunodeficiency virus, provided that they consult a doctor in a timely manner. But the danger is that the patient may not know for a long time that there are damaging cells in his blood, which means he does not get tested for this virus, and therefore will not receive help on time.
Pathogenesis
AIDS provokes a gradual decrease in the population of T-lymphocytes (they recognize cells with foreign antigens and play an important role in the acquired immune response), which is caused by a direct cytolytic effect and activation of apoptosis (the process of cell death) in T-helper cells. Leads to deactivation and depletion of the immune pool. HIV infection provokes the destruction of nerve cells and has a toxic effect on neurons. Against the background of decreased immunity, persistent (constantly present) infections are activated. Due to the lack of the necessary response of immunocompetent cells, active reproduction and generalization of the infection occurs.
What is immune status?
Immune status is a complex indicator demonstrating the general condition of the immune system. It reflects the activity of the immune organs and the cells they produce to protect the body.
To study the state of immunity, a clinical laboratory study is carried out, which includes collecting the patient’s medical history and a clinical blood test.
Carrying out tests to detect bacteria and virus carriage.
After receiving preliminary information, an immunogram is performed - tests of an approximate level, allowing to identify gross disturbances in the functioning of the immune system. Carrying out tests involves obtaining the following information:
- Lymphocyte count.
- Phagocytic (capturing) activity of leukocytes.
- Quantity and quality of T- and B-cells.
- Immunoglobulin concentration.
The data obtained are examined using fluorescent sera sensitive to CD antigens - surface antigenic markers. CD antigens are specific proteins that function as receptors and substances responsible for the interaction of immune system cells with each other.
At the moment, about 350 CD antigens are known and their list continues to grow. But for monitoring HIV infection, CD4+ and CD8 antigens associated with T lymphocytes are of interest. Their number determines a person's HIV status.
Symptoms of AIDS
From the moment of HIV infection to the first manifestations of acquired immunodeficiency syndrome, years and sometimes decades pass. The patient's condition begins to deteriorate due to the development of other diseases. One of the manifestations is a persistently elevated body temperature, which is accompanied by night chills, flashes of sweat (mainly at night), and a state of delirium. Blue-red nodes, characterized by pain, appear on the lower extremities, oral mucosa, and face (Kaposi's sarcoma).
White cheesy deposits of candida nature may appear on the surface of the mucous membrane and on the skin. There may be difficulty swallowing, a burning sensation in the mouth and a “lump” in the throat, pain in the chest area. There are traces in the form of herpes zoster, vesicles, the condition is accompanied by severe pain, rashes in the form of blisters. The patient complains of lack of appetite, diarrhea, and weight loss is observed - up to 10% of weight in a short period of time.
If the lung tissue is damaged, there is a strong dry cough and shortness of breath. Sometimes among the first symptoms of AIDS are manifestations of damage to the central nervous system: forgetfulness, dementia, severe headaches, decreased concentration, paralysis. Forms of flow
With acquired immunodeficiency syndrome, the patient is easily infected with other infectious diseases. Against the background of reduced immunity, fungi and bacteria spread. Tumors of the skin and internal organs may develop. The manifestation of AIDS differs depending on the clinical form.
Why is acquired syndrome dangerous?
A cure for HIV infection is not considered possible and thus requires lifelong drug treatment. The body itself cannot defeat it. After infection, the virus gradually destroys immune cells, opening the way for all other diseases. Because of this, carriers of HIV infection die from even the most banal ailments, such as a cold. Violation of social adaptation is also a serious problem for HIV-positive people. Society is only learning to perceive such people as equal and safe. Having learned about their status, people often commit suicide.
Until the terminal stage, associated infections respond well to treatment. But in the last phase, the drugs are no longer effective. Most often, patients have to deal with fungal, protozoal and bacterial infections and neoplasms.
Bacterial infections
Infection with bacteria is a very common phenomenon among carriers of the virus. Some of the bacteria are in our body, and some are found in large quantities around us. A healthy body can easily cope with them, but with AIDS, the immune system cannot control the development and influence of bacteria.
Localization of lesions:
- Leather. These are the most common infections for HIV-positive women and men. The main pathogens: Staphylococcus aureus, mycobacteria, Pseudomonas aeruginosa.
- Respiratory system. Tuberculosis and pneumonia are frequent “companions” of HIV. Bacterial lung infections are most common in children. The course is normal: fever, cough, moist wheezing. In the later stages of AIDS, the clinic is burdened by the combination of several infections.
- Gastrointestinal tract. Sometimes infection of the gastrointestinal tract occurs even before serious immunodeficiency. Patients are faced with salmonellosis, campylobacteriosis, and dysentery.
- Oral cavity. Periodontal disease is also common in patients with immunodeficiency. The most common diagnoses are gingivitis, stomatitis, ulcerative periodontitis, and tissue necrosis. In the absence of prevention and treatment, pathologies in the oral cavity progress rapidly.
Depending on the patient’s lifestyle and the quality of treatment, such infections may not occur or quickly disappear.
Lack of therapy leads to the fact that bacterial damage to one organ can spread to others. For example, with an oral infection, pathogens quickly spread to the gastrointestinal tract.
Fungal diseases
Among fungal infections for HIV-positive people, candidiasis, rubrophytia, lichen versicolor, and histoplasmosis are of greatest importance. The course and localization are different; in most cases, such infections recur, but are treatable.
AIDS diseases caused by fungi:
- Lichen versicolor (pityriasis versicolor) is a rash with thickening of the skin, affecting large areas of the body.
- Pneumocystis pneumonia caused by fungi. As a rule, it proceeds typically with fever, sputum production, and a lingering cough. She is being treated as an inpatient.
- Coccidioidosis is infection of the lungs by spores from the air. It manifests itself on the skin by the appearance of papules, plaques, ulcers, nodes, and fistulas. Patients need long-term prophylaxis with antimycotics.
- Rubrophytia - damage to the skin of the feet, legs, palms, and groin area. Blue spots with scales on the surface appear on the body.
- Candidiasis affects any part of the mucous membrane. Most often it manifests itself as candidal stomatitis in the mouth, genitals, and intestines. It is characterized by the appearance of a white coating with an unpleasant odor; in advanced forms, the development of ulcers and erosions.
- Cryptococcosis is a fungal disease with rashes on the skin and hair. At the first stages it resembles acne, then nodes form and unite. HIV-positive people are characterized by damage to the membranes of the brain, organs of the urinary system, and skin. For prophylaxis, itraconazole or fluconazole is prescribed for life.
Slightly less common at different stages of HIV is sporotrichosis caused by a dimorphic fungus. Infection occurs when scratched by thorns, thorns, or sharp plant stems. When the number of T cells is below 200, North American blastomycosis is characteristic. In the clinic: the appearance of nodes and plaques with the formation of scars. Localized on the face, skin of the torso, arms.
Viral infections
The influence of viruses affects the condition of the skin and mucous membranes. People with reduced immunity are most often faced with herpes zoster, genital warts, molluscum contagiosum, and hairy leukoplakia.
Infection occurs through contact with contaminated objects or the patient’s skin; damaged epidermis increases the risk of virus penetration.
Viral infections manifest themselves in the form of a rash, formations on the skin of different shades, white and gray spots in the mouth, and subcutaneous nodes. HIV-positive people should immediately consult a doctor if there are any changes on the body or mucous membranes. Treatment is usually long-term with the use of medications, compresses, diet and additional procedures.
Protozoal infections
Protozoal infections are infections caused by protozoan parasites. These microorganisms can only exist in the host and do not exist outside the “host” organism. AIDS-associated protozoal diseases:
- cryptosporidiosis;
- isosporosis;
- toxoplasmosis;
- microsporidiosis.
Infection is possible through sexual intercourse, cuts and exposure to infected fluid. All protozoal infections proceed in approximately the same way: prolonged diarrhea, abdominal pain, vomiting and nausea, weight loss. With toxoplasmosis - damage to the lymph nodes and mucous membranes of the eyes.
Tumors and other diseases
The human body with AIDS is also unable to control malignant and benign tumors. The most important is Kaposi's sarcoma, in which dark formations appear on any part of the body and internal organs. The second place in frequency is occupied by lymphomas; they are localized in the lymph nodes and internal organs. Outside the lymph nodes, the central nervous system and gastrointestinal tract are most often affected. Rarely, lymphoma affects the salivary glands, eyes, and lungs.
Women develop cervical cancer, most often carcinoma. Men who become infected through anal sex with men are diagnosed with anal carcinoma.
Tumors with reduced immunity are difficult to treat, but high-quality therapy helps curb the progress of the disease.
Patients can develop cancer in absolutely any part of the body. According to the latest WHO data, in developing countries, 4 out of 10 people infected are diagnosed with cancer. But the use of HAART and chemotherapy reduces this risk.
Forms of flow
Pulmonary
The most common form of AIDS, present in 50%-80% of adult patients and children. Accompanied by various forms of pneumonia, fever, severe cough, shortness of breath, chest pain. The condition causes oxygen starvation. X-ray shows scattered pulmonary infiltrates. Sometimes pneumonia is accompanied by respiratory failure, intoxication, and tuberculosis may occur. Treatment is carried out according to a complex scheme, which is built in accordance with the patient’s condition.
Gastrointestinal
The second most common form, which affects the intestines. The patient complains of prolonged diarrhea or obstruction, painful swallowing, and chest pain. The gastrointestinal tract is affected not only by associated infections, but also by the HIV pathogen itself. Changes occur not only in housing and communal services, but also in the liver and kidneys. Manifested by stomatitis, colitis, isosporosis, salmonellosis. The main risk is critical weight loss.
Cerebral
A form of HIV infection occurs in 15-20% of patients. NeuroAIDS is characterized by secondary damage to the central nervous system. Brain abscess, meningitis, encephalitis, and multifocal leukoencephalopathy develop. Damage to the central nervous system causes changes in cognitive abilities, behavior, and memory. There is a change in coordination of movements, lethargy, the presence of anxiety, irritation to bright light and loud music. In severe forms, dementia and schizoid manifestations may develop, and in some cases, HIV contributes to the formation of a brain tumor.
Disseminated
Develops in approximately 30% of AIDS cases. It manifests itself as tumors of the skin and mucous membrane, most of the formations are related to Kaposi's sarcoma. A small percentage of HIV-infected people are faced with a malignant tumor - B-cell lymphoma.
Undifferentiated
Clinical form, the etiology of which remains unclear. It manifests itself as prolonged diarrhea, asthenia, lymphadenopathy, purulent foci, and elevated temperature for months. A complex of AIDS-associated symptoms is observed.
What is HIV and how does it manifest itself?
People first started talking about HIV infection in the 80s of the twentieth century, but earlier cases of similar diseases can be found in historical documents.
The virus is believed to have come from central Africa during an intense migration.
The virus belongs to the family of so-called “slow” viruses. The fact is that many years can pass from the moment of infection to the appearance of the first symptoms (about 50% of infected people do not know that they are infected for about 10 years). The mechanism of infection begins from the moment the virus enters the blood. Having found the cells responsible for immunity, the virus adheres to them. The immune system is unable to effectively fight back against foreign substances, sometimes due to the variability of the virus, when cells simply cannot recognize it. The disease begins to progress, affecting more and more lymphocytes, and eventually there are so few of them left that HIV turns into AIDS. A condition in which the number of lymphocytes is less than 200 per 1 ml of blood is considered the beginning of the last stage of immunodeficiency; the body can no longer produce the required number of immune cells and becomes vulnerable to any infection.
There are several stages of the immunodeficiency virus disease:
- Incubation period. This is the time when the virus has just entered the body. It can occur without any symptoms or with flu-like symptoms. The duration of this period can be short, or it can last up to six months;
- Acute manifestations of infection. The patient may begin to get sick with encephalitis and fever. However, this is not observed in everyone; there may be no symptoms at this stage;
- The next stage is called latent. At the same time, not a single symptom will indicate the presence of the virus; only an HIV test can show its presence;
- The last stage when HIV turns into AIDS. At this time, the body is no longer able to resist any diseases. Infection with fungal and viral infections, as well as oncology, leads to the death of the patient.
Complications of AIDS
People with acquired immunodeficiency syndrome are at risk of developing tuberculosis. Most of these patients have a generalized form of tuberculosis, which can lead to death and disability. Up to 90% of AIDS patients suffer from Pneumocystis pneumonia, and 10% have damage to the central nervous system. Up to 23% of cases of tuberculous meningoencephalitis are registered.
All HIV-infected people are at risk of developing candidal pharyngitis, regardless of the stage of the disease. A tenth of patients have a fungal infection of the esophagus; the patient’s condition worsens due to a decrease in T-helper cells.
Immunity Destroyer
In 1983, the virus that causes AIDS was independently isolated by several laboratories. At the Pasteur Institute (France), a group of specialists led by Luc Montagnier named LAV (lymphadenopathy-associated virus), and scientists at the National Cancer Institute (USA) discovered a virus in an AIDS patient, which they classified as a human T-lymphotropic virus (HTLV). They later announced that the retrovirus they discovered, HTLV-III, was most likely the cause of AIDS and was identical to the LAV virus. In 1986, it became clear that HTLV-III and LAV were the same virus. In 1984, scientists at the University of California also isolated what they called an AIDS-associated retrovirus from patients.
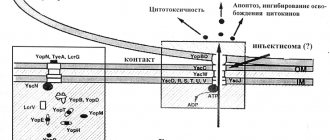
Structure of the HIV virion
Image:
In 1984, scientists were confident that LAV (or HIV) was the causative agent of AIDS. Evidence of a link between HIV and AIDS was that the virus was always isolated from patients with AIDS or even before they developed immunodeficiency. The researchers successfully cultured the pathogen on activated T lymphocytes expressing the CD4 glycoprotein that were killed by the virus, and even characterized its genome, which turned out to be longer than the retroviral genomes known at that time.
Diagnostics
The diagnosis of AIDS is made after consultation with an infectious disease specialist. If there are concomitant diseases, other medical specialists are involved. Patients with HIV infection are mostly advised by phthisiatricians. The following methods are used to diagnose the disease:
- Physical. A medical examination is aimed at identifying signs of the disease, in particular, the growth of lymph nodes, changes in behavior, rashes on the mucous membranes and skin. Rhythm disturbances and noises may be heard in the heart, and snoring in the lungs. White plaque may be present in the oral cavity.
- Ophthalmological. Signs of the disease are retinal necrosis, precipitates in the anterior chamber, and nerve atrophy. The patient complains of decreased sharpness and the formation of spots before the eyes.
- Laboratory. Shows the main manifestations of immunodeficiency: thrombocytopenia, anemia, leukopenia, lymphopenia. Clinical urine analysis shows proteinuria, lipiduria. The screening method allows you to determine the immune blot. PCR testing is used to identify antigens.
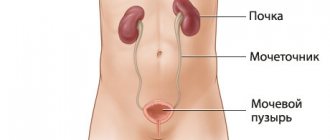
- Instrumental. Includes chest x-ray, MSCT, MRI of the brain and mediastinal tomography. For all patients with HIV, ultrasound of the kidneys, abdomen, and pelvis is recommended.
- Differential diagnosis. It is carried out in the presence of clinical symptoms. Skin manifestations are similar to those of allergic dermatitis, syphilis, and herpes zoster. Enlarged lymph nodes are detected with tuberculosis and brucellosis.
Signs of the syndrome
It is impossible to distinguish the first symptoms of AIDS. All precursors of the disease relate to HIV infection. During the incubation period, the virus may not manifest itself in any way; sometimes a person develops symptoms characteristic of the disease. These are fever, weakness, loss of appetite, swollen lymph nodes, pink skin rash, diarrhea.
Sometimes the asymptomatic course persists for many years. But the pathogen can be identified 3 months after infection by analysis. As viral copies multiply and the immune system is suppressed, more and more obvious signs of illness occur. A distinctive feature of HIV/AIDS is enlarged lymph nodes; this condition can last for several months. Patients experience migraines, pain in the hypochondrium, and fever. Conventional medications do not help much in this condition.
AIDS is differentiated from HIV infection according to several criteria: the patient’s condition, the number of T-helper cells and viral load. Normally, a person has from 500 to 1600 T-helper cells, even in a healthy person their number varies and depends on many factors. In HIV-positive people, their number gradually decreases with temporary plateaus. When the analysis shows 350 or fewer cells, prevention of diseases associated with immunodeficiency syndrome is prescribed.
AIDS is often accompanied by the following symptoms:
- weight loss;
- apathy and powerlessness;
- prolonged diarrhea;
- cough;
- forgetfulness, confusion, disorientation;
- painful or difficult swallowing;
- enlarged lymph nodes;
- fever.
Against the background of a severely weakened immune system, the body can no longer control opportunistic bacteria and fungi, which are the natural microflora of humans. In the terminal stages, patients face tuberculosis, Pneumocystis pneumonia, cancer, bacterial cardiomyopathy, and lymphoma.
AIDS treatment
The advisability of treatment in a hospital will be determined by the patient’s condition. Hospitalization in highly specialized medical institutions is possible: oncology and tuberculosis dispensaries. In some cases, hospitalization in intensive care is necessary. For concomitant diseases, such as hepatitis, diabetes, a patient with symptoms of AIDS is prescribed a diet. Bed rest is necessary for prolonged fever.
Etiotropic antiretroviral drugs prevent the progression of HIV infection. The action is aimed at reducing the amount of virus in the blood. Antiviral, antifungal and antibacterial agents are used to treat concomitant infections. If indicated, radiation and chemotherapy are performed; surgery may be required. To relieve symptoms, medications are taken to reduce fever, detoxification, and vasoprotective agents.
WHO activities
The World Health Assembly, at its sixty-ninth session, endorsed the new Global Health Sector Strategy on HIV 2016–2021. The Strategy includes five strategic directions to guide countries and WHO in their priority actions over the next six years.
These are the following strategic directions:
- information for targeted actions (understanding the scale of the epidemic and combating it);
- interventions to achieve impact (covering the full range of services needed);
- providing services in an equitable manner (reaching groups in need of services);
- financing for sustainability (financing the costs of providing services);
- innovation for acceleration (future-oriented).
WHO is one of the sponsors of the Joint United Nations Program on AIDS (UNAIDS). Within UNAIDS, WHO leads work on HIV treatment and care and co-infection with HIV and tuberculosis, and coordinates with UNICEF efforts to eliminate mother-to-child transmission of HIV.
Prognosis and prevention
The prognosis will depend on the timeliness of detection of HIV and opportunistic pathologies. With the help of antiretroviral drugs it will be possible to prevent the appearance of systemic forms. With HIV infection, tuberculosis leads to death in 50% of cases, toxoplasmosis and pneumystosis - in 17%, CMV infection (cytomegalovirus infection) - in 15%. Other conditions are less likely to cause mortality. If an opportunistic pathology (except tuberculosis) is detected, patients are prescribed two-week antiretroviral therapy.
Work is underway to create a vaccine that prevents HIV infection, but the main difficulty lies in the constant mutation of the virus. As nonspecific preventive measures, it is recommended to abstain from unprotected sexual intercourse (sexual intercourse without a condom) and drug use. At the state level, it is required to introduce educational programs related to HIV infection, disseminate information through the media and social events.
GLOBAL HIV STATISTICS
The first cases of infection were recorded in the 80s of the last century in the United States in gay men. Epidemiologists agree that the virus originates in Africa[1]. Today it has spread throughout the planet. Global statistics showed that during the year the number of new cases of HIV infection was 1.7 (1.2-2.2) million (2019) The number of people who died from AIDS-related diseases was 690,000 (500,000-970,000 ) Human. (2019) 75.7 (55.9–100) million people have become infected with HIV since the beginning of the epidemic. (2019). 32.7 (24.8–42.2) million people have died from AIDS-related illnesses since the beginning of the epidemic. (2019) In total, since the beginning of the epidemic, the number of deaths at the terminal stage is about 35 million people.
Thanks to the global expansion of access to antiretroviral therapy for people living with HIV, mortality from the syndrome has decreased by 51% compared to 2004. The number of new HIV infections has fallen by 40% since its peak in 1998. The number of new HIV infections has fallen to 1.7 (1.2–2.2) million in 2021, down from 2.8 (2.0–3.7) million in 1998. Despite the positive downward trend, global statistics indicate that 7,000 young women aged 15–24 years are infected every week.
The risk of contracting HIV is: – 26 times higher among men who have sex with men; – 29 times higher among injection drug users; – 30 times higher among people working in the sex industry; – 13 times higher among transgender people. Most of the infected are concentrated in Central and Southern Africa. The increase in patients continues to be greatest in Eastern Europe and Asia.